Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
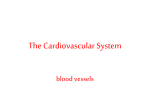
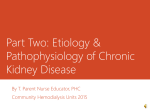
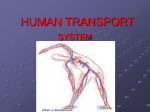
Hypertensive Retinopathy Caliber Changes in Retinal Blood Vessels Following Blood-Pressure Reduction and Inhalation of Oxygen By P. S. RAMALHO, PH.D., M.D., AND C. T. DOLLERY, M.B., M.R.C.P. Downloaded from http://circ.ahajournals.org/ by guest on June 17, 2017 SUMMARY Caliber changes in retinal vessels of groups of hypertensive patients were measured after the blood pressure had been lowered by successful renal surgery, posture with adrenergic blocking drugs, and parenteral hydralazine. The small arterioles dilated when the pressure was reduced, whatever means were used. Larger arterioles dilated in three younger hypertensive patients but in the remainder they were unchanged or narrowed by pressure reduction. Inhalation of oxygen constricts normal retinal arterioles but the response in hypertensive patients was much less. A response to oxygen was restored in some small arterioles that dilated when the blood pressure was lowered. As retinal arterioles have no adrenergic vasomotor supply, changes in their caliber probably occur because of autoregulation. Narrowing caused by autoregulation during a rise in systemic arterial pressure may become irreversible in long-standing hypertension because of structural changes in the vessel wall. Additional Indexing Words: Retinal circulation Arteriolar reactivity NARROWING of the retinal arterioles in hypertension has been described for many years.' 2 In 1914, Volhard and Fahr3 gave the name "angiospastic retinopathy" to the changes that occur in this condition. The retinal appearances in hypertension are particularly important because they correlate better than any other single factor with the prognosis of the untreated disease.4 Advances in drug treatment have allowed hypotensive therapy to be used in many patients who are not acutely ill with accelerated forms of the disease. The purpose of treatment in patients with mild disease is to prevent late vascular complications that now account for most of the morbidity and mortality. This type of treatment is based on the assumption that reduction of blood pressure will prevent or even reverse vascular complications of hypertensive disease. Renal hypertension Retinal vessels are the only ones in the body that are readily accessible to direct and repeated examination in life. Their caliber can be measured from well-focused retinal photographs.5 In this study caliber measurements from retinal photographs have been used to assess the response of the retinal arterioles of hypertensive patients to a number of different methods of lowering the blood pressure. Inhalation of oxygen at 1 atmosphere pressure has been used as an alternative method of assessing the vascular reactivity of retinal blood vessels in hypertensive patients because it is known that oxygen causes severe vasoconstriction in normal retinal vessels and the response is reduced in hypertension.6, 7 Methods Retinal photographs were taken with a Carl Zeiss retinal camera with Kodachrome IH film. The pupil was dilated with 0.5% cyclopentolate and 10% phenylephrine. Two retinal cameras were available, one mounted horizontally and the other vertically, so that photographs could From the Department of Medicine, Royal Postgraduate Medical School, London, England. 580 Circulation, Volume XXXVII, April 1968 HYPERTENSIVE RETINOPATHY Downloaded from http://circ.ahajournals.org/ by guest on June 17, 2017 be taken in both the erect and supine positions. Blood pressure measurements were made with a standard sphygmomanometer. The studies with the use of oxygen were carried out with the patient breathing the gas from a Douglas bag through a low dead-space respiratory valve box. Photographs were taken between 5 and 15 minutes after beginning of oxygen breathing, when the lung was completely washed out with oxygen. Method of Caliber Measurement Retinal photographs were scrutinized after processing and all those with imperfect focus rejected. Even minor degrees of image blurring are unacceptable in this method. The drawing of the retinal vessels was made by projecting the color transparencies onto a sheet of paper. Pairs of pictures of different areas were selected, and their identity was concealed by a code number. Caliber measurements were made with a low-power microscope (x 30) with a screw micrometer eyepiece. The site of each measurement was identified with respect to vessel branches and crossings and was marked on a diagram. Where possible, 10 arterioles and 10 veins were measured in each patient studied. Care was taken that these represented the whole range of vessel sizes that could be measured. The largest vessels near the optic disk are about 120 microns in the normal eye, and the smallest that can be identified clearly enough to be measured are about 30 microns. The results in this paper have been expressed as arbitrary units, each of which represents 1.25 ,u in an eye of normal length.5 There is an error in the measurement of retinal vascular caliber by this method, even when five measurements are averaged at each site. The standard deviation of the mean value obtained in this way is 2 units and is independent of the diameter of the vessel measured. Because of this variability we have preferred to look at trends of caliber change either by calculating regression lines of caliber change against initial diameter or a paired t-test on the caliber changes in all the vessels measured in one individual. Results Response of Normal Retinal Vessels In the study of hypertensive patients we made use of changes in the inspired oxygen pressure and postural change as maneuvers to bring about changes in the caliber of retinal vessels. It was necessary first to establish the normal reaction of retinal vessels to these maneuvers. It is well known that retinal arterioles constrict in response to increases in Circulation, Volume XXXVII, April 1968 581 inspired oxygen pressure6' 7especially the smallest arterioles less than 50 microns in diameter.8 Previous data on the reactions of the smaller retinal arterioles in nornal subjects breathing oxygen were obtained in young men under the age of 35 years. As the hypertensive patients were usually older than this, studies were made in a group of normal subjects embracing a larger span of years. Effects of Breathing Oxygen at 1 Atmosphere Thirteen normal subjects with ages ranging from 19 to 62 years were studied while breathing air and oxygen at I atmosphere pressure. Retinal photographs were taken during air breathing and again after at least five minutes of oxygen breathing. One hundred and fifty-seven arterioles and 139 venules were measured at the same sites while breathing air and again while breathing oxygen. The average reduction of caliber for all arterioles was 13.5% and for all venules 16.3%. The arterioles measured ranged in size from 30 to 124 units and the veins from 35 to 171 units. Variations in the reactions in individual vessels were large. The smallest reduction in the caliber of an arteriole was 3.8% and the largest 22.6%. Similar figures for veins were 3.4% and 24.9%. When the average results for each individual were plotted against age there was clear evidence of a relationship. The older the individual was, the less the reduction in diameter with oxygen. A similar trend was evident in both arterioles and venules (fig. 1). Effects of Postural Change in Normal Subjects Six normal subjects, average age 28 years (range 21 to 36), were photographed in both the standing and lying positions. Their blood pressures were taken with a standard sphygmomanometer during photography. Seventy arterioles and 61 veins were measured on these photographs. Changes in diameter were measured against the initial diameter of each vessel when each subject was lying flat. Although there was a wide scatter of results, there was a small but significant tendency for the smallest arterioles to dilate and the largest ones to constrict when these subjects RAMALHO, DOLLERY 582 ARTERIOLES 30 20 0 c:) 0 b -0,355 10 0 *S y= 26,897'-0,355x CD) . a 0 I ~ 50~ 50 10 30 30 AGE (years) 10 CDN LI- C=: CC> VENULES 3 30 0 LU CL 0 20 Downloaded from http://circ.ahajournals.org/ by guest on June 17, 2017 u > i > 0 0 b == -0,4818 y 34,278-0,4818x 10 4 r '~ * 1 -1 10 50 30 AGE (years) Figure 1 Percentage changes in caliber of retinal arterioles and veins during oxygen breathing of 13 normals ranging in age from 19 to 62 years. moved from the recumbent to the upright position. There was also a change in the diameter of the veins, as all except the smallest showed a significant reduction in diameter on standing (fig. 2). The mean blood pressure, taken as the diastolic plus one third of the pulse pressure, rose from 85.5 mm in recumbency to 94 mm on standing. Cardiac output changes were not measured in this study (fig. 2). ference between normal and hypertensive subjects is not so great as it appears by eye and also because the major narrowing of arterioles takes place more peripherally than 15 _ n 01 -~ :-5 0. .* 1 15 DIAMETER WHEN ov-- Vascular Responses in Hypertensive Retinal Vessels Hypertensive vascular disease leads y=y4ID8B-007x ~~~~O-OkP< 0-02 I' . 10 _ t-2 4 Arterioles 0* - L : * 10 + 5_ 0 20 i40 H0 60 BPI8PSmmHgol-2- '100 t120 1140 BP 94 mmHg to nar- rowing, irregularity, and sclerosis of retinal arterioles. We attempted to derive an index of arteriolar narrowing by measuring the diameter of all veins and arterioles on the edge of the optic disk. Neither the crude ratio of the sum of arteriolar diameters over the sum of vein diameters nor the ratio of sums of squares of diameters gave a satisfactory separation between normal and hypertensive subjects. This may be partly because the dif- 15r_ 10 - +5 - Yenules . 0- -5 0 4 . 15 _- Figure 2 Caliber changes in retinal arterioles and veins of normal subjects on standing upright. Each point represents the change in diameter at a single point on an individual vessel. Circulation, Volume XXXVII, April 1968 HYPERTENSIVE RETINOPATHY 583 the disk edge. It is difficult to make such the more peripheral parts of the retina because of the variability of the vessel branching pattern. measurements in change in diameter during oxygen breathing arteriolar segments, even in patients with grade 3 or grade 4 hypertensive retinopathy, showed a significant constriction during oxygen breathing. some Effects of Oxygen Thirteen hypertensive patients ranging in age from 15 to 63 years and with mean blood pressure readings between 147 and 173 mm Hg were studied while breathing air and oxygen at 1 atmosphere pressure. One hundred twenty-seven arterioles and 142 venules measured. Reduction of caliber of arterioles produced by oxygen breathing was much less in the hypertensive than in the normal subjects with the same range of ages. In the hypertensive patients the reactivity was almost independent of age, except for the youngest patient (table 1). The over-all percentage reduction of arteriolar caliber was 3.3% (normal 13.5%). The reaction of veins to oxygen breathing was much less reduced than that of the arterioles. The over-all reduction in diameter averaged 11.6% (normal 16.3%). In five of the 13 hypertensive patients the caliber reduction of arterioles during oxygen breathing was not statistically significant but, surprisingly, these five subjects all showed a significant reduction in the diameter of the veins. Although there was little over-all were Effect of Pressure Changes on Caliber of Retinal Vessels in Hypertensive Patients Posture and Sympathetic Blockade Downloaded from http://circ.ahajournals.org/ by guest on June 17, 2017 Six treated hypertensive patients, average 48 years (range 35 to 53 years), were selected because they were known to have a substantial fall in pressure when they stood up. The mean arterial pressure of the group was 144.6 mm Hg in recumbency and 114.6 mm on standing. All were being treated with drugs that are known to interfere with transmission at some point on the sympathetic vasomotor pathway. Seventy arterioles and 51 venules were measured on photographs taken while the patient was lying down and again at the same sites while he was standing upright. The initial diameter of the arterioles ranged from 28.8 to 114 units and the veins from 38 to 158 units. A plot of the change in diameter against the initial diameter of arterioles in the recumbent position showed that there was a significant increase in the diameter of the smallest arteriole and a decrease in diameter of the larger ones (fig. 3). age Table Percentage Reduction of Diameter of Retinal Arterioles and Venules in Thirteen Hypertensive Patients While Breathing Oxygen Age Sex 15 20 31 33 46 47 F M M M M M M F M F M M M 52 53 57 58 60 62 63 Mean *P > 0.05. Circulation, Volume XXXVII, April 1968 Mean BP (mm Hg) 147 170 167 153 157 150 153 173 163 167 167 163 157 Grade of retinopathy4 2 2 3 3 4 4 3 3 3 3 3 3 3 Percentage change of diameter Venules Arterioles -12.0 - 2.9 - 1.5* - 3.7 + 1.1* - 1.8* 3.0 4.7 - 7.4 - 3.2 - 3.0 + 0.7* - - 1.5* - 3.31 -19.1 -16.9 -12.5 -16.3 - 3.3 -11.7 -15.1 - 7.5 -14.8 -11.1 -10.2 - 1.8 -10.4 -11.59 .X1~ -r A RAMALHO, DOLLERY 584 30 I Arterioles t:6 596 y= 13 33-0 263x 20 w 0 m * * = O ui DIAMETER WHEN c*--l-BP144-6mmHg 40 20 60 60 120 100 Venules 140 BP reduction 144 6-1146mmHg dv_I I - U- - . e1 w *.0. a -10 0 .10 3 CT _ 12 34'/o increase indiameter INITIAL DIAMETER '20 '40 I_ '60 B0 100 '120 a Venules a , * nI ll . * K 0 Mean BP --T 11'0 1160 reduction 168 -121 mmrnHg 20 :0 I._ a nI 30 C +10 U IL -1 0 y=13 565-012x . 6* -*. 9. .10 < 20 :. p<0o01 .0 '0 Arterioles .. 0 -10l I IL . *. . 0... 0 a. 13,48"/. increase in diameter Figure 4 Downloaded from http://circ.ahajournals.org/ by guest on June 17, 2017 Figure 3 Caliber change in retinal arterioles and veins of hypertensive patients on adrenergic blocking drugs, who had a large postural fall in blood pressure on standing. retinal arterioles and veins in Caliber changes hypertensive patients treated with parenteral hydralin azine. Effect of Surgery in Patients with Unilateral Renal Disease Effect of Hydralazine Sympathetic blocking drugs are thought to lower blood pressure on standing chiefly by preventing the normal adjustment of peripheral resistance that takes place when the cardiac output falls on standing. For comparison we selected a group of six severely hypertensive patients, average age 51 (range 36 to 66) years, who were to have treatment initiated with parenteral hydralazine, a drug that has -a direct vasodilator action on systemic arterioles. The drug was administered by slow intravenous injection (less than 1 mg/minute), while the patients were lying flat. The average of the mean blood pressures fell from 168 to 121 mm Hg after administration of an average dose of 37 mg of hydralazine intravenously. Sixty-one arterioles and 50 venules were measured. The response was different from that seen in patients taking sympathetic blocking drugs. Almost all arterioles dilated after administration of drugs and the average increase was 12.3%. Small caliber arterioles dilated to a greater extent than large ones. The venules also dilated but in this case the greatest increase in diameter occurred in the largest veins. The average increase in diameter in veins was 13.5% (fig. 4). The closest approach to a cure of hyper- tension is successful renal surgery. Eleven patients with unilateral renal disease were studied before and between 4 and 40 weeks after operation. Eight of the patients had stenosis of the main renal artery and one of a branch artery. The remaining two had hy- dronephrosis and a pyelonephritic kidney, respectively. Four of the patients had no significant change in their pressure after surgery and there was no significant change in the caliber of either arterioles or venules in their retinae. Five of the remaining patients had their blood pressure reduced to near normal levels and in two others it was significantly reduced from preoperative levels. All these patients showed dilatation of the .20 : CALO8E CAOMES AFTER RENAL SUtliEl Mm Arterieins . od.cd IW U1Rg 0 . tz tt el -e1 * 20 I*10-1-01941 p<r -2e 1 ; * _ ;w *1 i tR a *= Figure 5 Caliber changes in retinal arterioles of seven whose blood pressure was reduced by renal patients surgery. Circulation, Volume XXXVII, April 1968 HYPERTENSIVE RETINOPATHY 585 Hg before treatment and 98 mm Hg after treatment. CALIBRE CHANGES IN 3 YOUNG HYPERTENSIVES B. P 138 mmHg - 9 rmmHg CD I.- C.2 =2 LLJ C= LAJ C= tR 30 _ Arterioles . Response to Oxygen before and after Blood Pressure Reduction in Hypertensive Patients 20 CL. 10 .* * --x 1 cn .Iqc zi 10' - E e 0I *. X I 0 10 ZU 30 40 5U 6bO 2U 8U 9U0. 1UU ARTERIOLAR OIAMETER BEFORE TREATMENT 0 ." C.0 -= . . . Figure 6 Caliber changes in retinal arterioles of three young hypertensive patients who showed a general dilatation of arterioles. Downloaded from http://circ.ahajournals.org/ by guest on June 17, 2017 smallest retinal arterioles whereas the response of the larger arterioles was variable (fig. 5). General Increase in Arteriolar Caliber During this investigation we observed three young patients, average age 18 (range 15 to 21) years, who showed a general increase in arteriolar caliber when the blood pressure was reduced (fig. 6). In two instances the patients were treated with guanethidine and the third had a successful nephrectomy for renal artery stenosis (fig. 7). The average of the three mean blood pressures was 138 mm After blood pressure reduction many hypertensive patients in this study showed dilatation of some arterioles of small caliber. The vasoconstrictor response of these small vessels to oxygen was found to have increased after reduction of the blood pressure. In five hypertensive patients with retinopathy and high levels of blood pressure (mean pretreatment pressure 157 mm Hg) the reaction to oxygen breathing was studied in the sitting position before and after lowering the blood pressure to a value of 109 mm Hg for 2 to 6 weeks by treatment with adrenergic blocking drugs. These patients' retinal arterioles showed a similar change in caliber to that observed in patients treated by renal surgery or posture after adrenergic blockade (fig. 8). One patient had no increase in his response to oxygen after pressure reduction but in the remaining four there was a significant increase in the vasoconstrictor response. The unreactive patient showed a small reduction in the caliber of his arterioles when the Figure 7 Retinal photograph of patient J.M. aged 15 (left) before and (right) after nephrectomy. There is a general increase in the diameter of arterioles. Circulatioon, Volume XXXVII, April 1968 RAMALHO, DOLLERY 586 .- az a) .e E co -C' of blood pressure allowed the arterioles to dilate; this degree of dilatation could be reversed by oxygen breathing. CALIBRE CHANGES AFTER LONG TERM MEDICAL TREATMENT 20 Arterioles * +10 [ Jr CI a -?k-, a *- 0 S.. m0 -10 Mean BP reduction -159-114mmHg y= 10G69-02x )I 20 0 20 40 60 80 100 120 ORIGINAL DIAMETER BEFORE TREATMENT Figure 8 Caliber changes in retinal arterioles of five patients whose blood pressure was reduced by several weeks of treatment with adrenergic blocking drugs. Downloaded from http://circ.ahajournals.org/ by guest on June 17, 2017 blood pressure was reduced. The four with increased reactivity to oxygen had dilatation of their smaller blood vessels when blood pressure was lowered. Study of 13 individual arterioles, which dilated after pressure reduction, showed that the average diameter was 65 units before and 71.5 units after the blood pressure was lowered (table 2). There was no net change in diameter in response to oxygen before the pressure was lowered but average reduction in diameter of 5.4 units with oxygen after the blood pressure had been lowered and the vessels had dilated. Thus, reduction Discussion The retinal arterioles of hypertensive patients are often narrowed. Reversal of the narrowing by sustained and general increase in diameter following treatment was found in only a small group of younger patients. General arteriolar dilatation also occurred in patients given intravenous hydralazine, during the period of drug action, but some of the patients had retinal arterioles that appeared abnormally narrow even when the blood pressure was near normal levels. Other methods of lowering blood pressure such as the postural change with adrenergic blocking drugs or successful renal surgery more often brought about a small reduction in the diameter of the larger retinal arterioles than an increase. These patients were middleaged and had long-standing hypertension. The vasoconstrictor response to oxygen was much reduced in hypertensive patients and a similar although less striking reduction in reactivity occurred in older, normotensive persons. The loss of response may be due to structural changes in the arteriolar wall which are, at least in the short-term, iLrreversible. Table 2 Changes in Thirteen Arteriolar Segments Which Showed Increased Reactivity to Oxygen after Lowering the Blood Pressure with Adrerergic Blocking Drugs Initial diameter (units) Mean 37 40 42 43 30 115 56 74 40 81 38 38 42 52 Caliber changes on 100% oxygen +1 +1 0 +2 +1 0 -1 +1 -1 -2 +2 -1 -2 +0.08 Diameter after hypotensive treatment 39 51 48 49 42 125 59 76 44 82 43 41 45 57.3 Caliber changes on 100% oxygen after treatment -8 -8 -6 0 -7 -7 -5 -1 -1 -3 -5 -2 -3 -43 Circulation, Volume XXXVII, April 1968 HYPERTENSIVE RETINOPATHY Downloaded from http://circ.ahajournals.org/ by guest on June 17, 2017 The degree of vasodilatation to be expected with blood pressure reduction must depend on the degree of constriction that occurred when the blood pressure rose. It has not proved possible to derive a satisfactory quantitative expression of the degree of arteriolar narrowing, and this places a limitation upon the interpretations that can be made. The most consistent response was the dilatation of small arterioles when the blood pressure was lowered, whatever means were used. The change in transmural pressure in the retinal arterioles during some of these maneuvers was large. Blood flow through the eye is opposed by the intraocular pressure of 16 to 20 mm Hg and, in the erect position, by the hydrostatic height of the column of blood from heart to eye (also 16 to 20 mm Hg). A fall in mean arterial pressure from 144 mm in recumbency to 114 mm on standing is equivalent to a reduction of retinal arteriolar transmural pressure from 124 to 74 mm Hg, a fall of over 40%. There is strong evidence that retinal arterioles do not have an adrenergic nerve supply,9-11 so that there must be another mechanism controlling arteriolar diameter. Such a mechanism is autoregulation, which is known to play an important part in regulating flow through many other organs. It is difficult to find any other explanation for dilatation of small arterioles in the face of reduced blood pressure in such varied circumstances. These studies suggest an explanation for the widely varying degree of retinal arteriolar narrowing seen in different patients with comparable degrees of pressure elevation. If arteriolar narrowing is an autoregulatory response, the amount of narrowing will depend upon the height of the blood pressure and the capacity of the vessel to react. Unreactive vessels in older patients or patients with long-standing mild hypertension might constrict less for a given pressure elevation than the arterioles of a young patient with a rapid rise in blood pressure. Arterioles with a greater degree of constriction are more likely to show substantial vasodilatation when the pressure is lowered. Circulation, Volume XXXVII, April 1968 587 It is interesting to compare our studies of the human retina in hypertension with those of Byrom'2 in rats with experimental malignant hypertension. Byrom found that focal retinal arteriolar constriction in rats during the early stages of malignant hypertension could be reversed by deepening the level of ether anesthesia. In animals with long-standing hypertension this maneuver did not result in vasodilatation, although removing the renal clip that had caused the hypertension reversed the changes. These results are comparable with our findings in a small group of younger patients but our older patients seemed to have developed irreversible retinal changes in most of their retinal arterioles. Our results provide some support for those who advocate early treatment to minimize hypertensive vascular disease. Changes in the diameter of the veins also require explanation. Both normal and hypertensive subjects show considerable venoconstriction during oxygen breathing and in the latter group this sometimes occurred when there had been little change in the diameter of the visible arterioles. The veins in the normal eye became slightly narrower in the upright position and they dilated in the hypertensive subjects when the blood pressure was lowered with hydralazine. As there is little evidence of smooth muscle in the walls of small retinal veins,'3 they would not be expected to show vasomotor responses. Many of the caliber changes can be explained as purely passive. The pressure relations of the thin-walled retinal vein resemble those of the collapsible tubing of the resistor of a Starling heart-lung preparation. At the outflow of the eye there is a zone of rapid change of pressure similar to that in the Starling resistor and sometimes referred to as a "vascular sluice"' or "waterfall."14 If the intraocular tension exceeds the .downstream venous pressure, which it must do under all physiological circumstances, a constriction will tend to form in the veins at the outflow from the eye. The pressure in the retinal veins will then be the intraocular pressure plus a small transmural pressure RAMALHO, DOLLERY 588 Downloaded from http://circ.ahajournals.org/ by guest on June 17, 2017 linearly related to the flow. Changes in venous pressure downstream will not affect either pressure or flow in the eye unless the venous pressure reaches or exceeds the intraocular pressure. Most of the changes in the caliber of the retinal veins can be explained on the basis of retinal blood flow. Thus, the small constriction that occurs on standing in normal subjects may be a reflection of the reduction in cardiac output that normally occurs in this position. Dilatation with hydralazine can be explained by the increase of blood flow which probably takes place with this drug. Constriction with oxygen may result from the reduction of blood flow following arteriolar constriction. The difficulty with this explanation is that it scarcely explains why venoconstriction occurs in response to oxygen in hypertensive patients whose arterioles do not respond. It is still possible that arterioles too small to be measured from color photographs do constrict in these patients but we have no direct evidence of this. Acknowledgment This work was supported by the Medical Research Council. We thank the patients and normal volunteers who consented to take part in this investigation. References 1. GOWERS, W. R.: State of the arteries in Bright's disease. Brit Med J 2: 743, 1876. 2. MOOR, R. F.: Retinitis of arterio-sclerosis, and its relation to renal retinitis and to cerebral vascular disease. Quart J Med 10: 29, 1916. 3. VoLHARD, F., AND FAHR, K. T.: Brightsche Mirenkrankeit: Klinik, Pathologie und AUas. Berlin, Springer-Verlag, 1914, p. 8. 4. KEITH, N. M., WAGENER, H. P., AND BARKER, N. W.: Some different types of essential hypertension: Their course and prognosis. Amer J Med Sci 197: 332, 1939. 5. DOLLERY, C. T., HILL, D. W., AND HODGE, J. V.: Response of normal retinal blood vessels to angiotensin and noradrenaline. J Physiol 165: 500, 1963. 6. CUISICK, P. L., BENSON, D. P., JR., AND BOoTHBY, W. N.: Effect of anoxia and high concentration of oxygen on the retinal vessels. Mayo Clin Proc 15: 500, 1940. 7. SIEKER, H. O., AND HICKAM, J. B.: Normal and impaired retinal vascular reactivity. Circulation 7: 79, 1953. 8. DOLLERY, C. T., HILL, D. W., MAILER, C. M., AND RAMALHO, P. S.: High oxygen pressure and the retinal blood vessels. Lancet 2: 291, 1964. 9. MALMFORS, T.: Adrenergic innervation of the eye as demonstrated by fluorescence microscopy. Acta Physiol Scand 65: 259, 1965. 10. LATIES, A. M.: Central retinal artery innervation: Absence of adrenergic innervation to the intraocular branches. Arch Ophth (Chicago) 77: 405, 1967. 11. EHRINGER, B.: Adrenergic nerves to the eye and related structures in man and in the cynomalgus monkey (Macaca irus). Invest Ophthal 5: 42, 1966. 12. BYROM, F. B.: Vascular crisis in hypertensives. In Antihypertensive Therapy (an International Symposium), edited by F. Gross. Basel, Springer-Verlag, 125, 1966. 13. HAGGAN, M. J., AND FEENEY, L.: Ultrastructure of retinal blood vessels. J Ultrastruct Res 9: 10, 1963. 14. PERMUTT, S., AND RILEY, R. L.: Haemodynamics of collapsible vessels with tone: Vascular waterfall. J Appl Physiol 18: 924, 1963. Circulation, Volume XXXVII, April 1968 Hypertensive Retinopathy: Caliber Changes in Retinal Blood Vessels Following Blood-Pressure Reduction and Inhalation of Oxygen P. S. RAMALHO and C. T. DOLLERY Downloaded from http://circ.ahajournals.org/ by guest on June 17, 2017 Circulation. 1968;37:580-588 doi: 10.1161/01.CIR.37.4.580 Circulation is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Copyright © 1968 American Heart Association, Inc. All rights reserved. Print ISSN: 0009-7322. Online ISSN: 1524-4539 The online version of this article, along with updated information and services, is located on the World Wide Web at: http://circ.ahajournals.org/content/37/4/580 Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in Circulation can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office. Once the online version of the published article for which permission is being requested is located, click Request Permissions in the middle column of the Web page under Services. Further information about this process is available in the Permissions and Rights Question and Answer document. Reprints: Information about reprints can be found online at: http://www.lww.com/reprints Subscriptions: Information about subscribing to Circulation is online at: http://circ.ahajournals.org//subscriptions/