Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
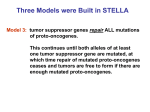
Leukemia (2005) 19, 329–334 & 2005 Nature Publishing Group All rights reserved 0887-6924/05 $30.00 www.nature.com/leu REVIEW CEBPA point mutations in hematological malignancies H Leroy1, C Roumier1, P Huyghe2, V Biggio1, P Fenaux3 and C Preudhomme1 Laboratoire d’Hématologie A, CHRU Lille, U524 INSERM Lille, France; 2Service des Maladies du sang, CHRU Lille, France; and Service d’Hématologie Clinique, Hôpital Avicenne-Paris 13 University, France 1 3 The CCAAT/enhancer-binding protein-alpha (CEBPA) is a transcription factor strongly implicated in myelopoiesis through control of proliferation and differentiation of myeloid progenitors. Recently, several works have reported the presence of CEBPA-acquired mutations in hematological malignancies. In this work, we analyzed characteristics of mutations and their correlation with disease characteristics described in previous studies. In the 1175 patients reported, 146 CEBPA mutations were identified in 96 patients. Mutations were found in the whole gene sequence, but cluster regions were clearly identified. Furthermore, two categories of mutations were reported: out-of-frame ins/del often in the N-terminal region, and in-frame ins/del often in the C-terminal region. CEBPA mutations were reported exclusively in acute myeloid leukemia (AML) (according to WHO classification criteria) and mutated patients preferentially belonged to M1, M2 and M4 FAB subtypes. All but one case belonged to the ‘intermediate’ prognostic subgroup of MRC classification. In the absence of poor prognostic factors, patients with CEBPA mutation had favorable outcome, very similar to that of the t(8;21), inv(16), t(15;17) subgroup. Systematic analysis of CEBPA mutations, in addition to that of alterations in master genes of hematopoiesis, may be useful to assess the prognosis of AML particularly in patients belonging to the ‘intermediate’ prognostic subgroup. Leukemia (2005) 19, 329–334. doi:10.1038/sj.leu.2403614 Published online 13 January 2005 Keywords: CEBPA; mutations; AML; prognosis; transcription factor; CCAAT/enhancer-binding protein Introduction Among the many oncogenes affecting proliferation and cell death, anomalies of the genes implicated in the closely regulated pathways of hematopoietic differentiation are key oncogenic events.1 In acute myeloid leukemia (AML), cell differentiation arrest can occur at different levels by alteration of specific genes like those of the CBF complex.2 The CEBPA gene (located on chromosome 19q13.1 band) belongs to the CCAAT/enhancer-binding protein family, which is involved in the balance between cell proliferation and terminal differentiation. CEBPA gene mRNA can be translated from the first AUG encoding the 42-kDa normal isoform and also from the second AUG (nt 508–510) encoding the 30-kDa normal isoform, which has lost the 119 first AA including the TAD1 functional domain. The functions of CEBPA 30-kDa protein are not well known. Nevertheless, Pabst et al3 demonstrated that this shorter CEBPA protein had lost normal CEBPA functions and had dominant negative effect on 42-kDa Correspondence: Dr C Preudhomme, Laboratoire d’Hématologie A – hôpital Calmette, CHRU, Place de Verdun, 59000 Lille, France; Fax: þ 33 3 20 44 55 10; E-mail: [email protected] Received 19 July 2004; accepted 4 November 2004; Published online 13 January 2005 wild-type (wt) CEBPA. The 42-kDa CEBPA protein has four principal domains: the C-terminal part containing a leucine zipper domain mediating homo- or heterodimerization; the DNA-binding domain (DBD), a basic positively charged domain able to interact with specific DNA sequences; and two regulatory and transactivating domains TAD1 and TAD2 (Figure 1). The 42-kDa normal protein acts as a transcription factor with a crucial role during differentiation of various cell types including hepatocytes, adipocytes, enterocytes, keratinocytes, lung, mammary gland cells and hematopoietic cells. In hematopoiesis, CEBPA plays a pivotal role in early stages of myeloid differentiation and is particularly expressed in myelomonocytic cells.4–8 CEBPA has multiple actions such as downregulation of C-MYC expression allowing differentiation, direct upregulation of the expression of granulocytic lineage-specific genes and synergistic action with other key genes in myeloid development including CBF complex genes and PU.1.5,9–11 In addition to specific DNA binding, CEBPA could act by protein– protein interaction. The principal partners of those interactions are p21, CDK2, CDK4 and E2F. Repression of E2F-dependent transcription genes by CEBPA had previously been shown to be a critical event in suppressing cellular proliferation and inducing granulocytic or adipocyte differentiation. CEBPA also inhibits cell proliferation by activating transcription of p21/WAF1, by stabilizing p21 and inhibiting CDK2 and CDK4.12–14 CEBPA expression begins with the commitment of myeloid lineage precursors and is upregulated during granulocytic differentiation.7 CEBPA-defective mice have no mature granulocytes, whereas cells of the other lineages are not affected.15 In addition, CEBPA expression could block monocytic differentiation.16 The strong implication of CEBPA in granulocytic differentiation points to this gene as a key target in leukemogenesis, as shown now in many studies. Pabst et al3 found that events leading to the loss of CEBPA function observed in AML contribute to leukemogenesis by blocking granulocytic differentiation. Moreover, myeloid blasts observed in those cases were committed myeloid cells generally classified in the M1 or M2 FAB AML subtypes.17 Recently, three mechanisms of CEBPA inactivation have been reported. One is downregulation of CEBPA expression by the AML1-ETO fusion transcript in t(8,21) leukemia cells. In this model, conditional expression of CEBPA in those cells is sufficient to trigger granulocytic differentiation.18 The second mechanism is inhibition of the translation of CEBPA mRNA by interaction with hnRNPE2, induced by BCR-ABL fusion protein.19 This mechanism could contribute to the transition from chronic phase to myeloid blast crisis in CML, by blocking myeloid differentiation. Finally, inactivating CEBPA mutations have been reported in hematological malignancies, especially in AML.3,20–26 In this review, we focused on CEBPA mutations and how, through inactivation of CEBPA mutations in hematological malignancies H Leroy et al 330 120 2nd ATG AA : 99 104 183 189 286 nt : 445 462 697 714 1006 Clustering regions R1 nt 1 445 R2 462 306 317 345 1068 1099 1183 R3 732 855 R4 1059 1062 R5 1137 1152 1196 % 60 50 40 Single alteration 30 20 10 0 R1 R2 R3 R4 R5 R1 R2 R3 R4 R5 % 60 50 Multiple alterations 40 30 20 10 0 Legend: : Transactivating Domain 1 (Poly-Gly) : Transactivating Domain 2 (Poly-Pro) : Out of frame ins / del mutations : In frame ins / del mutations : DNA Binding Domain (DBD) : Other type mutations : Leucine Zipper Domain Figure 1 Schematic representation of CEBPA functional domain; incidence of the different types of mutation and localization of mutation hot spot regions. transcriptional properties of the CEBPA protein, they could lead to leukemogenesis. Correlation of CEBPA mutations with hematological parameters and prognosis CEBPA mutations and morphological classification Overview of CEBPA gene mutations reported In the last 3 years, 1175 patients were screened for CEBPA mutations in seven studies.3,21–25,27.Those patients included 962 AML (Table 1), 156 myelodysplastic syndromes, 23 acute lymphoblastic leukemia and 34 non-Hodgkin’s lymphoma. Among those 1175 patients, 96 (8.2%) had CEBPA mutations including nine with silent mutations and 87 with acquired nonsilent mutations (described in online additional data, supplementary data). CEBPA mutations were only observed in myeloid malignancies. Leukemia All but two of the 87 reported patients with CEBPA mutation had AML, including 30 M1 AML, 35 M2 AML, 14 M4 AML, three M5 AML, two unclassified AML and one therapy-related AML (incidence in AML: 85 on 962 patients (8.8 %) ; see Table 1). The two remaining patients had RAEB-t (a disorder now included in AML in the new WHO classification of myeloid disorders). FAB classification of AML and MDS was available in 712 patients studied for CEBPA mutations. Incidences of mutations were 14.5 % of M1, 6.4% of M2, 4% of M4, 2% of M5, one of CEBPA mutations in hematological malignancies H Leroy et al 331 the seven therapy-related AML and one of the 12 RAEB-t. No mutations were found in M0, M3, M6 and M7-AML. In these four studies, the complete remission rate was not significantly different in patients with or without CEBPA mutations, but all studies except that of Snaddon et al21 showed better relapse-free survival (RFS) or overall survival (OS) in mutated cases. Discrepancies between Snaddon et al21 and other studies could have been due to some characteristics of their mutated cases, including higher peripheral blood blast count (median of 93 109/l vs o24 109/l in the mutated cases of other studies), the localization of mutations (five of eight mutated patients had a single alteration of the C-terminal part of CEBPA protein vs zero of 27 in the other studies), and, although this is more speculative, the fact that five of their eight mutated patients received standard dose AraC instead of highdose AraC in the other studies. An analysis of cooperating mutations, made in two studies, showed no difference in the incidence of FLT3 and MLL alterations in CEBPA-mutated and -nonmutated patients.24,27 However, in patients with CEBPA mutation, Preudhomme et al,24 showed that the presence of FLT3 internal tandem duplication (FLT3-ITD) had a negative prognostic influence, whereas, in the study of Fröhling et al,27 the presence of FLT3ITD or FLT3 mutations had no prognostic impact. Nevertheless, in the two studies, the size of the population studied was too small for definite conclusions (15 patients in Preudhomme et al, study24 and 36 patients in Fröhling et al, study27). Cytogenetic findings Cytogenetic data was available in 83 of the 87 mutated patients (see online additional data). Only one had a complex karyotype with more than three abnormalities; 58 cases (70%) had a normal karyotype and eight (10%) had only one abnormality. In the remaining 15 mutated cases, the karyotype was classified in the ‘intermediate’ prognostic subgroup without further details; no structural or numerical alteration of chromosome 19 and no ‘favorable’ karyotype (t(8;21), inv(16), t(16;16), t(15;17)) was reported in those patients. Therefore, all except one of the mutated cases belonged to the ‘intermediate’ subgroup of the MRC classification.28 This may suggest that CEBPA loss of function induced by balanced translocations and CEBPA loss of function by point mutation are mutually exclusive. Other clinical and biological correlations (Table 2) When they were studied, no correlation was observed between CEBPA mutations and age, sex, WBC count and bone marrow blast percentage. Prognostic value of CEBPA mutations CEBPA mutation profile in mutated cases (Table 3) Four studies have evaluated the prognostic impact of CEBPA mutations in 71 mutated patients, by comparison to 670 patients without CEBPA mutation.21,22,24,27 A total of 45 patients had a single CEBPA alteration, whereas 42 cases had multiple alterations resulting from biallelic mutations or from several mutations on the same allele. There was no Table 1 Prevalence of nonsilent CEBPA mutations in acute myeloid leukemia (AML) Study No of patients studied 1 236 M0 AML M1 AML M2 AML M3 AML M4 AML M5 AML M6 AML M7 AML Sec, AML Uncl, AML Incidence of mutations 2 78 FAB subtypes not available 36/236 6/78 3 137 4 99 5 135 6 277 Cumulative incidence (%) 0/1 2/8 5/62 0/22 0/32 0/5 NC NC 1/7 NC 8/137 NC 6/56 2/43 NC NC NC NC NC NC NC 8/99 0/1 8/33 2/34 NC 3/19 2/32 0/5 0/4 NC 0/7 15/135 0/10 7/62 4/64 0/22 1/50 0/61 0/3 NC NC 0/5 12/277 0 14.5 6.4 0 4 2 0 0 14.3 0 8.8 (85/962) Sec. AML ¼ secondary AML; Uncl. AML ¼ unclassified AML; NC ¼ no case. Study 1 ¼ Fröhling et al; Study 2 ¼ Gombart et al; Study 3 ¼ Pabst et al; Study 4 ¼ Snaddon et al; Study 5 ¼ Preudhomme et al; Study 6 ¼ Khosrovani et al. Table 2 Clinical and biological characteristics of AML patients with and without CEBPA mutation (median values) WT Fröhling et al Preudhomme et al Snaddon et al Khosrovani et al 47 45 46.5 NA Age Mutated 47 45 55.5 44 % Female WT Mutated WBC (giga/l) WT Mutated 55 49 36 NA 19.9 13 NA NA 50 33 62 33 28.9 20 NA 34.5 PB blasts WT Mutated 40% NA 9.2 G/l NA 62% NA 9.2 G/l NA BM blasts (%) WT Mutated Platelets (giga/l) WT Mutated 80 NA 75 NA 93 NA NA NA 80 NA 80 64.5 45 NA NA 41 WT ¼wild-type; WBC ¼ white blood count; PB ¼ peripherical blood; Na ¼ not available. Leukemia CEBPA mutations in hematological malignancies H Leroy et al 332 significant difference in location and type of mutations between patients with single or multiple alterations (Figure 1). multiple mutations, patients had preferentially M1-AML (45%), whereas, in case of single mutation, patients had preferentially M2-AML (44%) (Table 3). Characteristics of CEBPA mutations Pathogenetic role of CEBPA mutations Until now, 146 CEBPA mutations have been described in 96 patients,3,21–25,27 including nine isolated silent mutations without transcriptional effect in nine patients and 137 nonsilent CEBPA mutations in 87 patients (five missense mutations, 54 inframe ins/del mutations, 78 nonsense mutations including five STOP codon point mutations and 73 out-of-frame ins/del mutations inducing a STOP codon downstream). Reported mutations were nonrandomly distributed all over the CEBPA gene sequence and occurred in five regions of the protein (regions R1 to R5) (Figure 1): R1 corresponding to the AA before the Poly-Gly domain, R2 between the Poly-Pro and the Poly-Gly domain, R3 corresponding to the N-terminal part of the DBD and the region just before the DBD domain, R4 corresponding to the C-terminal part of the DBD and to the N-terminal part of the b-Zip domain (fork region), R5 corresponding to the C-terminal part of the B-zip domain. R1 and R4 were the two main cluster regions as 76% of the 137 nonsilent mutations belonged to these regions. Moreover, the distribution of the type of mutations between these two regions was heterogeneous. Nearly all out-of-frame ins/del nonsense mutations occurred in R1 region, whereas most 54 inframe ins/del mutations occurred in R4 region. Functional study of the mutated protein showed important loss of transactivation properties of CEBPA in almost all cases of mutation25 Interestingly, among the 78 nonsense mutations, 65 occurred at the 50 of the second ATG codon of CEBPA (R1 region) leading to increased translation of the alternative 30-kDa form of the protein. As demonstrated by Pabst et al, this shorter protein has a dominant negative effect on 42-kDa wt CEBPA. Conversely, none of the 54 in-frame ins/del mutations lead to increased synthesis of the dominant negative 30-kDa isoform. A minor cluster region (R2 region) has been reported by Fröhling et al,27 who found 14 recurring mutations in the TAD2 domain. Those alterations were 6 bp duplications or 3 bp deletions inducing the addition of H-P AA in a motif of three H-P repeats, or deletion of one P in a motif of seven P repeats. Of the nine cases with TAD2 mutation, seven had no 30-kDa dominant negative form. The significance of such recurrent alterations (ie repeats of GCC nucleotide triplets) remains to be understood. Overall, in 55 of the 87 mutated cases, mutations lead to the synthesis of the dominant negative 30-kDa form, which inhibits CEBPA normal function. No significant correlation between localization, number of mutations and FAB subtypes could be established (Figure 1). Of note, however, is the fact thatin case of Table 3 Expression of 30-kDa dominant negative isoform according to FAB subtype and number of CEBPA mutations Single alteration 30-kDa isoform Leukemia M1 AML M2 AML M3 AML Other 5 11 8 2 (45%) (55%) (89%) (40%) Total 26 (75%) 30-kDa isoform+ 6 9 1 3 (55%) (45%) (11%) (60%) 19 (25%) Multiple alteration 30-kDa isoform 30-kDa isoform+ 5 2 1 1 14 13 4 2 (26%) (13%) (20%) (33%) 9 (21%) (74%) (87%) (80%) (66%) 33 (%) How CEBPA mutations can contribute to leukemogenesis in AML and to prognosis remains uncertain. It has been shown that CEBPA mutations induced modifications in the gene expression profile obtained from blast cells, and that, if AML patients were classified according to the gene expression profile, CEBPA mutated patients segregated in two homogeneous clusters.29 A review of the currently published CEBPA mutations suggests two main types of mutated cases. The first group contains patients with at least one mutation in R1 or R2 clustering regions leading to increased translation of the 30-kDa isoform from the second AUG downstream of the mutation, inducing the indirect loss of CEBPA main function in a dominant negative manner. The other group contains patients where CEBPA gene mutations result in loss of the main transregulatory function of CEBPA, mainly due to multiple alterations of the gene; absence of wt CEBPA protein in blast cells could explain the differentiation arrest of these cells. How can mutations contributing to the loss of function of a master gene in early myeloid differentiation result in a myeloid type of leukemia? It has previously been reported that biallelic mutations of another early myeloid differentiation gene (AML1/ RUNX1) could induce M0 AML subtype.2 Furthermore, mice models of CML blast crisis with CEBPA knockout result in immature erythroid leukemia30,31 and expression of a dominant negative 30-kDa CEBPA protein inhibits differentiation of myeloid and erythroid progenitors.32 On the other hand, all CEBPAmutated patients reviewed in this work had M1, M2, M4 or M5 AML subtypes, clearly showing persistence of myeloid differentiation in blast cells. However, in mutated cases with multiple alterations of CEBPA, preventing expression of wt protein, or in single alterations with expression of p30 dominant negative form, the persistence of CEBPA residual cellular functions has been demonstrated.31,33,34 Therefore, those cases are not identical to KO models since the loss of transactivating properties is dependent of on cis-regulating elements of the CEBPA target genes. Moreover, other members of the CEBPA family, including CEBPB and CEBPE, could partially prevent the effects of the loss of function of mutated CEBPA and allow incomplete myeloid differentiation resulting in M1, M2, M4 and M5 blasts. Pabst et al18 demonstrated that, when CEBPA nonsense mutations occurred before the second AUG, the 30-kDa CEBPA isoform was increased by 4.2–8.6-fold compared with unmutated cases. This shorter form of CEBPA lacks antiproliferative activity35 and most of the transactivation properties of the normal protein,36,37 and acts dominantly on wt CEBPA by inhibiting DNA binding of CEBPA on targeted genes.3 Indeed, in the presence of equal amounts of 42-kDa and 30-kDa in vitro, the 30-kDa isoform totally abolished transactivation of a plasmid reporter by the full-length CEBPA protein.18 The 30-kDa protein binds DNA with only 14% affinity compared with the full-length protein and can inhibit DNA binding of wt CEBPA.3 However, the 30-kDa isoform does not inhibit 42-kDa normal function on each CEBPA-transregulated genes. For example, MPO gene expression is not abrogated by the 30-kDa form.31,34 The predominance of M1 and M2 FAB subtypes in CEBPA-mutated AML, with partial myeloid differentiation block in blast cells, is compatible with this effect and the higher incidence of CEBPA mutations in M1, M2 and M4 FAB subtypes supports a critical role of CEBPA gene function in CEBPA mutations in hematological malignancies H Leroy et al 333 the intermediate stages of granulocytic differentiation. One may hypothesize that events inducing loss of CEBPA gene function in transformed myeloid precursor cells could lead to M1, M2 or M4 FAB AML. In mutated cases where no 30-kDa is synthetized, other mechanisms are required to explain the contribution of CEBPA mutations to leukemogenesis. Since as few as three-fold increases in CEBPA 42-kDa protein are sufficient to induce differentiation of myeloid cell lines,8 it is possible that only moderate decreases of CEBPA protein in vivo are sufficient to explain the differentiation block in those AML. This could be achieved by haploinsufficiency resulting from single C-terminal mutations. It has been shown that patients with CEBPA mutations had similar prognosis as patients belonging to the ‘favorable’ group according to MRC classification (including t(8;21), inv(16) and t(15;17) AML). It is difficult to speculate on the reasons of this favorable prognosis of AML with CEBPA mutations. However, there are some similarities between the cellular effects of the chimeric oncoproteins observed in AML with ‘favorable’ karyotype and the cellular effects of CEBPA mutations found in AML with normal karyotype (belonging to the ‘intermediate’ karyotype subgroup of MRC classification). In both situations, CEBPA function is repressed. Indeed, chimeric proteins induce the disruption of CEBPA normal functions: in t(8;21), AML1-ETO is able to suppress CEBPA protein expression by decreasing the level of CEBPA mRNA18,38; in inv(16), CBFb-MYH11 is also able to disturb CEBPA functions38 and in t(15;17), Truong et al,39 showed that PML-RARa blocked CEBPA activity. Those similarities could contribute to explain why AML with CEBPA mutations have favorable prognosis in AML. This favorable prognostic value and the predominance of CEBPA mutations in M1, M2 and M4 AML justifies, in our opinion, systematic screening for CEBPA mutations in those AML groups, especially in patients belonging to the intermediate prognosis cytogenetic group. Analysis of the currently reported CEBPA mutations has shown a nonrandom distribution of mutations in the coding sequence of the gene, with two principal mutation cluster regions (R1 and R4). Mutation types are not equally distributed between the two regions as more than 87% of in-frame ins/del mutations occurred in the R4 region (if we exclude the TAD2 inframe ins/del) and nonsense out-of-frame mutation localized in the R1 region in 82% of the cases. As the size of ins/del mutations is shorter in out-of-frame ins/del mutations, the best screening methods may differ for each region: gene scan method after amplification may be preferable for the C-terminal region (R3 and R4 regions) and direct sequencing for the N-terminal region (genomic sequence coding for AA 1–200, including R1 and R2 region). By these methods, 92% of the 137 CEBPA mutations and 100% of the mutations inducing the synthesis of dominant negative 30-kDa isoform would have been identified. Systematic screening of CEBPA mutations in association with the search of other alterations in master genes implicated in leukemogenesis such as FLT3, MLL or RAS should probably be performed systematically in AML, particularly in patients belonging to the ‘intermediate’ prognostic group, to determine more precisely the impact of the association between genetic events on overall survival and therapeutic response in large cohorts of patients. Acknowledgements This work was supported by the ‘Fondation de France’ and by the ‘Ligue contre le cancer, Comité Nord’. We thank Dan Tenen for critical reading of this manuscript. Supplementary Information Supplementary Information accompanies the paper on the Leukemia website (http://www.nature.com/leu). References 1 Tenen DG. Disruption of differentiation in human cancer: AML shows the way. Nat Rev Cancer 2003; 3: 89–101. 2 Roumier C, Fenaux P, Lafage M, Imbert M, Eclache V, Preudhomme C. New mechanisms of AML1 gene alteration in hematological malignancies. Leukemia 2003; 17: 9–16. 3 Pabst T, Mueller BU, Zhang P, Radomska HS, Narravula S, Schnittger S et al. Dominant-negative mutations of CEBPA, encoding CCAAT/enhancer binding protein-alpha (C/EBPalpha), in acute myeloid leukemia. Nat Genet 2001; 27: 263–270. 4 Tenen DG, Hromas R, Licht JD, Zhang DE. Transcription factors, normal myeloid development, and leukemia. Blood 1997; 90: 489–519. 5 Reddy VA, Iwama A, Iotzova G, Schulz M, Elsasser A, Vangala RK et al. Granulocyte inducer C/EBPalpha inactivates the myeloid master regulator PU.1: possible role in lineage commitment decisions. Blood 2002; 100: 483–490. 6 Zhang P, Nelson E, Radomska HS, Iwasaki-Arai J, Akashi K, Friedman AD et al Induction of granulocytic differentiation by 2 pathways. Blood 2002; 99: 4406–4412. 7 Keeshan K, Santilli G, Corradini F, Perrotti D, Calabretta B. Transcription activation function of C/EBPalpha is required for induction of granulocytic differentiation. Blood 2003; 102: 1267–1275. 8 Radomska HS, Huettner CS, Zhang P, Cheng T, Scadden DT, Tenen DG. CCAAT/enhancer binding protein alpha is a regulatory switch sufficient for induction of granulocytic development from bipotential myeloid progenitors. Mol Cell Biol 1998; 18: 4301–4314. 9 Johansen LM, Iwama A, Lodie TA, Sasaki K, Felsher DW, Golub TR et al. c-Myc is a critical target for c/EBPalpha in granulopoiesis. Mol Cell Biol 2001; 21: 3789–3806. 10 Smith LT, Hohaus S, Gonzalez DA, Dziennis SE, Tenen DG. PU.1 (Spi-1) and C/EBP alpha regulate the granulocyte colony-stimulating factor receptor promoter in myeloid cells. Blood 1996; 88: 1234–1247. 11 Klempt M, Melkonyan H, Hofmann HA, Eue I, Sorg C. The transcription factors c-myb and C/EBP alpha regulate the monocytic/myeloic gene MRP14. Immunobiology 1998; 199: 148–151. 12 D’Alo F, Johansen LM, Nelson EA, Radomska HS, Evans EK, Zhang P et al. The amino terminal and E2F interaction domains are critical for C/EBP alpha-mediated induction of granulopoietic development of hematopoietic cells. Blood 2003; 102: 3163– 3171. 13 Wang QF, Cleaves R, Kummalue T, Nerlov C, Friedman AD. Cell cycle inhibition mediated by the outer surface of the C/EBPalpha basic region is required but not sufficient for granulopoiesis. Oncogene 2003; 22: 2548–2557. 14 Timchenko NA, Wilde M, Nakanishi M, Smith JR, Darlington GJ. CCAAT/enhancer-binding protein alpha (C/EBP alpha) inhibits cell proliferation through the p21 (WAF-1/CIP-1/SDI-1) protein. Genes Dev 1996; 10: 804–815. 15 Zhang DE, Zhang P, Wang ND, Hetherington CJ, Darlington GJ, Tenen DG. Absence of granulocyte colony-stimulating factor signaling and neutrophil development in CCAAT enhancer binding protein alpha-deficient mice. Proc Natl Acad Sci USA 1997; 94: 569–574. 16 Friedman AD. Transcriptional regulation of granulocyte and monocyte development. Oncogene 2002; 21: 3377–3390. 17 Bennett JM, Catovsky D, Daniel MT, Flandrin G, Galton DA, Gralnick HR et al. Proposals for the classification of the acute leukaemias. French–American–British (FAB) co-operative group. Br J Haematol 1976; 33: 451–458. 18 Pabst T, Mueller BU, Harakawa N, Schoch C, Haferlach T, Behre G et al. AML1-ETO downregulates the granulocytic differentiation factor C/EBPalpha in t(8;21) myeloid leukemia. Nat Med 2001; 7: 444–451. Leukemia CEBPA mutations in hematological malignancies H Leroy et al 334 19 Perrotti D, Cesi V, Trotta R, Guerzoni C, Santilli G, Campbell K et al. BCR-ABL suppresses C/EBPalpha expression through inhibitory action of hnRNP E2. Nat Genet 2002; 30: 48–58. 20 Nerlov C. C/EBPalpha mutations in acute myeloid leukaemias. Nat Rev Cancer 2004; 4: 394–400. 21 Snaddon J, Smith ML, Neat M, Cambal-Parrales M, Dixon-McIver A, Arch R et al. Mutations of CEBPA in acute myeloid leukemia FAB types M1 and M2. Genes Chromosomes Cancer 2003; 37: 72–78. 22 van Waalwijk van Doorn-Khosrovani SB, Erpelinck C, Meijer J, van Oosterhoud S, van Putten WL, Valk PJ et al. Biallelic mutations in the CEBPA gene and low CEBPA expression levels as prognostic markers in intermediate-risk AML. Hematol J 2003; 4: 31–40. 23 Kaeferstein A, Krug U, Tiesmeier J, Aivado M, Faulhaber M, Stadler M et al. The emergence of a C/EBPalpha mutation in the clonal evolution of MDS towards secondary AML. Leukemia 2003; 17: 343–349. 24 Preudhomme C, Sagot C, Boissel N, Cayuela JM, Tigaud I, de Botton S, et al., ALFA Group. Favorable prognostic significance of CEBPA mutations in patients with de novo acute myeloid leukemia: a study from the Acute Leukemia French Association (ALFA). Blood 2002; 100: 2717–2723. 25 Gombart AF, Hofmann WK, Kawano S, Takeuchi S, Krug U, Kwok SH et al. Mutations in the gene encoding the transcription factor CCAAT/enhancer binding protein alpha in myelodysplastic syndromes and acute myeloid leukemias. Blood 2002; 99: 1332–1340. 26 Chim CS, Wong AS, Kwong YL. Infrequent hypermethylation of CEBPA promotor in acute myeloid leukaemia. Br J Haematol 2002; 119: 988–990. 27 Fröhling S, Schlenk RF, Stolze I, Bihlmayr J, Benner A, Kreitmeier S et al. Mutations in younger adults with acute myeloid leukemia and normal cytogenetics: prognostic relevance and analysis of cooperating mutations. J Clin Oncol 2004; 22: 624–633. 28 Grimwade D, Walker H, Oliver F, Wheatley K, Harrison C, Harrison G et al. The importance of diagnostic cytogenetics on outcome in AML: analysis of 1612 patients entered into the MRC AML 10 trial. The Medical Research Council Adult and Children’s Leukaemia Working Parties. Blood 1998; 92: 2322–2333. 29 Valk PJ, Verhaak RG, Beijen MA, Erpelinck CA, Barjesteh van Waalwijk van Doorn-Khosrovani S, Boer JM et al. Prognostically Leukemia 30 31 32 33 34 35 36 37 38 39 useful gene-expression profiles in acute myeloid leukemia. N Engl J Med 2004; 350: 1617–1628. Iwama A, Osawa M, Hirasawa R, Uchiyama N, Kaneko S, Onodera M et al. Reciprocal roles for CCAAT/enhancer binding protein (C/EBP) and PU.1 transcription factors in Langerhans cell commitment. J Exp Med 2002; 195: 547–558. Wang QF, Friedman AD. CCAAT/enhancer-binding proteins are required for granulopoiesis independent of their induction of the granulocyte colony-stimulating factor receptor. Blood 2002; 99: 2776–2785. Schwieger M, Lohler J, Fischer M, Herwig U, Tenen DG, Stocking C. A dominant-negative mutant of C/EBPalpha, associated with acute myeloid leukemias, inhibits differentiation of myeloid and erythroid progenitors of man but not mouse. Blood 2004; 103: 2744–2752. Cleaves R, Wang QF, Friedman AD. C/EBPalphap30, a myeloid leukemia oncoprotein, limits G-CSF receptor expression but not terminal granulopoiesis via site-selective inhibition of C/EBP DNA binding. Oncogene 2004; 23: 716–725. Friedman AD, Keefer JR, Kummalue T, Liu H, Wang QF, Cleaves R. Regulation of granulocyte and monocyte differentiation by CCAAT/enhancer binding protein alpha. Blood Cells Mol Dis 2003; 31: 338–341. Lin FT, MacDougald OA, Diehl AM, Lane MD. A 30-kDa alternative translation product of the CCAAT/enhancer binding protein alpha message: transcriptional activator lacking antimitotic activity. Proc Natl Acad Sci USA 1993; 90: 9606–9610. Calkhoven CF, Bouwman PR, Snippe L, Ab G. Translation start site multiplicity of the CCAAT/enhancer binding protein alpha mRNA is dictated by a small 50 open reading frame. Nucleic Acids Res 1994; 22: 5540–5547. Ossipow V, Descombes P, Schibler U. CCAAT/enhancer-binding protein mRNA is translated into multiple proteins with different transcription activation potentials. Proc Natl Acad Sci USA 1993; 90: 8219–8223. Cilloni D, Carturan S, Gottardi E, Messa F, Messa E, Fava M et al. Down-modulation of the C/EBPalpha transcription factor in core binding factor acute myeloid leukemias. Blood 2003; 102: 2705–2706. Truong BT, Lee YJ, Lodie TA, Park DJ, Perrotti D, Watanabe N et al. CCAAT/enhancer binding proteins repress the leukemic phenotype of acute myeloid leukemia. Blood 2003; 101: 1141–1148.