Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
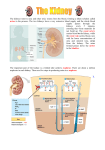
UNIT 8 NOTES THE URINARY SYSTEM Excretion: § The removal of nitrogen-containing waste products of metabolism and any excess substances due to cell metabolism ú E.g. Urea Parts of the Urinary System: 1. Kidney: • Main excretory organ • Help maintain homeostasis through regulation of H2O and ions • Blood enters the kidney via the renal artery, is cleaned, and leaves the kidney in the renal vein 2. Ureter: • Transports urine from kidney to bladder • Conveys urine by peristalsis 3. Urinary Bladder: • stores the urine • Expandable • When full, the sphincter muscles control the release of urine from the bladder 4. Urethra: • when the sphincter relaxes, the urethra carries the urine outside the body. Kidney Function: The kidneys perform a number of homeostatic functions, as they are the chief regulators of our internal environment: 1. Regulates blood volume and osmotic balance by excreting or conserving water as the situation demands. 2. Regulates the ion concentration between the ECF & the blood by controlling the excretion of inorganic salts (especially Na+, but also K+, Cl-, H+, Ca2+, HCO3-). 3. Regulates Blood pH by excreting excess acids or base a) If blood is acidic, H+ is excreted and HCO3- is reabsorbed b) If blood is basic, H+ is not excreted and HCO3- is not reabsorbed 4. Excretes toxic metabolic by-products such as urea, ammonia, uric acid, and creatinine (a product of muscle activity). Nephron: • The functional unit of the kidney is the NEPHRON, which consists of a renal tubule and its associated blood vessels. • Each kidney contains approximately 1 million nephrons Nephron Structure: 1. Bowman’s Capsule: this cup shaped receptacle is the blind end of the renal tubule, which receives filtrate from the blood. It encloses a ball of capillaries called the glomerulus. 2. The proximal convoluted tubule (PCT): most of the important things (nutrients, water, salt…) are reabsorbed from the PCT. 3. The ascending and descending loop of Henle: a lot of salt and water are reabsorbed from Loop of Henle. Dips into renal medulla 4. The distal convoluted tubule (DCT): the blood dumps things (excretion) into the DCT so it can be removed in the urine. 5. The collecting duct: collects filtrate from many tubules and pass the urine into the renal pelvis. Water and urea are also reabsorbed here. Nephron Capillaries: • Each nephron has its own blood supply which is supplied by the renal artery (high O2, glucose, AA, wastes) 1. Afferent Arteriole: o this arteriole enters the bowman’s capsule from the renal artery 2. Glomerulus: o the capillaries of the glomerulus are porous and very twisted up. o They sit within the Bowman’s capsule 3. Efferent Arteriole: • this arteriole leaves the bowman’s capsule. The blood is very hypertonic as most of the plasma has left the blood. The blood carries RBC, WBC, platelets and blood proteins 4. Peritubular Capillaries: • these are the capillaries that surround the Proximal and Distal convoluted tubules µBlood then travels to the renal venule → renal vein → vena cava • High in CO2, glucose, AA • Low in wastes & O2 URINE FORMATION Urine gets rid of wastes (NH3, urea, uric acid, creatinine) and other substances (vitamins, penicillin, histamines) found in excess in the blood Overall process: =blood is filtered using pressure – good and bad stuff enters nephron as filtrate =good stuff is reabsorbed from filtrate to blood =extra stuff and wastes – “fine tuning” occurs to make urine STEPS OF URINE FORMATION: 1. PRESSURE/GLOMERULAR FILTRATION = movement from blood to nephron Pressure Filtration: the high BP forces H2O and solutes through pores of glomerulus into Bowman’s capsule. • holes in glomerulus are small, so they are permeable to H2O and small solutes, but not to the large blood cells or blood proteins. • The filtrate is a mixture of salts, nutrients (glucose & aa), water and other small molecules. • At this point, blood plasma is isotonic (equal) to filtrate 2. SELECTIVE/ TUBULAR REABSORPTION = movement from nephron to blood (peritubular capillary network – PCN) - Occurs mainly in the proximal convoluted tubule o lots of protein carriers and mitochondria for active transport – microvilli for ↑ surface area for absorption – Therefore needs ATP!!! - : important molecules (nutrients ie sugar, salts & H2O) are returned to the blood WHAT IS REABSORBED? : 70% of H2O, and 75% of salts, glucose, amino acids, & other nutrients move back into the blood. • Na+ ions are actively transported into ECF and Cl- ions follow passively; water follows by osmosis. • glucose, aa’s, and other nutrients are actively transported into the blood Therefore, lots of ATP required!! 3. Tubular/Water Reabsorption: H2O reabsorption occurs mainly at the loop of Henle & in the collecting duct. The nephron pumps out salt & urea in these areas to make the blood and medulla extremely hyperosmotic. Water then moves back in to the blood by osmosis The DESCENDING LOOP OF HENLE: • continues the reabsorption of water as the filtrate moves from the cortex and down into the concentrated medulla. • permeable to water, but not very permeable to salt. Lots of WATER moves into the HYPERTONIC blood (created at the ascending loop) by osmosis as it follows the salt. As a result of this great loss of water, the filtrate becomes more and more concentrated The ASCENDING LOOP OF HENLE: • NOT PERMEABLE to water, but salt can move. • NaCl passively and actively moves out of the tubule and into the blood in the renal medulla This creates a very HYPERTONIC solution in the blood.. As the filtrate moves towards the DCT, most of the salt has left and the filtrate becomes more and more dilute. The COLLECTING DUCT: • H2O is also reabsorbed here. • permeable to water and urea. As the duct moves down into the VERY HYPERTONIC medulla, the filtrate loses more and more H2O by osmosis. This loss of H2O concentrates the urea in the filtrate, and because there is so much UREA in the collecting duct, some of it diffuses down its concentration gradient and back into the blood and medulla. 4. TUBULAR SECRETION = movement from blood to nephron • Occurs in distal convoluted tubule by active transport from the blood to tubular fluid • if the blood still needs to rid itself of other ions and waste products (hydrogen ions, ammonia, potassium ions), it will secrete them into the Distal Convoluted Tubule (DCT). • This is a very selective process that involves both active and passive transport. Lots of mitochondria in the DCT too! Urine = filtered substances + those substances not reabsorbed+ secreted substances REGULATION OF URINE FORMATION If you are dehydrated, the kidneys reabsorb the majority of water from the filtrate which causes urine to be dark yellow. ANTIDIURETIC HORMONE (ADH) • released in response to low [water] in the blood (eg dehydration) • controls water reabsorption with a negative feedback cycle. • hypothalamus makes ADH- stored & released from posterior pituitary gland • If a person does not drink much water in a given day, posterior pituitary releases ADH, causing more water to be reabsorbed and less urine to form. -Alcohol can disturb water balance by inhibiting the release of ADH - causes excessive loss of water in the urine (dehydration) - Leads to symptoms of a hangover.