Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
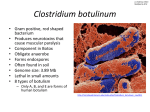
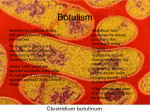
AANEM Case Report # 16 Botulism Ricardo A. Maselli, MD Nandini Bakshi, MD American Association of Neuromuscular & Electrodiagnostic Medicine AAEM CASE REPORT 16 ABSTRACT: Early diagnosis of botulism is essential for effective treatment. Electrophysiologic testing can be of major help to establish a prompt diagnosis, but the classic electrodiagnostic features of botulism are often elusive. Decrement or increment of compound muscle action potential (CMAP) amplitudes to slow or fast rates of nerve stimulation are often unimpressive or totally absent. Reduction of CMAP amplitudes, denervation activity, or myopathic-like motor unit potentials in affected muscles are found more frequently but they are less specific. In general, the electrophysiologic findings taken together suggest involvement of the motor nerve terminal, which should raise the possibility of botulism. The case reported here illustrates a common clinical presentation of botulism. This study emphasizes realistic expectations of the electrodiagnostic testing, the differential diagnosis, and the potential pitfalls often encountered in the interpretation of the electrophysiologic data. © 2000 American Association of Electrodiagnostic Medicine. Muscle Nerve 23: 1137–1144, 2000 BOTULISM RICARDO A. MASELLI, MD, and NANDINI BAKSHI, MD Department of Neurology, University of California Davis, 1515 Newton Court, Room 502, Davis, California 95616-4859, USA Although there are a number of forms of botulism, the food-borne, wound, and infant types of botulism are the most clinically relevant. This form of the disease results from the ingestion of food contaminated with spores and organisms that have been maintained in anaerobic conditions, resulting in germination and toxin production. Botulinum neurotoxins are resistant to the proteolytic activity of stomach fluids because they are associated with accessory proteins that protect them from proteolysis.38,39 In the alkaline environment of the intestine, the toxins are dissociated from these accessory proteins, absorbed, and transported via the circulation to the nerve terminals of skeletal muscles and the peripheral autonomic system. More than 12,000 cases of food-borne botulism have been recorded worldwide since 1951 with Food-Borne Botulism. Abbreviations: AChR, acetylcholine receptor; APB, abductor pollicis brevis; AQM, acute quadriplegic myopathy; CK, creatine kinase; CMAP, compound muscle action potential; EMG, electromyography; EPP, endplate potential; FCR, flexor carpi radialis; GBS, Guillain–Barré syndrome; LES, Lambert–Eaton syndrome; MEPP, miniature endplate potential; MCD, mean consecutive difference; MFS, Miller-Fisher Syndrome; MG, myathenia gravis; MUP, motor unit potential; NCV, nerve conduction velocities; NMJ, neuromuscular junction; SNAP, sensory nerve action potential; SSFEMG, stimulated single-fiber electromyography Key words: botulism, neuromuscular transmission, presynaptic, repetitive nerve stimulation, nerve terminal Correspondence to: American Association of Electrodiagnostic Medicine, 421 First Avenue SW, Suite 300 East, Rochester, MN 55902; e-mail: [email protected] © 2000 American Association of Electrodiagnostic Medicine. Published by John Wiley & Sons, Inc. AAEM Case Report #16: Botulism a case/fatality rate of 20%.17 About 34% of cases are caused by type A, 52% type B, and 12% type E.18 Wound Botulism. This form of the disease results from the contamination of wounds with bacteria and bacterial spores that proliferate and produce the toxin locally.9 The toxin is in turn transported to peripheral synapses via the circulation. Only types A and B have been encountered so far in wound botulism. Most cases have been reported in the United States, with an overwhelming majority in the state of California.42 Lately, most cases of wound botulism have been reported in drug addicts in association with subcutaneous tissue injection or “popping.”10 The infant variant of the disease was first diagnosed in 1976 and is currently the most common form of botulism in the United States.1,11,31,34 This form results from the ingestion of viable spores that germinate and colonize the intestinal tract. The neurotoxin produced in the intestine is transported via the circulation to peripheral nerve terminals.26 Approximately half of the cases reported in the United States have been identified in the state of California.17 Infant Botulism. At the nerve terminals, the toxin binds via the carboxyterminal of the heavy chain to an as yet unidentified receptor and is internalized through a receptor-mediated endocytosis. Once inside the nerve terminal, the light chain cleaves one Pathogenesis. MUSCLE & NERVE July 2000 1137 or two of the three key proteins involved in the process of neurotransmitter release. These proteins are: VAMP or synaptobrevin of the synaptic vesicle membrane and SNAP-25 and syntaxin of the presynaptic membrane.32 Botulinal toxins A and E hydrolyze SNAP-25, whereas B, D, F, and G cleave VAMP. Botulinal toxin C cleaves both SNAP-25 and syntaxin2,26 (Fig. 1). This cleavage of synaptic proteins disrupts the fusion but not the docking of synaptic vesicles to the presynaptic membrane. Neuromuscular transmission fails as a result of reduction of synaptic vesicle release and decrease of the endplate potential (EPP) quantal content.29 CASE REPORT History. A 44-year–old man with a long-standing history of intravenous drug use and “skin popping” experienced rapidly progressing blurred vision, diplopia, dysphagia, and dysarthria. Two weeks prior to the onset of these symptoms the patient developed an abscess in his right arm at the site of previous “popping.” This required antibiotic treatment with cephalexin (Keflex) and ciprofloxacin. The patient was initially admitted to a small community hospital where he developed respiratory failure and required mechanical ventilation. He was subsequently transferred to a university hospital. On admission, 5 days after the onset of symptoms, the patient was on ventilatory support and fully alert. He communicated by squeezing the Examination. FIGURE 1. Targets of Clostridia neurotoxins in the fusion protein complex. Schematic representation of some of the protein interactions involved in vesicle fusion and the sites of neurotoxin action. Botulinum toxins serotypes (BoNT/A to BoNT/F) and tetanus toxin (TeTx) are indicated within boxes aimed at their targets (modified from reference 2). 1138 AAEM Case Report #16: Botulism examiner’s hand in response to questions. A relevant finding in the general examination was the presence of multiple scars and scrapes throughout the skin of the abdomen and limbs. In addition, he had an abscess in his right shoulder. The neurologic examination showed very sluggish pupillary response to light, limitation of horizontal gaze, and inability to move the eyes vertically or to maintain the eyes opened. There was moderate weakness of facial and tongue movements. The tone and muscle strength were decreased in the upper and lower extremities but there was no muscle atrophy or fasciculations. The weakest muscles were the deltoid and iliopsoas muscles, which barely provided strength to overcome gravity. Deep tendon reflexes were mildly decreased in the upper extremities but were normal in the lower extremities. Plantar responses were flexor. Sensory examination was normal and coordination could not be properly assessed. On admission, the patient had a mildly elevated white blood cell count at 15,000/ mm3 and a low serum albumin level at 3 g/100 mL. Cultures from the abscess discharge revealed the presence of Staphylococcus aureus sensitive to ciprofloxacin and cephalexin (Keflex). Laboratory Tests. Electrodiagnostic Examination. The electrodiagnostic study was performed using a Nicolet Viking IV electromyograph (Nicolet Biomedical Inc., Madison, WI). Motor and sensory nerve conduction velocities were measured using conventional techniques and surface electrodes for stimulation and recording. Repetitive stimulation was performed in the right median nerve stimulating at wrist and recording from the abductor pollicis brevis (APB) muscle. Needle electromyography (EMG) was carried out using a disposable monopolar needle electrode (Teca Corp., Pleasantville, NY). Stimulated single-fiber EMG (SSFEMG) was performed in the right deltoid muscle using microstimulation of distal nerve branches with a monopolar needle. Recording and analysis of SSFEMG data were done as previously described.25 Nerve conduction studies. Motor nerve conduction velocity in the right median nerve was normal at 62.5 m/s with a compound muscle action potential (CMAP) amplitude of 5.2 mV peak-to-peak. The Fwave latency was also normal at 28.3 ms. The sensory conduction velocity in the right median nerve was normal at 61.5 m/s with a sensory nerve action potential (SNAP) amplitude of 14.1 mV. Stimulation of MUSCLE & NERVE July 2000 the right axillary nerve at Erb’s point with recording from the deltoid muscle resulted in a CMAP of normal latency and decreased amplitude: 4 ms and 2.6 mV peak-to-peak, respectively. Repetitive stimulation. There was no significant decrement of CMAP amplitude during a train of four stimuli delivered to the right median nerve at 2 HZ. Stimulation of the same nerve at 30 HZ with a train of 12 stimuli resulted in a modest increment of CMAP amplitudes of 20% (Fig. 2). Needle EMG. The right first dorsal interosseous, flexor carpi radialis (FCR), and deltoid muscles were studied. There was no evidence of spontaneous activity in any of these muscles. In the FCR and deltoid muscles there were polyphasic motor unit potentials (MUPs). Furthermore, the MUPs were small in amplitude and very short in duration. The pattern of recruitment in the distal muscles was normal. In the deltoid muscle, the pattern of recruitment was reduced, probably as a result of complete blockade of all the nerve terminals of some motor units. This true reduction of MUPs coupled with the low amplitude of distant MUPs allowed the recognition of MUPs located near the needle electrode even during maximal effort. This “rapid firing” of short-duration MUPs provided a seemingly combined myopathic and neurogenic characteristic to the MUP recruitment pattern (Fig. 3). Stimulated single-fiber EMG. A total of 23 measurements of jitter were performed during stimulation at 10 HZ, 20 HZ, and 40 HZ. The mean consecutive difference (MCD) was increased at these three frequencies of stimulation. There was no improvement of jitter with high frequency of stimulation. The MCD at 10 HZ was 41.7 ± 22.1 ms (n = 10), at 20 HZ was 40.2 ± 7.7 ms (n = 5), and at 40 HZ was 44.6 ± 13.9 ms (n = 3) (Fig. 4). Interpretation. The primary feature of the electrodiagnostic evaluation in this case was not pro- FIGURE 2. Repetitive nerve stimulation test. (A) Stimulation of the right median nerve at 2 HZ showed no significant decrement. (B) Stimulation of the same nerve at 30 HZ resulted in a moderate incremental response. AAEM Case Report #16: Botulism FIGURE 3. Needle electromyographic findings. (A) Myopathic motor unit potentials (MUPs); (decreased amplitude, short duration) recorded from the right deltoid muscle. Because of the severe reduction of amplitudes of distant MUPs, one of the MUPs can be distinguished from background activity even during activation at 25 HZ. (B) Recording from the same muscle of agematched control subjects. vided by the repetitive stimulation but rather by the needle EMG. It was shown that, even in severely affected muscles, the pattern of recruitment of MUPs was normal or only moderately reduced. This suggests that the patient’s weakness was not due to an abnormality of the central nervous system or a dysfunction of large-diameter motor nerve fibers. The absence of involvement of large-diameter motor nerve fibers was further supported by the normal motor conduction velocities and normal F-wave latencies in affected muscles. On the other hand, the marked reduction of MUP duration pointed to an abnormality of the distal motor branch, the neuromuscular junction (NMJ), or the muscle fiber itself. Acute diseases affecting distal motor nerve fibers usually are associated with prolongation of motor FIGURE 4. Stimulated single-fiber EMG. Example of marked increment of jitter in a single muscle fiber recorded from the right deltoid muscle. MUSCLE & NERVE July 2000 1139 predominance type 1 fibers (about 80%). In addition, there were rare necrotic and degenerating fibers and macrophage infiltration. Electron microscopy showed no ultrastructural abnormalities of the muscle fibers or motor endplates. However, several endplates were found to be unopposed by nerve terminals indicating acute denervation. In vitro studies with intracellular microelectrodes revealed severe reduction of the EPP quantal content (4.82 ± 3.84 in the patient vs. 22.2 ± 2.8 in control subjects) (Fig. 5). In addition, both the amplitudes and frequencies of miniature endplate potentials (MEPPs) were reduced (MEPP amplitudes: 0.34 ± 0.1 mV in the patient and 0.81 ± 0.08 mV in control subjects; MEPP frequencies: 2.3 ± 0.4/min in the patient and 4.0 ± 5.1 /min in control subjects) (Fig. 6). The reduction of the EPP quantal content confirmed the presence of presynaptic failure, whereas the additional reduction of amplitudes and frequencies of MEPPs were consistent with underlying denervation Thus, the findings of the in vitro physiology were in agreement with the results of the structural studies and consistent with acute neurogenic atrophy. During the 12day hospitalization there was progressive improvement of cranial nerve function and pulmonary function tests. However, the patient remained dependent on mechanical respiration and the proximal weakness in the limbs persisted. On day 9 of admission the patient had a tracheostomy for continued ventilatory support. Three days later he was discharged to a long-term facility. distal latencies and that was not present in this case. A dysfunction of the muscle fiber could result from either an abnormality of the muscle fiber membrane, as in periodic paralysis, or muscle fiber destruction, as in an acute myopathy. Periodic paralysis and other channelopathies are long-standing congenital diseases that cause episodic and transient weakness. None of these clinical features were present in the patient. Acute myopathies are associated with intense spontaneous activity (fibrillation and positive sharp waves) and that was not observed in this case. Diseases of the NMJ can be either presynaptic or postsynaptic. In both situations SSFEMG jitter is increased as it was in the patient. In acute postsynaptic diseases, such as in myasthenia gravis (MG) or during the effect of a paralyzing muscular agent like vecuronium, the release of neurotransmitter is normal. When the release of neurotransmitter is normal and the safety margin of the NMJ is diminished, repetitive stimulation at slow rates elicits marked decrement.27 Because this was not observed in the patient the repetitive stimulation at slow rates suggested a presynaptic failure. Presynaptic failure was further supported by the finding of CMAP increment at fast rates of stimulation. The two most common presynaptic disorders of neuromuscular transmission are Lambert–Eaton syndrome (LES) and botulism. In both conditions CMAP amplitudes are small. However, in LES, repetitive stimulation at fast rates results in prominent CMAP increment, which is usually more than 100%.24 On the other hand, in botulism, the increment is ordinarily less than 100%, as it was in the patient. In summary, the electrodiagnostic study was consistent with a presynaptic failure of neuromuscular transmission and further suggested that the presynaptic failure was most likely due to botulism. Outcome. Two months later, the patient was discharged from the long-term facility in a wheelchair. He started ambulating with a walker 4 months later. Additional recovery occurred during the following 8 months, but he continued experiencing some de- Clinical Course. The serum of the patient tested negative for acetylcholine receptor (AChR) antibodies. However, the mouse bioassay performed by the California State Department of Health Services using serum of the patient revealed the presence of Botulinum toxin A. The patient was initially treated with penicillin and trivalent botulism antitoxin (A, B, and E). However, an immediate improvement was not observed. Later, the patient developed bilateral lobe consolidations and the antibiotic treatment was changed to clindamycin and piperacillin to cover Gram-negative organisms. On day 6 of admission the patient had a muscle biopsy (left anconeus muscle) to search for possible additional causes of weakness. Light microscopy revealed the presence of a moderate number of angular atrophic fibers with a clear FIGURE 5. Nerve evoked endplate potentials (EPPs). (A) Superimposed consecutive EPPs elicited in the biopsy of the patient by microstimulation of the motor nerve terminal branch at 1 HZ. Note the marked reduction and variability of EPP amplitudes. (B) Normal EPPs recorded from a muscle biopsy of a control subject. 1140 AAEM Case Report #16: Botulism MUSCLE & NERVE July 2000 FIGURE 6. Spontaneous miniature endplate potentials (MEPPs). (A) Examples of reduced amplitude MEPPs. There is a homogeneous distribution of MEPP amplitudes. Note the absence of large-amplitude MEPPs or “giant MEPPs.” (B) Amplitude distribution of MEPPs displayed in (A). gree of shortness of breath up to 2 years after the onset of symptoms. DISCUSSION This case exemplifies the apparent discrepancy between the severity of symptoms and the rather mild electrodiagnostic abnormalities often encountered in botulism. Patients with botulism are usually first seen by the electrodiagnostic medicine consultant in the intensive care unit while they are on mechanical ventilatory support, and the electrophysiologic findings in these patients are often unimpressive. Motor and sensory conduction velocities, including distal motor and F-wave latencies are invariably normal. This is an important point because it helps to distinguish botulism from an acute demyelinating neuropathy or Guillain–Barré syndrome (GBS). Clinically, GBS is one of the most important differential diagnoses of botulism and the electrodiagnostic study plays a fundamental role in the differentiation of one from the other. The CMAP amplitudes in botulism are usually diminished, but the reduction of CMAP amplitudes in this condition may be mild or restricted to proximal muscles, which are as a rule those most severely affected. This certainly may be missed if the recording of CMAP amplitudes is limited to distal muscles, as is usually the case with conventional nerve conduction velocity studies. Reduction of CMAP amplitudes is also seen in axonal AAEM Case Report #16: Botulism neuropathy and this can lead to potential diagnostic problems. However, in axonal neuropathy there is often secondary demyelination that may result in additional abnormalities of the nerve conduction velocity study, including temporal dispersion and fragmentation of CMAPs and prolongation of F-wave latencies.12 These findings are distinctively absent in botulism. More importantly, because the pathogenic mechanism of neuropathy is length dependent, the abnormalities in this condition (i.e., reduction of CMAP amplitudes) are more pronounced in distal muscles, whereas in botulism the abnormalities are more prominent in proximal muscles.29 Repetitive nerve stimulation is considered an important part of the electrodiagnostic study of human botulism.16,36 In this case report, a modest CMAP increment in response to high-frequency repetitive nerve stimulation suggested presynaptic failure and was consistent with the diagnosis of botulism. However, in the authors’ experience, which is based mostly on intoxications due to Botulinum toxin type A, incremental responses to fast-rate repetitive nerve stimulation are often missing, even after studying multiple nerves in serologically proven cases. This observation is in sharp contrast to the report by Cornblath and colleagues showing positive incremental responses to high-frequency repetitive stimulation in 92% of patients with infant botulism.7 It should be noted that 96% of the cases reported by these investigators were due to Botulinum type B. Cherington reported that posttetanic facilitation is seen more often in type B botulism (84% of patients) than in type A (62% of patients).6 It is tempting to speculate that the larger percentage of incremental responses in patients intoxicated with type B in comparison with that of patients intoxicated with type A may be due to the fact that neurotoxin types A and B have different molecular targets at the nerve terminal. Fakadej and Gutmann communicated that long runs of repetitive stimulation at fast rates (40– 50 HZ for 10 s) often induce prominent incremental responses in adult and infant forms of botulism.13 However, this observation was also made in cases with patients intoxicated with neurotoxin type B; therefore, the explanation just provided may also apply to this situation. Several cases of wound- and food-borne botulism due to toxin type A have been investigated with intracellular microelectrode recordings.21,28 The most constant findings were the reduction of EPP quantal content and decrease of MEPP amplitudes and frequencies. These findings are very similar to those encountered in human denervation,30 suggesting that, in principle, Botulinum type A induces ultrater- MUSCLE & NERVE July 2000 1141 minal pharmacologic denervation. In contrast, in type B intoxication there is less effect on MEPP amplitudes and frequencies but equal or even more reduction of EPP quantal content than in type A.28 In addition, in type B there is marked desynchronization of EPP onsets or EPP jitter.15 All these findings suggest that toxin type B fundamentally interferes with the release of synaptic vesicles primed by the impulse-evoked peak entry of Ca2+ into the nerve terminal. Because tetanic stimulation increases the entry of Ca2+ into the nerve terminal it is understandable that type B intoxication results more often in incremental responses than type A. Unfortunately, even when an incremental response to high-frequency repetitive stimulation is unambiguously demonstrated, the diagnosis of botulism cannot be established with certainty because incremental responses to tetanic stimulation can be seen in many conditions. Prominent incremental responses to tetanic stimulation (>100% increment CMAP amplitude) are encountered, almost exclusively in LES. This feature can help to differentiate LES from botulism, because in botulism large incremental responses are seldom observed. Nevertheless, modest increments are occasionally detected in LES as well, which can lead to potential diagnostic problems. In a recent study, Tim and associates reported that only 37% of their LES patients had 100% CMAP amplitude potentiation in the three muscles tested.40 Furthermore, 78% of their patients had 100% CMAP facilitation in the abductor digiti quinti muscle, whereas only 24% had a similar degree of facilitation in the trapezius muscle. The higher frequency of facilitation in distal muscles of LES patients is important because the opposite pattern occurs in botulism where the larger frequency of facilitation involves proximal muscles. Tim and colleagues also reported that 98% of their LES patients showed a decremental response to slow-rate repetitive stimulation in muscles of the hand.40 This finding is also at variance with botulism where decrement in response to slow-rate repetitive nerve stimulation is not consistent. The inconsistency of decrement in botulism may result from the impairment of synaptic vesicle fusion induced by the neurotoxin. Because the decrement at slow rates of stimulation results from transient depletion of synaptic vesicles at the active zones, an impairment of vesicle fusion may prevent vesicle depletion and consequently the decrement. A careful analysis of the configuration and pattern of recruitment of MUPs in clinically affected muscles is one of the most useful parts of the electrodiagnostic assessment of botulism. Due to the 1142 AAEM Case Report #16: Botulism complete blockade of neuromuscular transmission in many muscle fibers the number of muscle fibers contributing to the electrical field generated by the whole motor unit decreases and the MUP duration falls. In moderately affected muscles the number of motor units is not diminished and therefore the pattern of MUP recruitment is normal. However, in severely affected muscles all the muscle fibers of a motor unit near the needle electrode may be blocked, which may result in an apparent decrease in the recruitment of MUPs. Furthermore, polyphasic MUPs are common because of the immediate change of the motor unit architecture and subsequent reinnervation induced by the toxin. Thus the findings of the needle examination are best described as comprising a combination of myopathic and neuropathic abnormalities. Although these electrodiagnostic features are the most constant findings in botulism, they are also the least specific. Therefore, it is advisable to include histologic assessment with muscle biopsy when the diagnosis of botulism is made only on the basis of the electromyographic pattern. This should appropriately exclude the possibility of an underlying myopathic process. Potential Pitfalls. The following situations can pose special diagnostic problems (Table 1). Miller–Fisher variant of GBS vs. botulism. Some of the author’s patients were initially thought to have Miller–Fisher syndrome (MFS). Both MFS and botulism classically present with hyporeflexia and generalized weakness with predilective involvement of cranial nerves. However, the nerve conduction velocity studies in MFS show a characteristic absence of distal sensory evoked responses that is not seen in botulism.14,37 Furthermore, the recruitment of MUPs in affected muscles is diminished in MFS but is normal in botulism. The presence of anti-GQ1b antibodies in MFS or the positive mouse bioassay in botulism can provide additional help for differentiating these conditions. Normal vs. abnormal electrodiagnostic study in botulism. Electrodiagnostic abnormalities in mild cases of botulism may be quite subtle and difficult to detect with routine studies. However, a careful electrodiagnostic evaluation should uncover reduction of CMAP amplitudes and short-duration MUPs in affected muscles. Motor axonal neuropathy combined with myasthenia vs. botulism. In principle, a combination of motor neuropathy and myasthenia may reproduce all the clinical symptoms encountered in botulism, including hyporeflexia and weakness of bulbar musculature. The electrodiagnosis in a hypothetical case of a MUSCLE & NERVE July 2000 Table 1. Electrodiagnosis of botulism and related disorders. NCVs ↓NCV ↓CMAP amplitudes ↓SNAP amplitudes EMG Fibrillation and positive waves Short duration MUPs Myopathic recruitment Repetitive nerve stimulation Decrement (slow rate) Increment (fast rate) Botulism MFS LES Axonal neuropathy + MG AQM Myopathy + axonal neuropathy − + − + + ++ − ++ − + ++ + − ++ − + ++ + + ++ + + − − − + + ++ + + ++ ++ + ++ ++ + + + − − ++ +++ ++ − − − − − AQM, acute quadriplegic myopathy; CMAP, compound muscle action potential; EMG, electromyography; LES, Lambert–Eaton syndrome; MFS, Miller–Fisher syndrome; MG, myasthenia gravis; MUP, motor unit potential; NCV, nerve conduction velocity; SNAP, sensory nerve action potential. combined motor neuropathy and myasthenia may show, as in botulism, reduction of CMAP amplitudes and abnormalities of repetitive nerve stimulation. However, in a motor neuropathy, due to frequent secondary demyelination, additional abnormalities of nerve conduction velocities occur. This includes temporal dispersion and fragmentation of CMAPs and prolongation of F-wave latencies, which are, as a rule, absent in botulism. The presence of increment to high-rate repetitive nerve stimulation may favor botulism, but this finding may be present in other conditions such as LES, myasthenia,20 and even in motor neuron disease.33 Conversely, the absence of increment or even the finding of decrement in response to fast repetitive stimulation does not rule out the diagnosis of botulism. Unfortunately, other laboratory studies may not provide additional help. For instance, as much as 15% of patients with generalized myasthenia do not have serum antibodies against the AChR,41 and only 33% of patients with wound botulism have seropositive mouse bioassay for botulinum toxin.23 Ultimately, a motor point muscle biopsy with microelectrode, immunohistochemistry, and ultrastructure of the NMJ and motor nerves may be necessary to establish the diagnosis. Acute quadriplegic myopathy in critically ill patients vs. botulism. There have been numerous reports describing persistent quadriparesis in critically ill patients, usually following the administration of nondepolarizing neuromuscular blocking agents alone or in combination with steroids.3,8 This condition is poorly understood. The electrodiagnotic findings in acute quadriplegic myopathy (AQM) are often strikingly similar to those seen in botulism. The similarities include reduction of CMAP amplitudes with normal sensory potentials and a myopathic EMG pattern.4,19 In addition, both can show variable de- AAEM Case Report #16: Botulism grees of spontaneous EMG activity (fibrillation potentials and positive waves), absence of creatine kinase (CK) elevation, or unrevealing muscle biopsy. In the authors’ experience, the spontaneous activity is more intense in AQM and repetitive nerve stimulation at fast rates is more likely to induce incremental responses in botulism. Furthermore, direct muscle stimulation often reveals electrical inexcitability in AQM but not in botulism.35 Proximal myopathy combined with neuropathy vs. botulism. The combination of myopathy and neuropathy, although infrequent, does happen occasionally, particularly if both conditions represent the neurologic manifestation of a paraneoplastic syndrome or a connective tissue disease.5,22 Electrodiagnosis usually demonstrates, as in botulism, reduced CMAP amplitudes and normal recruitment of shortduration MUPs. Histologic examination with conventional muscle biopsy may be sufficient to differentiate these two clinical situations. REFERENCES 1. Arnon SS. Infant botulism. In: Feigin RD, Cherry JD, editors. Textbook of pediatric infectious diseases, 3rd ed. Philadelphia: Saunders; 1992. 2. Bark IC, Wilson MC. Regulated vesicular fusion in neurons: snapping together the details. Proc Natl Acad Sci USA 1994; 91:4621–4624. 3. Barohn RJ, Jacson CE, Rogers SJ, Ridings LW, McVey AL. Prolonged paralysis due to nondepolarizing neuromuscular blocking agents and corticosteroids. Muscle Nerve 1994;17: 647–654. 4. Bird SJ, Macking GA, Schotland DL, Raps EC. Acute myopathic quadriplegia: a unique syndrome associated with vecuronium and steroid treatment. Muscle Nerve 1992;15:1208. 5. Carsons S. The association of malignancy with rheumatic and connective tissue diseases. Semin Oncol 1997;24:360–372. 6. Cherington M. Electrophysiologic methods as an aid in the diagnosis of botulism: a review. Muscle Nerve 1982;5(suppl): S28–S29. MUSCLE & NERVE July 2000 1143 7. Cornblath DR, Sladky JT, Sumner AJ. Clinical electrophysiology of infantile botulism. Muscle Nerve 1983;6:448–452. 8. Danon MJ, Carpenter S. Myopathy with thick filament (myosin) loss following paralysis with vecuronium during steroid treatment. Muscle Nerve 1991;14:1131–1139. 9. Davis JB, Mattman LH, Wiley M. Clostridium botulinum in a fatal wound infection. JAMA 1951;146:646–648. 10. Davis LE. Botulinum toxin—from poison to medicine. West J Med 1993;158:25–29. 11. Dodds KL. Worldwide incidence and ecology of infant botulism. In: Hauschild AHW, Dodds KL, editors. Clostridium botulinum: ecology and control in foods. New York: Marcel Dekker; 1992. 12. Dyck PJ, Johnson WJ, Lambert EH, O’Brien PC. Segmental demyelination secondary to axonal degeneration in uremic neuropathy. Mayo Clin Proc 1971;46:400–431. 13. Fakadej AV, Gutmann L. Prolongation of post-tetanic facilitation in infant botulism. Muscle Nerve 1982;5:727–729. 14. Fross RD, Daube JR. Neuropathy in the Miller Fisher syndrome: clinical and electrophysiologic findings. Neurology 1987;37:1493–1498. 15. Gansel M, Penner R, Dreyer F. Distinct sites of action of clostridial neurotoxins revealed by double-poisoning of mouse nerve terminals. Pflugers Arch 1987;409:533–539. 16. Guttman L, Pratt L. Pathophysiologic aspects of human botulism. Arch Neurol 1976;33:175–179. 17. Hatheway CL. Botulism: the present state of the disease. Curr Top Microbiol Immunol 1995;195:55–75. 18. Hauschild AHW. Epidemiology of human foodborne botulism. In: Hauschild AHW, Dodds KL, editors. Clostridium bolutinum: ecology and control in foods. New York: Marcel Dekker; 1992. 19. Hirano M, Ott BR, Raps EC. Acute quadriplegic myopathy: a complication of treatment with steroids, nondepolarizing blocking agents or both. Neurology 1992;42:2082–2087. 20. Ismail MK, Midani HA. Post-exercise facilitation in myasthenia gravis [abstract]. Muscle Nerve 1998;21:1600. 21. Lambert EH, Engel AG, Cherington M. End-plate potentials in human botulism [abstract]. Excerpta Medica 1974;334:65. 22. Lucchinetti CF, Kimmel DW, Lennon VA. Paraneoplastic and oncologic profiles of patients seropositive for type 1 antineuronal nuclear autoantibodies. Neurology 1998;50:652–657. 23. MacDonald L, Rutherford GW, Friedman SM, Dietz JR, Kaye BR, McKinley GF, Tenney JH, Cohen ML. Botulism and botulism-like illness in chronic drug abusers. Ann Intern Med 1985;102:616–618. 24. Maddison P, Newsom-Davis J, Mills KR. Distribution of electrophysiological abnormality in Lambert–Eaton myasthenic syndrome. J Neurol Neurosurg Psychiatry 1998;65:213–217. 25. Mandler R, Maselli RA. Single fiber EMG in wound botulism. Muscle Nerve 1996;19:1171–1173. 26. Maselli RA. Pathogenesis of human botulism. Myasthenia gravis and related diseases. Ann NY Acad Sci 1998;841: 122–139. 27. Maselli RA. Electrodiagnosis of disorders of neuromuscular 1144 AAEM Case Report #16: Botulism 28. 29. 30. 31. 32. 33. 34. 35. 36. 37. 38. 39. 40. 41. 42. transmission. Myasthenia gravis and related diseases. Ann NY Acad Sci 1998;841:696–711. Maselli RA, Burnett ME, Tonsgard JH. In vitro microelectrode study of neuromuscular transmission in a case of botulism. Muscle Nerve 1992;15:273–276. Maselli RA, Ellis W, Mandler RN, Sheikh F, Senton G, Knox S, Salari-Namin H, Agius M, Wollman RL, Richman DP. Cluster of wound botulism in California: clinical, electrophysiologic, and pathologic study. Muscle Nerve 1997;20:1284–1295. Maselli RA, Wollman RL, Leung C, Distad B, Palombi S, Richman DP, Salazar-Grueso EF, Roos RP. Neuromuscular transmission in amyotrophic lateral sclerosis. Muscle Nerve 1993; 16:1193–1203. Midura TF, Arnon SS. Infant botulism: identification of Clostridium botulinum and its toxin in faeces. Lancet 1976;ii: 934–936. Montecucco C, Schiavo G. Structure and function of tetanus and botulinum neurotoxins. Q Rev Biophys 1995;28:423–472. Norris FH. Adult spinal neuron disease progressive muscular dystrophy (Aran’s disease) in relation to amyotrophic lateral sclerosis. In: Vinken PJ, Bruyn GW, editors. Handbook of clinical neurology. Vol. 22. New York: Elsevier; 1975. p 1–56. Pickett J, Berg B, Chaplin E, Brunstetter MA. Syndrome of botulism in infancy: clinical and electrophysiologic study. N Engl J Med 1976;295:770–772. Rich MM, Teener JW, Raps EC, Schotland DL, Bird SJ. Muscle is electrically inexcitable in acute quadriplegic myopathy. Neurology 1996;46:731–736. Rivner MH, Swift TR. Electrical testing in disorders of neuromuscular transmission. In: Brown WF, Bolton CF, editors. Clinical electromyography. Newton, MA: ButterworthHeinemann; 1993. p 625–651. Sauron B, Bouche P, Cathala HP, Chain F, Castaigne P. Miller Fisher syndrome: clinical and electrophysiologic findings. Neurology 1984;34:351–364. Sharma SK, Singh BR. Hemagglutinin binding mediated protection of botulinum neurotoxin from proteolysis. J Nat Toxins 1998;7:239–253. Singh BR, Li B, Read D. Botulinum versus tetanus neurotoxins: why is botulinum neurotoxin but not tetanus neurotoxin a food poison? Toxicon 1995;33:1541–1547. Tim RW, Massey JM, Sanders DB. Lambert–Eaton myasthenic syndrome (LEMS) clinical and electrodiagnostic features and response to therapy in 59 patients. Myasthenia gravis and related diseases. Ann NY Acad Sci 1998;841:823–826. Vincent A, Li Z, Hart A, Barrett-Jolley R, Yamamoto T, Burges J, Wray D, Byrne N, Molenaar P, Newsom-Davis J. Seronegative myasthenia gravis: evidence for plasma factor(s) interfering with acetylcholine receptor function. Ann NY Acad Sci 1993;681:529–538. Weber JT, Goodpasture HC, Alexander H, Werner SB, Hatheway CL, Tauxe, RV. Wound botulism in a patient with a tooth abscess: case report and review. Clin Infect Dis 1993;16: 635–639. MUSCLE & NERVE July 2000