Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Heart failure wikipedia , lookup
Drug-eluting stent wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
Lutembacher's syndrome wikipedia , lookup
History of invasive and interventional cardiology wikipedia , lookup
Cardiac surgery wikipedia , lookup
Antihypertensive drug wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
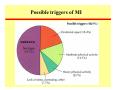
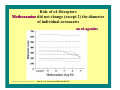
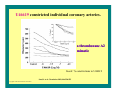
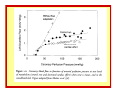
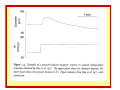
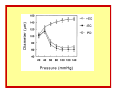
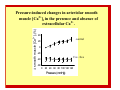
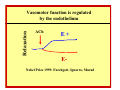
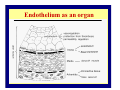
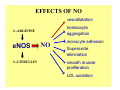
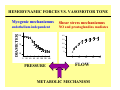
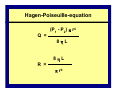
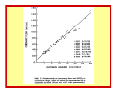
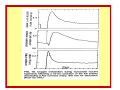
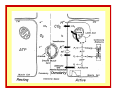
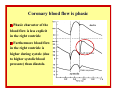
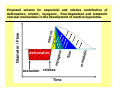
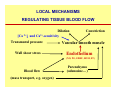
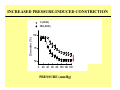
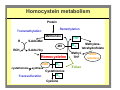
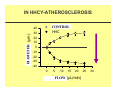
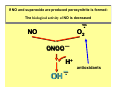
PATHOPHYSIOLOGY OF CORONARY CIRCULATION and MICROCIRCULATION Akos Koller DEPARTMENT OF PATHOPHYSIOLOGY AND GERONTOLGY FACULTY OF MEDICINE UNIVERSITY OF PÉCS 2009 Angina pectoris ISCHEMIC HEART DISEASES myocardial ischemia, infarction • Develops due to (absolute or relative) tissue hypoperfusion • Reduced myocardial oxygen supply • Increased oxygen demand • Accumulation of tissue metabolites imbalance between oxygen demand and supply MYOCARDIAL INFARCTION Myocardial infarction is an irreversible damage/necrosis of a given region of the myocardium due to the long-term critical reduction of the coronary blood flow. CAUSES OF REDUCED MYOCARDIAL OXYGEN SUPPLY Partial or complete intraluminal occlusion of coronary vessels: • atherosclerotic plaque • thrombus • aggregation of platelets • coronary embolism • coronary aneurysm • arteritis (polyarteritis nodosa) Possible triggers of MI unknown CLINICAL FORMS OF ISCHEMIC HEART DISEASE • • • • • • • • • stable pectoral angina (effort angina): silent ischemia acute coronary syndromes unstable pectoral angina myocardial infarction non-Q myocardial infarction infarction with ST-elevation acute heart failure of ischemic origin sudden cardiac death of ischemic origin STABLE PECTORAL ANGINA SYNDROME Caused by reversible myocardial ischemia. A clinical syndrome associated with blunt chest pain, sweating, dyspnoe (breathlessness), fear of death, ECG abnormalities (ST,T). Initiated by: • physical stress • emotional stress • at rest may also develop • last no longer than 15 minutes • ceases upon rest or nitroglycerin (nitrate) treatment STABLE PECTORAL ANGINA SYNDROME Caused by reversible myocardial ischemia. A clinical syndrome associated with blunt chest pain, sweating, dyspnoe (breathlessness), fear of death, ECG abnormalities (ST,T). Initiated by: • physical stress • emotional stress • at rest may also develop • last no longer than 15 minutes • ceases upon rest or nitroglycerin (nitrate) treatment !! Evaluation of the risk of patients suffering from coronary dysfunction physical examination ECG laboratory tests functional examinations exercise test (ergometry) thallium heart scan exercise echocardiography coronarography ST-segment depression Causes of dysfunction of coronary circulation atherosclerosis, thrombus, platelets physical obstruction (large vessels) Angiogram of a narrowing coronary artery. (plaque disruption) Davies, Heart 83:361 (2000) Atherosclerosis funtional constriction reduced diameter (resistance vessels) Q= 4 r Going toward the capillaries: • the total cross-section of vessels increases • the range of change in diameter increases (2-5% to 60-80%) The metabolism of tissue depends on the blood (oxygen ) supply, thus the healthy structure and function of microvessels (microcirculation) are utmost important If the blood supply is not sufficient the pumping function of the heart become reduced (heart failure) TREATMENT OF STABLE ANGINA PECTORIS • • • • • • • Aspirin (inhibits platelet aggregation) Beta-receptor blockers Nitrites and nitrates Calcium antagonists Statins (inhibit cholesterol build up) ACE - inhibitors Other drugs Mechanisms determining coronary circulation THE SPECIAL FUNCTION OF THE HEART IS ENSURED BY ITS SPECIAL CIRCULATION The pump function requires energy. This energy derives from the metabolism of the heart muscle. This metabolism primarily depends on the O2 supply and therefore on the coronary microcirculation. The blood supply of the heart, nutrition and oxygen needs The heart is an obligate aerobic organ The number of mitochondria in the cardiac muscle fibers is significantly greater as compared to other types of muscles. Close to one third of the total cardiac mass is mitochondrion. The usable glycogen storage in the heart is minimal The O2 bond to the myoglobin can provide O2 only for short period of time Therefore, the functioning heart needs continuous blood supply OXYGEN CONSUMPTION (mVO2) OF THE HEART At “rest” the mVO2 is 8-10 mL/100g/min. (for left ventricle ) The weight of heart in adult man is 300 g, thus mVO2 at “rest” is 25-30 mL, which is 12 % of the total (250 ml) mVO2 of the organism. RELATIONSHIP BETWEEN O2 CONSUMPTION AND FUNCTION OF THE HEART • Contraction of the heart generates pressure and kinetic energy. •The major part of mVO2 is utilized to generate pressure and to a lesser degree kinetic energy Wall stress! O2 CONSUMPTION OF THE HEART CAN INCREASE MULTIPLE TIMES to physical activity, but also in response to emotional excitements In trained athletes it can rich 65-70 mL/100g/min (from 1520%) At maximal physical activity the O2 consumption can increase to 7 times of resting condition (for short time) Positive inotropes (e.g. cathecolamines) increase the energy demand of the heart, even if the mechanical efficiency do not increase O2 CONSUMPTION OF THE HEART CAN INCREASE MULTIPLE TIMES In resting conditions cardiac O2 extraction (AVdO2) is larger than other organs have. Coronary venous O2 saturation: ~ 25% 25 (from 95-100%) The venous pO2 ~20-Hgmm (vs. 95-100%), Thus O2 extraction can increase just a little bit ! Thus in case of increased O2 demand: CORONARY BLOOD FLOW MUST INCREASE!! CORONARY BLOOD FLOW (CBF) At rest: 180-240 ml/min At maximum: 900-1200 ml/min The resistance segments of the coronary circulation: small arteries, arterioles, precapillary sphincters(?) have substantial basal tone The dilation of small vessels reduces the vascular resistance to 1/5-1/7! The coronary blood flow is phasic! Systole: no coronary blood flow! (or „negative flow”) Diastole: coronary flow is high Systole: 0,3 s Diastole: 0,5 s IF THE HR INCREASES FROM 70/MIN TO 180/MIN the diastolic perfusion time decreases from 35 s to 24 s in a minute The transmural pressure in the coronary wall is determined by: THE INTRALUMINAL AND THE EXTRALUMINAL PRESSURES! (it is different in the right and left ventricle!) NUTRIENTS AND OXYGEN CONSUMPTION The nutrients of cardiac muscle: glucose free fatty acid lactic acid ketone bodies aminoacids The use of nutrients depends on their concentrations in the blood THE GREAT O2 DEMAND OF THE CARDIAC MUSCULAR FIBRES IS ENSURED BY THE RICH VASCULAR SYSTEM OF THE CARDIAC MUSCLE AORTA Anatomy of the coronary circulation The right and left coronaries originate behind the sac after the aortic valve There is a huge individual variability in the ramification and the supplied area Anatomy of the coronary circulation arteries two main branches (circumflex, descendens), then additional superficial arterial branches, then intramural arteries arterioles intramural, subepi-, subendocapillaries (1 muscular fibre/1 capillary: O2-diffusion) venules veins Characteristics of the coronary circulation The circulatory transit time in the coronaries (the time needed for the red blood cells to get from the arterial side to the venous side) is 6-8 sec at rest. The transit time during physical activity is much less. Despite of the rich vascular system of the heart muscle, there are no collaterals (in humans) between the large coronary branches and the smaller arteries, arterioles. Clinical significance: In humans, the continuous blood flow is always endangered. The leading cause of death: failure of the left ventricle’s blood flow supply. Clinical significance: this may arise from • restriction of the lumen or total occlusion, • the decreased vasomotor dilator capacity of the resistance vessels Consequence: ischemia and heart muscle injury, necrosis the flow of the injured area is only 10 % of the original in case of acute occlusion: ischemia, infarction If the occlusion develops gradually, there is a chance to develop anastomosis, therefore the symptoms of the occlusion are less severe Intraluminal pressure is different in the right and left ventricle! Systolic blood pressure in the right ventricle (and ventricular wall) is only ~ 25 mmHg therefore it has only little effect on the transmural pressure and the diameter of the arteries Systolic blood pressure in the left ventricle (and ventricular wall) is ~ 120 mmHg and this pressure can obstruct the arteries. Therefore coronary blood flow is determined by the intraluminal pressure (which is identical to the aortic pressure) and the pressure generated by the heart muscle The left ventricle receives its blood flow mainly during diastole even negative blood flow can be observed: for a short time blood flows from the coronaries back to the aorta during systole coronary blood flow is minimal in the left ventricular wall coronary blood flow is high during diastole Resting frequency (HR): 70/minute. systole: 0,3 sec, diastole: 0.5 sec. Total blood flow of the left ventricle: 60 mL/min (50 mL under diastole) • If HR increases, the diastolic period of time decreases limiting the increasing of flow •If HR exceeds 180/min the phasic flow may become impaired Subepicardium: Capillary system of the myocardium high density, capillaries are between the muscle fibers almost every muscle fiber has its own capillary it supplies the fibers with sufficient O2 diffusion, even if the O2 demand of the fibers is maximal In case of maximal dilatation: 2500-4000 capillaries/mm3 are open (in working skeletal muscles: 300-400/mm3) The highest capillary density is near to the endocardium of the left ventricle If the ventricular load chronically rises, the ventricular wall becomes thicker (ventricular hypertrophy) Ventricular hypertrophy: capillary density doesn’t follow it, capillary/muscle fiber ratio decreases The O2 and energy supply of the myocardium decreases From here The coronary/peripheral circulation is regulated by the integrated effects of 3 mechanisms: neural - hormonal - local - The vascular resistance is determined by the small arteries and arterioles Diameter of the arterioles is determined by vasoactive agents (among others) Neural regulation Increased activation of the sympathetic nervous system leads to the release of catecholamines, norepinephrine, epinephrine Catecholamine-s (norepinephrine, epinephrine): Vasoconstriction through α1-receptors. In case of maximal stimulation constriction can be 30% if β-receptors are blocked. Vasodilatation through the direct stimulation of β2 receptors If there is a coronary stenosis, maximal sympathetic stimulation can cause death, because it increases the O2 demand of the myocardium Catecholamine-s (norepinephrine, epinephrine): Vasoconstriction through α1-receptors. In case of maximal stimulation constriction can be 30% if β-receptors are blocked. Vasodilatation through the direct stimulation of β2 receptors If there is a coronary stenosis, maximal sympathetic stimulation can cause death, because it increases the myocardial O2 demand NE effects the contractility (HR) and the diameter of coronary vessels Norepinephrine vs. α and β receptors NE (10-7 to 3x10-7 mol/L) elicited dose-dependent dilations of of isolated human coronary arterioles arterioles (n=39) Copyright ©2002 American Heart Association Sun, D. et al. Circulation 2002;106:550-555 Relationship between maximal diameter (passive diameter, PD) and changes in diameter, as percentages of PD, to NE in individual arteries. The data show that the percent increase in vessel diameter was not dependent on vessel size. There were no significant differences in NE-induced dilations between vessels with spontaneous tone and vessels treated with endothelin. Only 2 vessels (average passive diameter 240 µm) responded with a decrease in diameter to NE. r2 equals 0.005, 0.053, and 0.089 (P=NS) for the following NE concentrations: 10-7 mol/L, 2x 10-7 mol/L, and 3x10- 7 mol/L, respectively. Copyright ©2002 American Heart Association Sun, D. et al. Circulation 2002;106:550-555 Changes in diameter of isolated human coronary arterioles in response to NE in absence of endothelium (EC-) (top) and presence of NOS inhibitor L-NNA (bottom). (E-) (L-NNA) Sun, D. et al. Circulation 2002;106:550-555 Copyright ©2002 American Heart Association Role of ß-Receptors Propranolol, Propranolol eliminated coronary dilations to NE. a combined ß1- and ß2adrenoceptor antagonist Copyright ©2002 American Heart Association Sun, D. et al. Circulation 2002;106:550-555 Role of ß-Receptors Practolol did not affect coronary dilations to NE. a ß1-adrenoceptor antagonist Copyright ©2002 American Heart Association Sun, D. et al. Circulation 2002;106:550-555 Role of ß-Receptors Butoxamine eliminated coronary dilations to NE. a ß2-adrenoceptor antagonist In addition, we have found that salbutamol (10-6 mol/L) elicited substantial dilation of human coronary arterioles (60±8 µm, n=5). Sun, D. et al. Circulation 2002;106:550-555 Copyright ©2002 American Heart Association Role of α1-Receptors Methoxamine did not change (except 2) the diameter of individual coronaries an α1-agonists Copyright ©2002 American Heart Association Sun, D. et al. Circulation 2002;106:550-555 U46619 constricted individual coronary arteries. a thromboxane A2 mimetic Insert: % constrictions to U46619 Sun, D. et al. Circulation 2002;106:550-555 Copyright ©2002 American Heart Association A: Upper panel: Reverse transcription-polymerase chain reaction analysis of ß-adrenoceptor mRNA in porcine coronary arterioles and myocardial tissue was performed with the use of gene-specific primers for the ß2-adrenoceptor (ß2-AR) and the ß1-adrenoceptor (ß-1-AR). A, Lower panel: ß2-AR transcripts from the subepicardial (EPI) and subendocardial (ENDO) arterioles were normalized with the corresponding GAPDH transcripts. *P<0.05 vs EPI arterioles. Marker= X174-DNA marker. Copyright ©2004 American Heart Association Hein, T. W. et al. Circulation 2004;110:2708-2712 B: Immunohistochemical analysis of ß2-adrenoceptor (ß2-AR) protein in EPI and ENDO arterioles. Shown as a pseudo-color spectral display. Performed in vessels treated without (–1°) or with (+1°) anti–ß2-AR primary antibody. Level of ß2-AR protein expression was represented by the signal intensity of the color pallet. Copyright ©2004 American Heart Association Hein, T. W. et al. Circulation 2004;110:2708-2712 Conclusions • Human coronary arteries and arterioles dilate in response to norepinephrine via β2receptors located on vascular smooth muscle Schematic representation of adrenergic receptor distribution in the coronary circulation. Endothelium is in light green. Vascular smooth muscle cell layer is in yellow. ß2-adrenoceptor WSS Copyright ©2009 BMJ Publishing Group Ltd. Barbato, E. Heart 2009;95:603-608 Adrenergic receptor balance. Shifting of the adrenergic vasomotor modulation from normal coronary arteries through different stages of coronary diseases. ß2-adrenoceptor Barbato, E. Heart 2009;95:603-608 Copyright ©2009 BMJ Publishing Group Ltd. Hormonal/humoral regulation • • • • • • Estrogen, testosterone, aldosteron, Insulin, thyroxin, ghrelin Catecholamines, angiotensin II ANP/BNP fever etc. Mechanisms involved in the local regulation of (coronary) blood flow: 1. Smooth muscle (Pressure-Myogenic) 2. Endothelium (Shear stress) 3. Parenchyma (Oxygen-Metabolic) 4. Others PRESSURE SENSITIVE MYOGENIC SMOOTH MUSCLE MECHANISM ROLE OF INTRALUMINAL PRESSURE Bayliss 1902: myogenic mechanism 1902 Volume changes (upper trace) and arterial pressure recording (lower trace) from hindlimb of dog with occlusion of the supply artery for 8 s and then for 20 s. Bayliss (from Handbook of Physiology) Autoregulation of the coronary circulation The flow is constant between 60 to 180 Hgmm perfusion pressure. Below 60 Hgmm the flow decreases in subendocardial layer. Control }* 150 80 60 40 -10 10 30 50 70 90 110 130 150 Pressure (mmHg) 100 5 50 -10 10 30 50 70 90 110 130 150 Pressure (mmHg) Myogenic Index Diameter ( µ m) 200 % of passive diameter Passive 100 4 3 2 1 0 -1 -10 10 30 50 70 90 110 130 150 Pressure (mmHg) ∆ smooth muscle [Ca2+]i (%) Pressure-induced changes in arteriolar smooth muscle [Ca2+]i in the presence and absence of extracellular Ca2+. 40 control 20 0 -20 Ca2+ free -40 -60 0 20 40 60 80 100 120 140 Pressure (mmHg) Increases in smooth muscle [Ca2+]i and development of myogenic tone at 80 mmHg as a function of extracellular [Ca2+]. 100 80 50 60 40 25 20 0 0 -4 -3 CaCl2 (log mol/L) -2 ∆smooth muscle 2+ [Ca ]i (%) Myogenic tone (µm) 75 Mechanisms involved in the local regulation of (coronary) blood flow: 1. Smooth muscle (Pressure-Myogenic) 2. Endothelium (Shear stress) 3. Parenchyma (Oxygen-Metabolic) 4. Others Endothelium Endothelium A new organ! Discovered in 1980! Smooth muscle Endothel Discovery of the vasomotor role of endothelium Relaxation Vasomotor function is regulated by the endothelium ACh E+ E- Nobel Prize 1999: Furchgott, Ignarro, Murad Endothelium as an organ The endothelium is a new organ The total mass of the endothelium is about 1.5 kg An endocrine organ, which size and importance similar to the liver EDRF 15 years of research: chemical identification of EDRF: Nitric-oxide (NO) R. Furchgott: endothelium, EDRF, NO L. Ignarro: nitrate compounds, nitroglycerin, NO F. Murad: role of NO vs. cGMP in vasodilation Nobel Prize 1999 nitric-oxide: NO EFFECTS OF NO vasodilatation trombocyte aggregation L-ARGININE eNOS L-CITRULLIN NO monocyte adhesion Superoxide elimination smooth muscle proliferation LDL oxidation NO prevent vascular diseases! www.surgery.usc.edu www.szulo.hu/kids/k39/nikot39.htm www.astrazeneca.fi FUNCTIONS OF VASCULAR ENDOTHELIUM I Release of vasodilator agents Nitric oxide (=EDRF) Prostacyclin (PGI2) Bradykinin EDHF (endothelium-derived hyperpolarizing factor) Release of vasoconstrictor agents Endothelin Angiotensin I (angiotensin II) Protection of vascular smooth muscle vasoconstrictor → to vasodilator stimuli (acetylcholine and serotonin) FUNCTIONS OF VASCULAR ENDOTHELIUM II Antiaggregatory effect Acts via NO (nitric oxide) and PGI2 (prostaglandins) Prevention of coagulation Thromboresistant surface Immune function Supply of antigens to immuncompetent cells Secretion of interleukin I Enzymatic activity Angiotensin-converting enzyme (ACE) Carbonic anhydrase (large amounts in lung endothelium) Growth signal to vascular smooth muscle VEGF (vascular endothelial growth factor) Heparin-like inhibitors of growth Stimuli of NO production 1. Humoral agonists of eNOS increase [Ca2+]i: acetylcholine (M3-receptor), bradykinin, thrombin, substance P, vasoactive intestinal polypeptide (VIP), insulin, histamine) 2. Mechanical agonist (wall shear stress) - flow induced vasodilatation - Mechano-sensitive ion channels, tyrosine kinase, PECAM 3. Endotoxin shock and inflammation (via iNOS) in shock: -lipopolysacharide induced shock -direct reaction to TNF-α from monocytes -results too much NO ->generalized vasodilatation in inflammation: -in reaction to interleukins (e.g. IL-1) and TNF -contributes to reddening (rubor), and local heat (calor) in inflammation 4. Nitrites- sodium nitroprusside etc. Nitric oxide, a gas, as a biological signaling molecule Prostaglandins COX1/2 Endothelium: SHEAR STRESS SENSITIVE MECHANISM Intraluminal flow 1990: Shear stress mechanism Flow-induced dilation in coronary arterioles A 30 CONTROL Control Dilation (µm) L-NNA HHcy 20 ∗ 10 0 -10 0 10 20 30 40 Flow (µL/min) 50 HEMODYNAMIC FORCES VS. VASOMOTOR TONE Myogenic mechanizmus DIAMETER endothelium independent Shear stress mechanizmus NO and prostaglandins mediates 40 100 30 20 75 10 0 50 0 20 40 60 80 100 120 140 PRESSURE 0 10 20 FLOW METABOLIC MECHANISM 30 40 Hagen-Poiseuille-equation (P1 - P2) π r4 Q = 8ηL 8ηL R = π r4 Haemodynamic basis Laplace-Frank law: P×r T= w T P w Wall shear stress (WSS): 4ηQ WSS = πr 3 dv WSS = 4η dr 50 µm SCELETAL MUSCLE MICROCIRCULATION Role of mechanosensitive mechanisms • The pressure and shear stress sensitive mechanisms are important in the optimization of microvascular network function to deliver blood flow to tissues. • Minimal energy loss Mechanisms involved in the local regulation of (coronary) blood flow: 1. Smooth muscle (Pressure-Myogenic) 2. Endothelium (Shear stress) 3. Parenchyma (Oxygen-Metabolic) 4. Others PARENCHYMA METABOLIC MECHANISM ”OXYGEN” SENSITIVE Metabolic mechanisms Metabolites from the functioning myocardium have vasomotor effects (1860) „Metabolic” vasoactive substances PO2 ↓ PCO2 [H+] ↑ Adenosine ATP ischaemia Change in diameter (%) Change in diameter (%) Arteries Arterioles 35 30 25 } 20 15 * ADO 10 5 0 -5 -10 -9 -8 -7 -6 -5 -4 40 35 30 25 NE 20 15 10 5 0 -5 -10 -9 -8 -7 -6 Log dose (M) -5 -4 Reactive hyperemia • substantial increase in blood flow (due to dilation of arterioles) following arterial occlusion 1867: Gaskell 1902: Bayliss 1912: Anrep Folkow, Gregg, Coffman, Berne, Rubio, Olsson, Belloni, Sparks, and many others who are also here today Flow/Diameter Reactive hyperemia: substantial increase in blood flow (due to dilation of arterioles) following arterial occlusion occlusion release Time Olsson RA.: Myocardial reactive hyperemia. Circ Res 37: 263-270., 1975. (present in isolated isolated heart!) RH O2 sat. O2 fel. Mechanisms eliciting reactive hyperemia Neuro-humoral factors Tissue factors • neural tone • circulating hormones • substances in the plasma • etc. • adenosine • pO2 decreases • hyperosmolality • ATP-K+ channels • free radicals • etc. Mechanosensitive vascular mechanisms • pressure-induced • flow-dependent • stretch-induced • cell deformation • etc. Coronary blood flow is phasic Phasic character of the blood flow is less explicit in the right ventricle Furthermore blood flow in the right ventricle is higher during systole (due to higher systolic blood pressure) than diastole. Aorta Pressure diameter (µm) 200 150 100 Time (s) Pressure + Flow diameter (µm) 200 150 100 Occlusions: 30 s 60 s 120 s Biomechanical events during and following occlusion Physical forces elicit: •Deformation •Stretch •Wall shear stress Resulting in: •Constriction •Dilation occlusion release Time olic meta b flow myo gen deformation ic stret ch Diameter / Flow Proposed scheme for sequential and relative contribution of deformation, stretch-, myogenic-, flow-dependent and metabolic vascular mechanisms in the development of reactive hyperemia. vasoactive agents in local regulation of blood flow PO2 ↓ PCO2 [H+] ↑ lactate Adenosine ATP EDHF Prostaglandins Endothelin NO (nitric-oxide) Etc. LOCAL MECHANISMS REGULATING TISSUE BLOOD FLOW Dilation [Ca 2+]i and Ca2+-sensitivity Transmural pressure Wall shear stress Constriction Vascular smooth muscle Endothelium (NO, PG, EDHF, ROM, ET) Blood flow (mass transport, e.g. oxygen) Parenchyma (adenosine…) PATHOPHYSIOLOGY DIABETES INCREASED PRESSURE-INDUCED CONSTRICTION C (-Endo) DM (-Endo) Diameter (%) 100 75 * * 50 ** ** * ** * * 0 20 40 60 80 100 120 140 PRESSURE (mmHg) REDUCED SHEAR STRESS-INDUCED DIALTION ∆ Diameter (µm) Control 30 DM * 20 10 0 0 5 10 15 20 Áramlás FLOW (µL/min) HYPERTENSION Effect of high pressure (hypertension) HYPERHOMOCYSTEINAEMIA Homocystein metabolism Protein Remethylation Transmethylation Methionine R S-Ado-Met MS RCH3 THF S-Ado-Hcy Homocysteine CBS cystathionine-β-synthase Transsulfuration B6 Cystathionine B6 Cysteine B12 MethylTHF Folsav Methylenetetrahydrofolate MTHF reductase Homocysteine Nem proteint alkotó aminósav methionin anyagcsere reactív thiol (-SH) csoport plazmaszint: 5-12 µmol/L IN HHCY-ATHEROSCLEROSIS CONTROL Kontroll HHC DIAMETER ∆ Átmérõ (µm) 40 30 20 10 0 -10 -20 -30 -40 0 5 10 15 20 Áramlás FLOW (µL/min) 25 30 HHCY PROMOTES ATHEROSCLEROSIS HHcy Shear stress endothelium eNOS Xanthineoxidase oxypurinol .O2 NO SOD L-NAME AA COX Indo PGH2 OONOPGI2 TxA2 PLATELET AGGREGATION, THROMBOSIS dilation constriction Smooth muscle HYPERTROPHY If NO and superoxide are produced peroxynitrite is formed: The biological activity of NO is decreased _ . O2 NO ONOO _ H+ _ . OH antioxidants Role of the endothelium in regulation of microcirculation HEALTH: Diameter (tone) Permeability Hemostasis NO DISEASE: stimulus PGI2 EDHF endothelium smooth muscle Proliferation Remodeling Inflammation TXA2 ET •O2- In pathological conditions vascular production of: Dilators are reduced (NO, PGI2) Constrictors are increased (TXA2, endothelin) Role of reactive oxygen species Thank You The End