Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
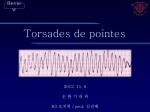
Torsades de pointes (long QT Syndrome) PHCP 403 Samirah Abdu-Aguye INTRODUCTION • Torsade de pointes is an uncommon and distinctive form of polymorphic ventricular tachycardia (VT) characterized by a gradual change in the amplitude and twisting of the QRS complexes around the isoelectric line • It is usually associated with a prolonged QT interval, which may be congenital or acquired. • It is one of the most common types of arrhythmias caused by drug interactions INTRO CONT’D • Torsade usually terminates spontaneously but frequently recurs and may degenerate into ventricular fibrillation. EPIDEMIOLOGY • The prevalence of torsade is unknown. Torsade is a life-threatening arrhythmia and may present as sudden cardiac death in patients with structurally normal hearts • Torsade is 2-3 times more common in women than in men. Women have longer QT intervals, and have more QT prolongation secondary to drug therapy. CLINICAL PRESENTATION • Patients with torsade usually present with recurrent episodes of palpitations, dizziness, and syncope; however, sudden cardiac death can occur with the first episode. • Nausea, cold sweats, shortness of breath, and chest pain also may occur but are nonspecific and can be produced by any form of tachyarrhythmia. RISK FACTORS Risk factors for torsade include the following: • Congenital long QT syndrome • Female gender • Several medications and electrolyte disorders such as hyperkalemia and hypomagnesemia) • Bradycardia • Baseline electrocardiographic abnormalities • Renal or liver failure/disease Acquired long QT syndromes Drugs in a number of drug classes have been associated with torsade. Antiarrhythmic drugs associated with torsade include the following: • Class IA - Quinidine, disopyramide, procainamide • Class III - Sotalol, amiodarone (rare), ibutilide, dofetilide, almokalant • Anti-infectives - Erythromycin, Ciprofloxacin, clarithromycin, azithromycin, levofloxacin, Moxifloxacin, gatifloxacin, Pentamidine, Chloroquine Fluconazole, Voriconazole, Amantadine • Antipsychotics - Haloperidol, Chlorpromazine, Ziprasidone, Amisulpride • Tricyclic antidepressants, Lithium, Moclobemide and Citalopram/Escitalopram • Antihistamines (histamine1-receptor antagonists) Terfenadine, astemizole, diphenhydramine, loratidine • Cholinergic antagonists - Cisapride, organophosphates (pesticides) • Citrate (massive blood transfusions) • Other drugs: Ondansetron, Dolasetron, Methadone, • Cocaine Treatment • Treatment can be divided into short-term and long-term management • In an otherwise stable patient, DC cardioversion is kept as a last resort because torsade is paroxysmal in nature and is characterized by its frequent recurrences • Any offending agent should be withdrawn. Predisposing conditions such as hypokalemia, hypomagnesemia, and bradycardia should be identified and corrected. Treatment Cont’d • Magnesium is the drug of choice for torsades. • Magnesium can be given at 1-2 g IV initially in 3060 seconds, which then can be repeated in 5-15 minutes. • Magnesium is effective even in patients with normal magnesium levels. Because of the danger of hypermagnesemia, the patient requires close monitoring. other drugs that can be used include mexiletine and isoproterenol • JD is a 60-year-old woman. She reports being in her usual state of relatively good health until she developed a “cold” approximately 4 days before admission. • She went to a community pharmacy complaining of her upper respiratory tract symptoms, and the pharmacist gave her for erythromycin 500 mg QID (for 10 days). She took the first dose on the morning of admission. She started feeling worse approximately 1 hour after taking the second dose of erythromycin. • She reported feeling lightheaded and short of breath. She experienced palpitations as well and eventually passed out for a few minutes, and was rushed to the hospital by her daughter. While being evaluated in the ED, she had another syncopal episode. An ECG showed Torsades de pointes. PMH Current Medications CAD Carvedilol 3.125 mg PO bid Chronic Renal disease Pravastatin PO 40mg OD Heart failure (EF 30%) Paroxysmal atrial fibrillation Furosemide 40 mg PO bid Warfarin 4 mg PO daily as directed Amiodarone 200 mg PO bid Candesartan 8 mg PO daily Erythromycin 500 mg PO QID, started day of admission Serum electrolytes • Na 140 mmol/L (135-145) • K 2.8 mmol/L(3.5-5) • Mg 1.2 mEq/L(1.5-2) Questions • What risk factors predisposed the patient to drug-induced arrhythmia? • List the specific medication(s) you believe caused the arrhythmia • How should this patient be managed? • What monitoring parameter should be used to assess efficacy and toxicity of treatment • List3 of the most common drug classes (with an example from each) associated with TdP. References • Isbister G. Risk assessment of drug-induced QT prolongation. Australian Prescriber [Internet]. 2015 [cited 20 February 2015];(Volume 38, Issue 1):20-24. Available from: http://www.australianprescriber.com/magazin e/38/1/issue/207.pdf • Dave J, Bessette M, Setnik G, Gaeta T, Lakhia R. Torsade de Pointes [Internet]. Emedicine.medscape.com. 2015 [cited 20 February 2015]. Available from: http://emedicine.medscape.com/article/1950 863-overview#a30