Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Schmerber v. California wikipedia , lookup
Blood transfusion wikipedia , lookup
Jehovah's Witnesses and blood transfusions wikipedia , lookup
Blood donation wikipedia , lookup
Autotransfusion wikipedia , lookup
Deep vein thrombosis wikipedia , lookup
Hemorheology wikipedia , lookup
Men who have sex with men blood donor controversy wikipedia , lookup
Hemolytic-uremic syndrome wikipedia , lookup
Von Willebrand disease wikipedia , lookup
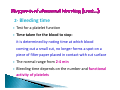
Blood coagulation Dr. Abir Alghanouchi Biochemistry department Sciences college Arrest of bleeding Events preventing excessive blood loss ◦ Vascular spasm: Vasoconstriction of damaged blood vessels ◦ Platelet plug formation ◦ Coagulation or blood clotting *DAMAGE TO BLOOD VESSEL leads to: 1. Vascular Constriction: Immediate constriction of blood vessel Vessel walls pressed together – become “sticky”/adherent to each other Minimize blood loss 2. Platelet Plug formation: PLATELETS attach to exposed collagen with the presence of von Willebrand factor (vWF) and Glycoprotein IbIX Aggregation of platelets causes release of chemical mediators (ADP, Thromboxane A2) ADP attracts more platelets Thromboxane A2 (powerful vasoconstrictor) * promotes aggregation & more ADP Leads to formation of platelet plug! 3- Blood Coagulation (clot formation): Final Step in Hemostasis: Transformation of blood from liquid to solid Clot reinforces the plug Multiple cascade steps in clot formation Process requires plasma proteins, PLs and calcium. Thrombin Soluble fibrinogen Insoluble fibrin Stages ◦ Activation of prothrombinase ◦ Conversion of prothrombin to thrombin ◦ Conversion of fibrinogen to fibrin Pathways ◦ Extrinsic ◦ Intrinsic Initially independent, then they converge on common pathway leading to the formation of a fibrin clot ! PRIMARY AGGREGATION Platelet Aggregation Clotting Hemostatic clot Fibrin SECONDARY COAGULATION 0 min Thrombin 5 min 10 min A cascade is a mechanism in which enzymes activate other enzymes sequentially usually leading to an amplification of an initial signal. Each of these pathways leads to the conversion of factor X (inactive) to factor Xa (active) The intrinsic and extrinsic coagulation pathways are a series of reactions involve coagulation factors known as 1. Enzyme precursors (zymogens) 2. Non-enzymatic (cofactors) 3. Calcium (Ca ++) 4. Phospholipids (PL). All coagulation factors normally are present in the plasma, with PL being provided by platelets. Zymogens: ◦ Factors II, VII, IX, X, XI, XII, and prekallikrein ◦ NO biologic activity until converted by enzymes to active enzymes called serine proteases Cofactors ◦ Factors V, VIII, tissue factor, and HMWK Extrinsic—Release of biochemicals from broken blood vessels/damaged tissue. Intrinsic—No tissue damage, blood contacts damaged endothelial layer of blood vessel walls. Intrinsic clotting—all factors are found in circulating blood. Extrinsic clotting—Factor III (tissue thromboplastin) is found outside of blood. Activated in vivo by endothelial injury, in vitro by glass or other contact A foreign surface such as collagen activates factor XII (Hageman factor). Acting as catalysts are high MW Kininogen (HMWK) and kallikrein in the contact phase. XI, XII, HMWK, PK The contact group is adsorbed by contact with a negatively charged surface such as collagen or the subendothelium in vivo. Not Vitamin K dependent Calcium is involved in three steps: the activation of FIX, X and prothrombin. Cofactor VIII interacts in the activation of factor X and cofactor V reacts with prothrombin. The platelet phospholipid surface acts as template in the activation of FX and prothrombin. Is initiated by the release of tissue thromboplastin (Factor III) which is exposed to the blood when there is damage to the blood vessel. Factor VII which is a circulation coagulation factor, forms a complex with tissue thromboplastin and calcium. This complex rapidly converts Factor X to the enzyme form Factor Xa. Factor Xa catalyzes the prothrombin (Factor II) to thrombin (Factor IIa) reaction which is needed to convert fibrinogen (Factor I) to fibrin. XIIIa and Ca++ stabilize fibrin clot Formation of blood clot causes more clotting to occur—positive feedback. Prothrombin is soluble single chain glycoprotein (72kDa) synthesized in liver Thrombin is produced by the enzymatic cleavage of two sites on prothrombin by activated Factor X (Xa) and generate active 2 chain thrombin molecule which is then released from platelet surface The A and B chains of thrombin are held together by a dissulfide bond S 1 A 2 Xa Fragment 2 -1 S S B Xa Prethrombin Prothrombin (72kDa) 1 + 2 Fragment 2 -1 A S B Active thrombin (34 kDa) Converts fibrinogen to fibrin Activation of prothrombin into thrombin (cont…) The activation of prothrombin occurs on the surface of activated platelets and requires assembly of prothrombinase complex consisting of platelet, anionic PLs, Ca2+, factor Xa and prothrombin This complex is termed factor Va which is activated by traces of thrombin Factor Va is subsequently inactivated by further action of thrombin to limit activation of prothrombin to thrombin Factor Xa Thrombin in Hemostasis Conversion of fibrinogen to fibrin 340kDa (factor I) is soluble plasma glycoprotein that consists of 3 non identical pairs of polypeptides chains (Aα, Bβ, γ)2 covalently linked by disulfide bonds The A and B portions of the Aα and Bβ chains, termed Fibrinopeptide A (FPA) and Fibrinopeptide B (FPB) Thrombin Release of FBs by thrombin generate fibrin monomer (weak) Aggregate spontaneously forming insoluble fibrin polymer (fibrin clot) (hard, insoluble) Antithrombin III ◦ Most important since it can also inhibit the activities of factors IXa, Xa, XIa and XIIa ◦ Binds to activated factors rendering them inactive ◦ The action of AT-III is enhanced and accelerated by the presence of Heparin (either naturally released from basophils or given therapeutically as an anticoagulant) Protein C ◦ Produced by liver; Vitamin K dependent ◦ Inhibits (cleaves) the cofactors VIIIa and Va ◦ Significantly decreases the rate of clot formation ◦ Needs to be activated (by Thrombin (IIa)) ◦ Enhancement of Protein C anticoagulant functions is achieved by Protein S. Protein S ◦ Produced by liver ◦ Vitamin K dependent ◦ Acts as a cofactor to Protein C to enhance its ability to degrade factors V and VIII Heparin ◦ It is a negatively charged polysaccharide found in mast cells near the walls of blood vessels and on the surfaces of endothelial cells ◦ Heparin acts as an anticoagulant by increasing the rate of formation of irreversible complexes between antithrombin III and the serine protease clotting factors Alpha 2-macroglobulins ◦ Contributes most of the remaining (25%) of antithrombin activity in plasma Alpha 1-antitrypsin ◦ Acts as a minor inhibitor under physiological conditions, which normally inhibits elastase ◦ Alpha 1-Antitrypsin activity normally increases markedly after injury to counteract excess elastase arising from stimulated neutrophils Vitamin K antagonists 1. Coumarin drug: ◦ They are anticoagulant in vivo ◦ They inhibit carboxylation of Glu residues in prothrombine and factors VII, IX, X Vitamin K antagonists 2. Dicumarol ◦ Is naturally occurred (plant origin) ◦ Used only in vivo as anticoagulant to prevent thrombosis in patients with a tendency to form blood clot ◦ Slow onset of action 2-3 days but long duration 4-6 days Heparin ◦ Animal origin (most cells) ◦ Acts both in vivo and in vitro ◦ Rapid onset few minutes Removal of Ca2+ by citrate oxalate (in vitro) Defibrination of blood ◦ Break down of fibrin threads once formed by continuous shaking or by glass rod Platelets (thrombocytes) have several functions in blood clotting: Form platelet plug at the site of injury Sites of activation of some clotting factors (II, X) Provide the surface on which certain clotting factors bind (Va, Xa, II, Ca2+) Sources of some clotting factors (XIII, PL) If platelets are not lysed, blood does not clot Individuals with thrombocytopenia (low platelets), bleeding for a long time Platelets deficiency can be due to many agents (drugs, some infections, ionizing radiation) Clot is slowly dissolved by the “fibrin splitting” called Plasmin Plasmin gets trapped in clot and slowly dissolves it by breaking down the fibrin meshwork at various places, leading to the production of circulating fragments that are cleaved by other proteases or by the kidney and liver Plasminogen is the inactive pre-cursor that is activated by activators in plasma: 1. Tissue plasminogen activator (t-PA) 2. Urokinase (to lesser extend) Is produced as a precursor “prourokinase’’ by epithelial cells Its main action is probably in the degradation of extracellular matrix Inactive t-PA is released from vascular endothelial cells following injury It binds to fibrin and is consequently activated Active t-PA converts plasminogen into plasmin Dissolves the clot Inherited bleeding disorders ◦ Hemophilia A and B ◦ Von Willebrand disease ◦ Other factor deficiencies Acquired bleeding disorders ◦ Liver disease ◦ Vitamin K deficiency 1- Hemophilia A and B Are the best-known coagulation factor disorders Hemophilia A Coagulation factor deficiency Inheritance Incidence Hemophilia B Factor VIII Factor IX X-linked recessive X-linked recessive 1/10,000 males 1/50,000 males 2- von Willebrand Disease It is the most common hereditary bleeding disorder and is characterized as being inherited autosomal recessive or dominant In this disease there is a defect in von Willebrand factor (vWF) which: 1. 2. acts as a carrier for factor VIII mediates the binding of glycoprotein Ib (GPIb) to collagen 2- von Willebrand Disease This binding helps the activation of platelets and formation of primary hemostasis vWD is characterized by excessive bleeding in infants because platelets fail to form hemostatic plug Source of vitamin K Green vegetables Synthesized by intestinal flora Required for synthesis Factors II, VII, IX ,X contribute to bleeding disorders Causes of deficiency Malnutrition Biliary obstruction Malabsorption Antibiotic therapy 1. Formation of carboxyglutamate Vitamin K is essential for the functioning of several proteins involved in blood clotting (II, VII, IX and X) These proteins contain a unique modified glutamate residue, called carboxyglutamate (Gla). These proteins are synthesized as inactive precursors that are activated by the vitamin K-dependent carboxylase which converts glutamate in these proteins to carboxyglutamate forming mature clotting factors. 1. Formation of carboxyglutamate (cont…) (mature) Dicumarol, Warfarin (Gla residue) 2. Interaction of prothombin with platelets The Gla residue of prothrombin is a natural high affinity binder (chelator) of positively calcium ions, hence the designation of calcium as a co-factor (factor IV) in the schematic. The prothrombin-calcium complex is then able to bind to PLs essential for blood clotting on the surface of platelets. Extrinsic system (tissue damage) Intrinsic system (surface contact) XIIa XII Tissue factor XIa XI IX VIIa IXa VIII VII VIIIa X Xa V Va II Fibrinogen Vitamin K dependant factors IIa (Thrombin) Fibrin A number of parameters are used for diagnosis of clotting disorders including: 1. Coagulation time (whole blood clotting time) 2. Bleeding time 3. Prothrombin time (PT) 4. Prothrombin consumption test 5. Activated partial thromboplastin (APTT) 6. Thrombin clotting time (TT) 1- Coagulation time Test for intrinsic system Simple test but takes time and rarely done now Method: Venous blood is taken and placed on glass test tube at 37°C and it observed at time intervals until clotting occurs Normal blood takes 5-10min to clot Longer periods Coagulation defects 2- Bleeding time Test for a platelet function Time taken for the blood to stop: it is determined by noting time at which blood coming out a small cut, no longer forms a spot on a piece of filter paper placed in contact with cut surface The normal range from 2-4 min Bleeding time depends on the number and functional activity of platelets 3- Prothrombin time (PT) Test for extrinsic system It involves tissue factor The level of prothrombin in blood is measured indirectly by measuring PT 3- Prothrombin time (PT) (cond…) Method: An excess of tissue factor and Ca2+ ions are added to diluted plasma containing citrate (anticoagulant) and then the time taken for the mixture to clot is measured High PT low level thrombin Results from liver disease due to deficiency of prothrombin, fibrinogen, V, VII and X factors 4- Prothrombin consumption test This test is used for detection of minor coagulation defects Method: Ca2+ is added to both plasma and serum samples At given time intervals, the mixture is subsampled into tubes containing fibrinogen and the time taken for fibrinogen to clot is recorded The normally plasma will clot fibrinogen very rapidly (12-20s) because it contains prothrombin but serum takes 2-3 min or more because it contains normally little prothrombin (it is removed) 4- Prothrombin consumption test plasma time x100 Prothrombin consumption time (%) = Serum time It is less than 20% Higher percentage means inefficient hemostasis so serum contains more thrombin e.g. 0.5/2.5*100=20% 0.5/1*100=50%>20% Normal Disorder 5- Activated partial thromboplastin (APTT) This test is used for intrinsic system Method: A mixture of koalin (provide a maximal stimulus for factor XII) and PL (acts as platelet substitute) is added to citrate plasma following by Ca2+ The time taken for mixture to clot is measured Prolonged clotting time is almost always due to deficiency of factors VIII and IX Normal APTT: 20-25 to 32-39 s; Critical Values: >100-150 seconds 6- Thrombin clotting time (TT) TT is a coagulation assay which is usually performed in order to detect for the therapeutic level of the anticoagulant Heparin It is also sensitive in detecting the presence of a fibrinogen abnormality 6- Thrombin clotting time (TT) (cont…) Method: After liberating the plasma from the whole blood by centrifugation, bovine thrombin is added to the sample of plasma The clot is formed and is detected optically or mechanically by a coagulation instrument The time between the addition of the thrombin and the clot formation is recorded as the thrombin clotting time (generally <21s) APTT Prolonged, PT Normal: Deficiencies of factor VIII, IX, XI, and/or XII (intrinsic pathway) PT Prolonged, APTT Normal: Deficiency of factor VII (extrinsic pathway), mild-to-moderate deficiencies of factor II, V, X, and/or fibrinogen (common pathway) Both PT and APTT Prolonged: Deficiencies of factor II, V, X, and/or fibrinogen (common pathway), Multiple factor deficiencies