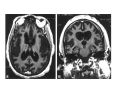
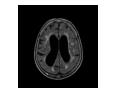
Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
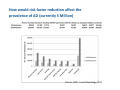
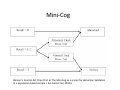
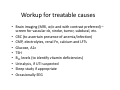
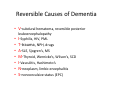
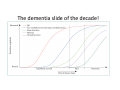
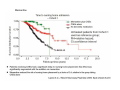
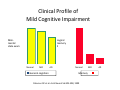
Dementia – Learning Objectives • What is Dementia? • Differentiate dementia types, e.g. AD, VaD, DLB, FTD • Clinical evaluation of a dementia patient • Rapidly progressive dementias • Treatment of dementia • Current research directions in dementia What is Dementia • A clinical diagnosis – A decline in cognitive ability – To diagnose dementia, there also needs to be evidence of impaired of functioning, e.g. performing activities of daily living, occupational, or social functioning – A measured decline in cognitive ability, from baseline, or that is significantly lower than expected, without functional impairment defines “MCI”, that is often a prodrome to dementia What is Dementia • A clinical diagnosis • Many pathologies may cause it: – Alzheimers – Vascular disease – Lewy Body – Frontotemporal degeneration – Others (CBD, PSP, MSA, Prion, rare genetic causes) • Dementia “mimics” Clinical case • 72yo RHD male, with 14 years of education • CC: “I’m fine, my family made me come here” • He reports he has no problems with memory or ADLs, and no problems driving. • PMH: HTN, HLD, “borderline” diabetes, CABG 2011 • Meds: “One for my blood pressure, and a white one”, NKDA Clinical case ‐ continued • SH ‐ Retired accountant, lives alone, divorced, 2 children live in a neighboring city and work full time. He drinks a beer “every now and then” • FH – father had dementia in his late 70’s • ROS: Occ low back pain, slow stream when urinating. Dementia Risk Factors • • • • • • • Age Female sex ApolipoproteinE‐ɛ4 Prior head injury Low education Family history Stroke • • • • • • Sedentary lifestyle Obesity Hypertension Hyperlipidemia Diabetes Smoking Non modifiable risk factors • Age: ~2% of 65‐year‐olds will develop dementia every year, less than 5% prevalence at this age. Annual risk in 70’s is about 5%, and prevalence increases to nearly 50% by early to mid 80’s • Family history raises the annual risk by about 30%, so about 2.6% per year at 65, to 6.5% per year in 70’s. So the absolute increase in risk is still relatively small. Non‐modifiable risk … • ApolipoproteinE‐ɛ4 (APOE4) gene is associated with greater risk for dementia. It was initially described as a lipid transport protein and major ligand LDL receptors with a role in cholesterol metabolism and cardiovascular disease. • For each copy of ɛ4, avg. age of onset is 8yrs sooner • One copy of the ɛ4 variant triples risk, and 2 copies (rare) increases risk more than 10‐fold, … but … Mahley RW. Apolipoprotein E: from cardiovascular disease to neurodegenerative disorders. Journal of molecular. 2016;94(7):739‐746. Non modifiable risk factors • Relative risks overemphasize small differences – APOE4 does not mean you will definitely develop dementia ! • APOE4 is present in 25% of people who are cognitively normal in their 70s, conversely 35% of those with Alzheimer’s don’t have any copies of the e4 allele. • Testing for APOE4 in a clinical setting will will not tell you what you want to know – that is: if you have, or if will you get Alzheimer's disease or not. How would risk factor reduction affect the prevalence of AD (currently 5 Million) Barnes, Yaffe ‐ Lancet Neurology, 2011 Questions to ask • Any recent illnesses, recurrent UTIs? • Any new prescription or over‐the‐counter medications? benzodiazepines, opiates, anticholinergic drugs for urinary incontinence, sleep aids? (Beers List) • Alcohol use, or illicit drugs? • Any environmental factors? • Has the patient had any head injuries recently, or history of significant head injury? • History of stroke, epilepsy, sleep apnea? Modified from: Galvin, J Am Board Fam Med May‐June 2012 vol. 25 no. 3 367‐382 Clinical case ‐ exam • Basic neurological exam is unremarkable, except for his blood pressure 154/90, positive Palmomental reflex on both sides; he is unable to perform tandem gait, but is otherwise steady when walking. • You reassure him, recommend closer monitoring of his blood pressure and low salt diet, order health screening labs including lipid panel and PSA. Uh‐Oh! • As you send him out to checkout, his ex‐wife, who was waiting in the waiting room grabs you in the hallway, and panicking, tells you he has had three car accidents, did not pay their taxes this year, resulting in fines, is repeating conversations and misplacing items. • What went wrong with this visit? Reliable history is important • Anosognosia – Inability to recognize illness (or impairment) • Many patients with dementia are not aware of the impact on ADLs, even though they may report awareness of memory loss • History from a reliable witness, who knows the patient well is essential Cognitive screening • MMSE – Well known, but can miss subtle of non‐ Alzheimer type dementia • MoCA – Sensitive, readily available, but takes longer to administer • Kokmen – Similar sensitivity to MoCA, requires no paper form • Short Blessed Test – Fast, tests memory and executive function, limited language, no visuospatial • MiniCog – Very fast and easy. Not as sensitive or specific as other tests, but appropriate for screening in primary care setting. Mini‐Cog Borson S, Scanlan JM, Chen PJ et al. The Mini‐Cog as a screen for dementia: Validation in a population‐based sample. J Am Geriatr Soc 2003;5 What else to look for? • Normal age‐associated memory changes? – We spend a lot of time educating population that significant memory loss with age is not “normal”, but mild changes with age are still expected. • Depression – Especially if new onset of depression later in life • Vision problem • Hearing problem Workup for treatable causes • Brain imaging (MRI, w/o and with contrast preferred) – screen for vascular dz, stroke, tumor, subdural, etc. • CBC (to ascertain presence of anemia/infection) • CMP, electrolytes, renal Fn, calcium and LFTs • Glucose, A1c • TSH • B12 levels (to identify vitamin deficiencies) • Urinalysis, if UTI suspected • Sleep study if appropriate • Occasionally EEG Reversible Causes of Dementia • V‐subdural hematoma, reversible posterior leukoencephalopathy • I‐Syphilis, HIV, PML • • • • • • T‐trauma, NPH, drugs A‐SLE, Sjogren’s, MS M‐Thyroid, Wernicke’s, Wilson’s, SCD I‐Vasculitis, Hashimoto’s N‐neoplasm, limbic encephalitis S‐nonconvulsive status (EPC) Remember the caregiver! • Identify the primary caregiver – It is rare that there is not an identifiable caregiver, impaired patients who are functioning in the community usually have someone helping them, and it may be surprising who that turns out to be • Assess adequacy of family and other support system Physician Quality Reporting System (PQRS) 2013 Dementia measures set Diagnosis and Staging of Dementia: [Mild/Moderate/Severe] Cognitive Assessment: [e.g. MoCA or MMSE] Functional Status Assessment: [FAQ – clinical screen, IADLs] Neuropsychiatric Symptom Assessment [e.g. NPI domains screen] Management of neuropsychiatric symptoms Screening for Depression Safety Driving Caregiver education and counseling Types of Dementia • Alzheimer’s disease • Lewy Body Dementia • Vascular (post‐stroke, Binswanger’s…) • • • • • • • • • • • Pseudodementia (depression) Post‐traumatic/Dementia Pugilistica Toxic/metabolic Lewy Body Dementia Fronto‐temporal dementia Prion diseases (Creutzfeldt‐Jakob disease) Steroid‐responsive autoimmune encephalopathy associated with thyroid dysfunction (Hashimoto’s encephalopathy) Primary progressive aphasia Semantic dementia Cortico‐basal degeneration Other rare causes From: Ecology of the Aging Human Brain Arch Neurol. 2011;68(8):1049-1056. doi:10.1001/archneurol.2011.157 Figure 1. Brain autopsy results from 336 cognitively normal individuals expressed as summary neuropathology scores (range, 0-9) ranked from lowest to highest. Each stacked bar shows an individual's burden of Alzheimer disease (AD) (blue), Lewy body disease (LBD) (green), and microvascular brain injury (μVBI) (red). A, One hundred sixteen Adult Changes in Thought study (ACT) participants. B, One hundred six Nun Study (NS) participants. C, Fifty-nine Honolulu-Asia Aging Study (HAAS) participants. D, Fifty-five Oregon Brain Aging Study (OBAS) participants. Date of download: 7/21/2016 Copyright © 2016 American Medical Association. All rights reserved. Dementia is a “mixed bag” of disorders Diagnosis of Alzheimer’s dementia A. B. C. Insidious onset. Symptoms have a gradual onset over months to years, not sudden over hours or days; Clear‐cut history of worsening of cognition by report or observation; and The initial and most prominent cognitive deficits are evident on history and examination in one of the following categories A. Amnestic presentation: It is the most common syndromic presentation of AD dementia. The deficits should include impairment in learning and recall of recently learned information. There should also be evidence of cognitive dysfunction in at least one other cognitive domain. B. Nonamnestic presentations: – Language presentation: The most prominent deficits are in word‐finding, but deficits in other cognitive domains should be present. – Visuospatial presentation: The most prominent deficits are in spatial cognition, including object agnosia, impaired face recognition, simultanagnosia, and alexia. Deficits in other cognitive domains should be present. – Executive dysfunction: The most prominent deficits are impaired reasoning, judgment, and problem solving. Deficits in other cognitive domains should be present. The diagnosis of dementia due to Alzheimer’s disease: Recommendations from the National Institute on Aging‐Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer's disease. McKhann, Guy M. et al. Alzheimer's & Dementia: The Journal of the Alzheimer's Association , Volume 7 , Issue 3 , 263 ‐ 269 Alzheimer’s disease pathology History: Biology 1906‐ first description of Auguste D. age 51 1976‐ cholinergic deficit in AD discovered 1984‐ b‐amyloid discovered as key component of AD plaques 1986‐ tau protein discovered as key component of NFT • • • • • • AD Facts Only 5% of cases are familial (APP, PS1, PS2) ApoE4 allele is risk factor Cholinergic deficit B‐amyloid plaques Tau & neurofibrillary degeneration No cure amyloid is a key player in AD amyloid is a key player in AD 1) APP is a membrane‐bound glycoprotein that may serve as a growth factor in injury and repair 2) APP is normally cleaved by ‐ secretase and ‐ secretase, but in AD, ‐secretase is active 3) ‐amyloid is toxic to cells and accumulates in brain tissue as amyloid plaques, a hallmark of the disease Neurofibrillary tangles (NFT) & paired helical filaments (PHF) The role of the microtubule‐ associated protein tau in AD Structural MRI can monitor progression of disease from normal to MCI to Dementia Alzheimer’s Dementia • Under recognized and under diagnosed ‐ Only 38% of AD patients are diagnosed in the primary care setting • Families & friends often do not recognize the early warning signs of dementia • Treatment usually sought only after significant decline Knopman et al., (2000) J Am Ger Soc 48:300‐4 The dementia slide of the decade! Increasing severity of disease Amyloid plaques NFTs Cholinergic pathways Increasing severity of disease Memantine Clinical Profile of Mild Cognitive Impairment 30 16 14 25 12 20 Mini‐ mental 15 state exam Logical memory II 10 8 6 10 4 5 2 0 0 Normal MCI General cognition AD Normal Memory Petersen RC et al: Arch Neurol 56:303‐308, 1999 MCI AD Increased risk of AD in MCI MCI AD 12%/yr Control AD 1‐2%/yr 100 100 90 90 80 80 70 70 60 60 50 50 Initial exam 12 24 36 Months 48 Initial exam Petersen RC et al: Arch Neurol 56:303‐308, 1999 12 24 36 Months 48 Vascular dementia (VaD) • Heterogeneous phenotype • Cortical deficits: – Lg vessel infarcts • Subcortical deficits: – – – – – Lg vessel infarcts Sm vessel infarcts Lacunar infarcts White matter disease Microvascular disease • Mixed with other degenerative dementia Heterogeneity of VaD Clinically silent infarcts on imaging No clinical strokes & below threshold imaging Strategic single infarcts Multiple lacunar infarcts Multiple large infarcts White matter infarcts Alzheimer pathology Dementia following stroke Vascular Dementia No infarcts Knopman DS Continuum 2004;10(1):113‐134 Syndrome: abrupt onset of confusion, left neglect, disorientation, and “memory” Syndrome: abrupt onset of confusion, confabulation, and autobiographical memory impairment Syndrome: abrupt onset of confusion, confabulation, and autobiographical memory impairment Those were easy… What about these? Syndrome: insidious onset, slowly progressive, attention & concentration impairment Syndrome: insidious onset, slowly progressive, memory, attention, & concentration impairment The continuum of dementia “Pure AD” AD with CAA AD with vascular involvement AD with vascular lesions AD with CVD VaD with AD changes VaD with small vessel disease “Pure VaD” Roman GC Acta Neurol Scand 2002;106(s178):6‐9 DLB Requires the presence of dementia, the “D” in DLB ≥2 core features are essential for a diagnosis of probable DLB, ≥1 for possible DLB: • Fluctuating cognition with pronounced variations in attention and alertness • Recurrent visual hallucinations that are typically well formed and detailed • Spontaneous motor features of parkinsonism Suggestive features: (If one or more of these is present with one or more core features, a diagnosis of probable DLB can be made. In the absence of any core features, ≥1 suggestive features is sufficient for possible DLB. • REM sleep behavior disorder • Severe neuroleptic sensitivity • Low dopamine transporter uptake in basal ganglia DLB supportive features • • • • • • • • • • • • Repeated falls Syncope Severe autonomic dysfunction Transient loss of consciousness Neuroleptic sensitivity Hallucinations in other modalities Systematized delusions Depression CT/MRI shows relative preservation of temporal lobe structures Occipital hypometabolism identified by PET/SPECT Abnormal (low uptake) MIBG myocardial scintigraphy Prominent EEG slowing with temporal lobe transient sharp waves ‐synuclein 40x H&E 40x DLB pathology Brainstem Thalamus & hippocampus Amygdala & basal ganglia Standard Brain Imaging Studies are Largely Unrevealing Ishii, K. "PET approaches for diagnosis of dementia." American Journal of Neuroradiology 35.11 (2014): 2030‐2038. Treatment of DLB • DLB responds better to cholinesterase inhibitors than patients with Alzheimer's disease on both cognitive and behavioral measures • antipsychotics should be used infrequently and with caution 2o extrapyramidal side effects • 90% (10/11) of DLB patients had partial to complete resolution of psychosis using quetiapine Fernandez et al. Journal of Clinical Psychiatry. 63(6):513‐5, 2002 Jun. • selective serotonin reuptake inhibitors may be of benefit Swanberg MM. Cummings JL. Drug Safety. 25(7):511-23, 2002. DLB is part of the Parkinson’sAlzheimer spectrum Galvin: Arch Neurol, Volume 58(2).February 2001.186-190 FTD FTD • Behavioral variant – Behavioral (personality changes) prominent, loss of empathy, odd behavior, mood dysregulation, disinhibition or apathy – Judgement, planning, multi‐tasking, task switching are also impaired – Appetite changes, hyper or hypo‐sexuality • Semantic Dementia – Loose “meaning” of words may still produce speech that gradually becomes devoid of meaning but remains “fluent” – loose nouns>>verbs, left side temporal lobe predominant atrophy – Right side tends to produce prposagnosia, trouble recognizing emotions, poor non‐verbal communication • Progressive Non‐fluent Aphasia – Relative preservation of comprehension and “meaning”, but unable to produce speech, similar in many aspects to Broca’s apahsia, but gradually progressive. – Association with parkinsonism, CBD or PSP like syndrome (tauopathy) • FTD‐ALS – Often a behavioral variant. – Strong genetic association (C9ORF72 repeats, GRN, TRDBP, CHAMP2) Rapidly Progressive Dementia • • • • • • • • CJD (about 2/3 of degenerative cases) HIV Toxic/environmental Wernicke's Limbic Encephalitis Hashimoto’s Encephalopathy Venous Thrombosis MID Neurol Clin Pract. 2012 Sep; 2(3): 187–200. CJD • Variant Creutzfeldt‐Jakob disease (vCJD) is a rare and fatal human neurodegenerative condition, linked to the consumption of food contaminated with the prion agent. • 175 cases of vCJD were reported in the United Kingdom of Great Britain and Northern Ireland (United Kingdom), and 49 cases in other countries from October 1996 to March 2011. • Following the successful containment of the BSE epidemic in cattle, the number of cases of vCJD in the United Kingdom has declined since 2000. • Sporadic CJD, occurs in 1:1,000,000, and accounts for about 85% of CJD cases; • 5–15% inherited: Gerstmann‐Straussler‐Scheinker (GSS), Familial Fatal Insomnia • Iatrogenic CJD, which results from accidental transmission via contaminated surgical equipment or as a result of corneal or meningeal (dura mater) transplants or the administration of human‐derived pituitary growth hormones; < 5% of CJD cases. WHO Fact sheet N°180 Revised February 2012 Figure 2. Chronologic change of the striatal and cortical lesions. Y. Shiga et al. Neurology 2004;63:443-449 ©2004 by Lippincott Williams & Wilkins Syndrome: insidious onset, slowly progressive, isolated memory impairment Limbic Encephalitis • Subacute onset of progressive memory impairment … • headache, irritability, sleep disturbance, delusions, hallucinations, agitation, seizures and psychosis Anti‐Hu, Anti CRMP‐5 Lung SCC. Anti‐Ma2, germ‐cell tumours of the testis. Anti‐NMDAR, ovarian tumors, commonly teratomas. VGKC antibodies(including LG‐1), not usually paraneoplastic – NMDA antibodies can be triggered by teratoma, post HSV, or may be sporadic – – – – Other immune mediated … • Hashimoto’s encephalopathy, or “Steroid Responsive Encephalopathy associated with Autoimmune Thyroiditis” (SREAT) • MS • Vasculitis Other infectious: • HIV, Syphilis, Lyme, Whipples NPH • Abnormal gait: Earliest feature and most responsive to treatment; bradykinetic, broad‐ based, magnetic, and shuffling gait • Urinary incontinence: Urinary frequency, urgency, or frank incontinence • Dementia: Prominent memory loss and bradyphrenia; forgetfulness, decreased attention, inertia Numerous clinical trials in last two decades. Why no cure yet? Is it because we have the wrong drug? or because we haven’t treated early enough? Wrap up • • • • • • • • Dementia is a common clinical diagnosis with advancing age, with several , often overlapping causes. Ealry onset disease more often single disease and rarer. Many “proteinopathies” involved in neurodegeneration. AD is most common (AB42), also DLB (SNCA), Tau is a marker of secondary neurodegeneration, but may be primary in some dementia (PSP, CBD, some FTD, PTE) Vascular disease is inextricable from much of late life onset dementia Despite overlapping pathologies, the clinical syndrome, esp. the pattern of early symptoms, provides insight into primary underlying pathologic mechanisms, guides treatment, informs prognosis as well as guiding targets for clinical research. Clinical evaluation of a dementia patient must consider the whole person, their occ and educational background, environment, culture and caregivers. QoL and safety are paramount. Rapidly progressive dementias require careful investigation “VITAMINS” Symptomatic treatment is not futile – delaying a disease of late life, even a little, and treating neuropsychiatric symptoms have cumulative benefits on pt. and caregivers. Current research directions in dementia are focusing on prevention with lifestyle interventions as well as molecular targets such as proteinopathies in pre‐clinical disease, protein changes during disease such as tau, and neuroprotective agents, especially important for those already affected or when prevention fails.