Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
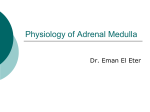
1885 Propranolol and Lidocaine Inhibit Neural Norepinephrine Release in Hearts With Increased Extracellular Potassium and Ischemia Xiao-Jun Du, PhD; Rudolph A. Riemersma, PhD; Keith A.A. Fox, MD; Anthony M. Dart, MRCP, PhD Downloaded from http://circ.ahajournals.org/ by guest on June 16, 2017 Background. Propranolol and lidocaine are effective antiarrhythmic drugs in myocardial ischemia and infarction. As sympathetic nerve activation and norepinephrine release in ischemic hearts are arrhythmogenic, we tested the possibility that both agents inhibit neural norepinephrine release following sympathetic activation in the ischemic environment. Methods and Results. The model used was an in situ perfused innervated rat heart. Norepinephrine release was induced by electrical stimulation of the left cervicothoracic stellate ganglion and analyzed using radioenzymatic assay or high-performance liquid chromatography. In normoxically perfused hearts, evoked norepinephrine release was not affected by either of the two agents at doses of 1 to 10 ,gmol/L when extracellular K' concentration was 4 mmol/L but dose-dependently reduced at 10 mmol/L K+ (D,L-propranolol: -53±4% at 1 ,umol/L and -64±6% at 10 gmol/L; lidocaine: -37±11% at 0.1 jzmol/L -67±5% at 1 ,umol/L, and -75±6% at 10 ,umol/L). At 10 mmol/L K', norepinephrine release was not affected by timolol or atenolol (both 10 ,umol/L but was equally inhibited by D- or L-propranolol at 10 ,umol/L (-56±5% and -53±9%o, respectively), indicating a P-blocking-independent mechanism. In hearts with metabolic acidosis (pH 6.85) at K' of 4 mmol/L, neural norepinephrine release was also reduced by propranolol at 10 pimol/L (-37%). Finally, in hearts perfused with 4 mmol/L K' and subjected to 6-minute periods of ischemia, neural norepinephrine release was similarly suppressed by D,Lpropranolol (-38±6% at 0.1 ,umol/L, -445% at 1 ,zmol/L, and -78±3% at 10 ,umol/L) or lidocaine (-39+7% at 0.1 umol/L, -58±9%o at 1 ,umol/L, and -91±3% at 10 ,umol/L). Conclusions. These data indicate that propranolol and lidocaine inhibit neural norepinephrine release via a Na+ channel-blocking mechanism that is synergistic with changes induced by ischemia, primarily raised extracellular K'. This mechanism may contribute to the anti-ischemic and antiarrhythmic properties of both agents in acute myocardial ischemia, which induces increased extracellular K' and sympathetic activation. (Circulation. 1993;88[part 11:1885-1892.) KEY WORDs * potassium * ischemia * nervous system * sodium * 3-adrenergic receptors membranes T he antiarrhythmic and anti-ischemic effects of propranolol in acute myocardial ischemia and infarction have been well established.1-4 In the setting of ischemia, sympathetic activation with norepinephrine (NE) release in the ischemic myocardium is considered of importance in mediating ventricular arrhythmias.5 The protective effects of 3-adrenergic antagonists are generally attributed to blockade of 8-adrenoceptors on myocytes. Whether the antiarrhythmic effect may be partly due to inhibition of neural norepinephrine release in the ischemic myocardium is unknown. Although it is well known that activation of presynaptic f3-adrenoceptors facilitates norepinephrine release, studies examining the effect of P-antagonists on norepinephrine release yield conflicting results.6 In addition, some P-antagonists, like propranolol, Received March 11, 1993; revision accepted June 22, 1993. From the Cardiovascular Research Unit (R.A.R., K.A.A.F.), Department of Medicine (RIE), University of Edinburgh, Edinburgh, UK; and Baker Medical Research Institute (X.-J.D., A.M.D.), Melbourne, Australia. Correspondence to Dr X.-J. Du, Baker Medical Research Institute, Prahran, Victoria 3181, Australia. possess a nonspecific membrane stabilizing activity, in- cluding the blockade of voltage-gated Na' channels.7 This activity, however, is generally considered of minor importance, as it requires concentrations far above those achieved clinically. Acute myocardial ischemia induces regional hyperkalemia and acidosis within minutes of interruption of coronary flow.8'9 Elevated extracellular K' concentration ([K+]o) is known to interfere with the conduction of the action potential in Purkinje fibers or myocytes9-13 and perhaps also in adrenergic nerves.14 Interestingly, studies in vitro have revealed a potentiation, by a raised [K']. or by acidosis, of inhibitory effects of lidocaine on Na' channels of myocardium.10-12,15,16 As depolarization of the neural plasmalemma by Na' influx via voltagegated Na' channels is necessary for action potential propagation and subsequent norepinephrine release,17 an inhibition of Na' channels of the neural membrane in ischemia may suppress norepinephrine release and hence the intensity of the subsequent adrenergic stimulation to the ischemic myocardium. This possibility, however, has never been tested. 1886 Circulation Vol 88, No 4, Part 1 October 1993 Using a perfused, innervated rat heart model,1819 we have therefore studied the effects of propranolol and lidocaine on neural norepinephrine release during simulated ischemia (ie, increased [K']. and acidosis) and stop-flow ischemia. We chose lidocaine as a reference agent for propranolol because it is a well-defined Na' channel blocker with effects known to be enhanced by increased [K']. or by acidosis'0-1215,16 and also because it is an effective agent for the acute treatment of ischemic arrhythmias.20 Methods Downloaded from http://circ.ahajournals.org/ by guest on June 16, 2017 Preparation Male Sprague-Dawley rats (280 to 350 g) were used for this study. Experiments were carried out using a perfused, innervated rat heart model previously described in detail.18"19 Rats were anesthetized with pentobarbital (60 mg/kg IP) and heparinized (200 U per rat IV). The chest was opened and a metal cannula inserted into the ascending aorta to start coronary perfusion in situ. The perfusate was a modified Krebs-Henseleit solution containing (in mmol/L) Na' 145, K' 4.0, Ca2 1.85, Mg2- 1.05, HCO3- 25, P043- 0.5, glucose 11, and EDTA 0.027. The buffer was continuously gassed with 95% 02-5% CO2 (pH 7.4) and warmed to 37°C. Perfusion flow rates were controlled by a peristaltic pump and set at 5 mL* g` * min' by the estimated heart weight. The left cervicothoracic stellate ganglion, with the cardiac nerves attached, was separated and mounted on a pair of bipolar electrodes for subsequent electrical stimulation using a model S88 or a model SD9 stimulator (Grass Instrument Co, Quincy, Mass).'9 The nerves were continuously superfused with warm and oxygenated buffer except when stimulated. Stimuli had a pulse width of 2 milliseconds, a current of 0.8 mA, and a frequency of 5 Hz. After ligation of bilateral pulmonary vessels and the superior vena cava, a catheter was inserted via the inferior vena cava into the right atrium for the collection of coronary venous effluent. The recovery of coronary effluent was between 85% and 100%. The left ventricle was cannulated via the apex, and the ventricular pressure was derived from a pressure transducer (Elcomatic, Glasgow, UK) or a microtip catheter pressure transducer (model SPR-249, Millar Instruments Inc, Houston, Tex) and was recorded on a TA2000 recorder (Gould Inc, Cleveland, Ohio) or a model 7 polygraph (Grass Instrument). Heart rate was measured from ventricular pressure traces. Alteration of K' levels in the perfusate was achieved by infusion, via a model 22 or a model 901A pump (Harvard Apparatus, South Natick, Mass), of KCl solution, and final K' concentrations achieved were ascertained by measuring K' levels in the perfusate and in the venous effluent collected in the absence of nerve stimulation using a model 501 Na/K analyzer (Instrumentation Laboratory, Milan, Italy). Global heart ischemia was induced by stopping of perfusion, and the myocardial temperature was kept at 37°C by covering hearts with a thermostatic chamber. Coronary effluent was collected during the first 2 minutes of the restoration of coronary flow to the preischemic level. Norepinephrine Assay Two norepinephrine analysis methods-radioenzymatic assay and high-performance liquid chromatography (HPLC) with electrochemical detection -were used in this study. Samples collected from one experiment were always assayed with the same method and, whenever possible, in a single assay run. In experiments carried out in Edinburgh, effluent samples were immediately cooled on ice and mixed with an equal volume of perchloric acid (final concentration, 0.3N) and stored at -40°C until assayed. Concentrations of norepinephrine were analyzed radioenzymatically in duplicate, and the average of the two measurements was used.2' The intra-assay coefficient of variation at 2 pmol/mL was 7%. For those experiments carried out in Melbourne, effluent samples were immediately frozen on dry ice and stored at -70°C until analyzed using an HPLC method. Norepinephrine was extracted using alumina adsorption, separated by HPLC, and quantified by electrochemical detection.22 The intra-assay coefficient of variation was 3%. Drugs Used Desipramine, atenolol, timolol, D,L-propranolol, D-propranolol, L-propranolol (all from Sigma Chemical Co, St Louis, Mo), butoxamine (provided by Dr A. Ungar, Department of Pharmacology, University of Edinburgh), and lidocaine chloride (Delta West Ltd, Bentley, Australia) were used. Protocols A 20-minute period of perfusion with normal perfusate was allowed to stabilize preparations before the experiment. All experiments were carried out in the presence of desipramine (final concentration of 0.1 ,umol/L) to inhibit neural norepinephrine reuptake. Sympathetic ganglion stimulation was performed at 5 Hz for periods of 30 or 60 seconds with 15-minute intervals between stimuli. The first stimulus (S,) served as a reference for each experiment. Drugs or KCl were infused into the heart at least 10 minutes before the subsequent stimulation. Coronary effluent was collected for a period of 2 minutes immediately before or during and after nerve stimulation. In two groups of hearts (n=8 each) perfused with either 4 or 10 mmol/L K+, the reproducibility of norepinephrine release in response to five episodes of nerve stimuli (30 seconds) was examined. Propranolol and norepinephrine release. The effect of propranolol and other P8-antagonists on norepinephrine release was examined in seven separate groups of hearts perfused with various perfusate K' concentrations (Table 1). Hearts in group 1 were initially perfused with 4 mmol/L K'. After a control nerve stimulus (S,, 30 seconds), D,L-propranolol was infused into the heart at 1 ,umol/L throughout the subsequent experiment, and another four stimuli (30 seconds each) were performed at K+ concentrations of 4 (S2), 7 (S3), 10 (S4), and 13 mmol/L (S5), respectively. In group 2, hearts were perfused with 10 mmol/L K+, and four nerve stimuli (30 seconds each) were given in the absence (S,) and presence of D,L-propranolol at 0.1 (S2), 1 (S3), and 10 ,gmol/L (S4), respectively. Du et al Propranolol, Lidocaine, and Norepinephrine Release TABLE 1. Protocols for Experiments on Neural Norepinephrine Release 1887 Examining the Effect of Propranolol and Other P-Antagonists Sequence of Nerve Stimulation (5 Hz, 30 seconds) Group 1 (n=7) 2 3 4 5 6 7 S, 4/10/10/10/10/10/- S2 4/1 (D,L-propranolol) S3 7/1 (D,L-propranolol) 10/1 (D,L-propranolol) 10/5+5 (L+D-propranolol) 10/5+5 (D+L-propranolol) 10/10 (timolol) S4 10/1 (D,L-propranolol) 10/10 (D,L-propranolol) S5 13/1 (D,L-propranolol) 10/0.1 (D,L-propranolol) 10/10 (L-propranolol) ... 10/10 (D-propranolol) ... 10/10 (atenolol) ... 10/10 (butoxamine) 10/10 (D,L-propranolol) ... 4/4/10 (D,L-propranolol) ... ... Values in the table denote concentrations of perfusate K+ in mmol/L and agents tested in ,umol/L (mmol/Lpmol/L). (n=8) (n=8) (n=8) (n=7) (n=8) (n=7) Downloaded from http://circ.ahajournals.org/ by guest on June 16, 2017 The effect of D- and L-isomers of propranolol on norepinephrine release was tested in groups 3 and 4 with perfusate K' of 10 mmol/L. The first control stimulus (S,, 30 seconds) was followed by another two stimuli (30 seconds each) in the presence of D- or L-propranolol (10 ,umol/L, respectively, S2) or a combination of D- and L-propranolol (5 ,umol/L each, S3). In groups S and 6, hearts were perfused with 10 mmol/L K', and three stimuli (30 seconds each) were performed in the absence (S,) and presence (S2 and S3) of 18-antagonists. The agents presented at S2 and S3 were atenolol (10 ,umol/L, S2) and timolol (10 ,umol/L, S3) for group S and butoxamine (10 ,umol/L, S2) and D,Lpropranolol (10 1tmol/L, S3) for group 6. In comparison, hearts in group 7 were perfused with 4 mmol/L K', and sympathetic ganglion was stimulated twice (30-second duration each) without (S,) and with (S2) D,L-propranolol at 10 ,umol/L. The protocols for this series of experiments are also summarized in Table 1 for clarity. Lidocaine and norepinephrine release. The effect of concentrations of lidocaine on norepinephrine release was examined in two groups of hearts (n=7 each) perfused with 4 or 10 mmol/L K', respectively. Nerve stimulation was performed five times (30 seconds each) in the group perfused with 10 mmol/L K' or six times (30 seconds each) in the group perfused with 4 mmol/L K+. The first stimulation served as control (S,), and concentrations of lidocaine tested were 0.1 (S2), 1 (S3), 10 (S4), 100 (S5), and 400 ,umol/L (S6), respectively. Propranolol, lidocaine, and norepinephrine release with low pH. Effects of D,L-propranolol and lidocaine on norepinephrine release at a reduced pH were examined in three groups of hearts (all n=7) perfused with 4 mmol/L K'. The perfusate pH was reduced by lowering NaHCO3 from 25 mmol/L to 7 mmol/L, and NaCl concentration was increased accordingly. The final pH was adjusted to 6.8 to 6.9 (average, 6.85) by the addition of concentrated HCl. In all three groups, the first nerve stimulus (S,, 1 minute) was performed at normal pH of 7.4. Then the perfusate pH was reduced to 6.85, and the second and third stimuli (1 minute each) were applied after 10 (S2) or 25 minutes (S3) of perfusion with low pH buffer. Group 1 served as the control, and D,L-propranolol (group 2) or lidocaine (group 3) was presented at S2 (1 ,umol/L) and S3 (10 ,umol/L), respectively. ... ... ... ... ... ... Propranolol, lidocaine, and norepinephrine release in ischemia. Effects of D,L-propranolol and lidocaine on norepinephrine release in ischemic hearts were tested. Five groups of hearts (n=7 to 10) were perfused with 4 mmol/L K' and subjected to three periods of 6-minute total ischemia separated by 15-minute intervals of perfusion at 5 mL- g- min- . Nerve stimulation (5 Hz, 1 minute) were performed in the final minute of ischemic periods. Group 1 served as control and received no drug treatment. In the remaining four groups, propranolol (two groups) or lidocaine (two groups) were infused 10 minutes before the second and third periods of ischemia (0.01 and 0.1 pimol/L for one group and 1 and 10 ,umol/L for one group, respectively). Previous studies have shown that there is no ischemia-induced norepinephrine release by periods of total ischemia less than 10 minutes.23 Statistical Analysis Results are expressed as mean±SEM. Whenever possible, each animal served as its own control to eliminate between-animal variation in quantitative norepinephrine release and to improve statistical power. Therefore, norepinephrine data are presented both in absolutes and in percentage of individual values measured before and after an intervention. Differences were tested for statistical significance by one- or twoway ANOVA, followed by paired- or unpaired Student's t test. Bonferroni's correction was performed for comparison of repetitive measurements between groups. P<.05 was considered significant. Results Basal norepinephrine release was always low (0 to 1.3 pmol* g`. min') and not influenced by perfusion with increased K' concentrations (4 mmol/L: 0.7+0.2 pmol* g.* min-1, 10 mmol/L: 1.0+0.1 pmol * g`-* min'. P=NS). In control hearts, quantities of norepinephrine release evoked by S1S5 were not significantly different within or between groups (P=NS by ANOVA or paired t test: 4 mmol/L K', 34.0±3.9, 36.2+4.1, 33.8+4.6, 34.4±5.8, and 33.5+±5.5 pmol/g, respectively; 10 mmol/L K+, 37.1+5.0, 39.9±6.2, 34.6+5.8,33.1±4.8, and 31.9±4.3 pmol/g, respectively). The percentages of S2SS over S, (individual control) were 108±4%, 99±7%, 97±10%, and 95 +8%, respectively, for the group with 4 mmol/L K' and 107+7%, 91+±6%, 89+5%, and 86+6%, respectively, for Circulation Vol 88, No 4, Part 1 October 1993 1888 i 50 Propranolol (1 FM)- 60 40- .DI 30 - ,40 30 20.- * z * 10* . n t) - as 4 4 7 10 Potassium concentration (mM) 13 30 0 a .1 20 * 10Downloaded from http://circ.ahajournals.org/ by guest on June 16, 2017 nAv . 0 0.1 1 20. 0 Si 10 0 *5E 3 E*S2 C D D+L C L L+D C A T C B P C P FIG 2. Bargraph of effects of -adrenoceptorantagonists (all at 10 munolIL) and stereoisomers of propranolol (both at S pimol/L) on norepinephrine (NE) release in response to nerve stimulation in hearts perfused with 4 mmolIL or 10 mmolIL K+. Sympathetic ganglion was stimulated at 5 Hz for a period of 30 seconds. n = 7 or 8 per group. D indicates D-propranolol; L, L-propranolol; C, control; A, atenolol; T, timolol; B, butoxamine; and P, D,L-propranolol. * P<.05 and **P<.I001 versus control values in the same group by paired t test. [K+J 10mM z 40 he 4mM 1 9 .50 he 0. [K'1 [K-] 10 mM | 10 Propranolol (AM) FIG 1. Top, Plots of influence ofperfusate K' concentration on the inhibition of nerve stimulation (5 Hz for 30 seconds) mediated norepinephrine (NE) release by D,L-propranolol at 1 jumol/L (n= 7). Bottom, Plot of inhibition by varying concentrations of DL-propranolol of norepinephrine release induced by sympathetic ganglion stimulation (5 Hz for 30 seconds) in hearts perfused with 10 mmol/L K' (n =8). *P<.01 versus the values by control stimulation (S,, without propranolol) by paired t test. - the group with 10 mmol/L K' (P=NS for within- and between-group comparisons). Propranolol and Norepinephrine Release at Increased K' DL-Propranolol at 1 ,umol/L failed to modify norepinephrine release induced by nerve stimulation during perfusion with 4 mmol/L K' but showed a progressively enhanced inhibition of such release with increasing perfusate K' from 7 to 13 mmol/L (F=6.91, P<.01 by ANOVA, 7 mmol/L: -44±11%, 10 mmol/L: -50±7%, and 13 mmol/L: -59±9%, all P<.01 by paired t test versus Si, Fig 1). At 10 mmol/L perfusate K', inhibition of norepinephrine release by propranolol was dose dependent (F=25.8, P<.001; 0.1 1£mol/L: -7.7±10.3%, P=NS; 1 Mimol/L: -53.5±4.0%, P<.01; and 10 ,umol/L: -63.7±6.0%, P<.001, Fig 1). At 4 mmol/L K', D,L-propranolol of 10 limol/L was ineffective in modifying norepinephrine release with an S2/S1 ratio of 110±8%. With 10 mmol/L K', norepinephrine release was not influenced by atenolol or timolol at 10 gmol/L but was inhibited moderately by 10 ,umol/L butoxamine (-32±9%, P<.05) and markedly by 10 gmol/L D,L-propranolol (-69±5%, P<.001, Fig 2). Administration of D- or L-propranolol alone significantly suppressed norepinephrine release to a similar extent to that observed by the combination of the two isomers (-55±5% versus -59±8% and -53±9% versus -59±8%, both P=NS, Fig 2). There was a good correlation between the reduction of norepinephrine release produced by either of the two isomers and that by simultaneous infusion of both isomers (r=.80, P<.01, n=16). Lidocaine and Norepinephrine Release at 4 and 10 mmol/L K' In hearts perfused with 4 or 10 mmol/L K', basal norepinephrine overflow remained low and not affected by lidocaine even at 100 1umol/L (0.68±0.22 versus 1.01+0.11 pmol*g 1 min', P=NS). There was no significant difference in norepinephrine release by S, in groups with 4 or 10 mmol/L K' (49.3+6.7 versus 41.2+9.5 pmol/g). With 4 mmol/L K', norepinephrine release in response to nerve stimulation was not significantly affected by lidocaine until the concentration was 10 ,tmol/L or above (P<.02, Fig 3). In contrast, in hearts with 10 mmol/L K', there was a dose-dependent suppression of norepinephrine release by lidocaine that was statistically significant starting at 0.1 limol/L (F=8.54, P<.001 by two-way ANOVA for overall difference at a dose of 0.1 to 100 ,tmol/L, Fig 3). The average dose required to suppress norepinephrine release by 50% of control (IC50) was about 70 ,umol/L with 4 mmol/L K' and 0.5 ,umol/L with 10 mmol/L K'. Effects of Propranolol and Lidocaine on Basal Heart Rate at 4 and 10 mmol/L K' Basal heart rate remained stable in hearts perfused with 4 or 10 mmol/L K' (244+6 and 232±9 beats per minute, P=NS, combined data from 20 and 47 hearts, respectively). Both D,L-propranolol and lidocaine reduced basal heart rate, in a concentration-dependent manner, with 4 or 10 mmol/L K'. Interestingly, for both agents, the dose-response curves of heart rate reduction were similarly shifted leftward by an increased perfusate K+ concentration (Fig 4). At 10 mmol/L K', D- and L-isomers of propranolol at 10 gmol/L reduced basal heart rate to a similar extent to that produced by 10 11mol/L D,L-propranolol (-162±+6 and -151±8 versus -165±6 beats per minute, P=NS). Propranolol, Lidocaine, and Norepinephrine Release: Effect of Metabolic Acidosis Norepinephrine release evoked by the first stimulus (S,) at normal pH was similar in all three groups. In the Du et al Propranolol, Lidocaine, and Norepinephrine Release 1889 100. 80- 05 0 U z El 60- rw z 40- si S2 a ~. --0- Contl Pmpranlol Lio 200 1 pH74a pH 7.40 H68 pH 6.85 (10 mmn) * ~j X S3 pH6.5 pH 6.8S (25 min) FIG 5. Plot of effects of DL-propranolol and lidocaine on evoked norepinephrine (NE) release in perfused hearts with metabolic acidosis (pH reduced from 7.40 to 6.85, K+ =4 mmol/L). The sympathetic ganglion was stimulated (5 Hz for 1 minute) once at a perfusatepHof7.4 (S,) and a further two times after 10 and 25 minutes ofperfusion at a pHof 6.85 (S2 and S3, respectively). Propranolol or lidocaine were presented 10 minutes before and during 52 at 1 limol/L and 10 minutes before and during 53 at 10 ,umol/L. n=7per group. *P<. 05 and 'P <. 0 versus individual values at pH 7.4 (S,) in the same group by paired t test. 0 U Wo z Downloaded from http://circ.ahajournals.org/ by guest on June 16, 2017 Lidocaine (-Log M) FIG 3. Plots of effects of varying concentrations of DLpropranolol or lidocaine on norepinephrine (NE) release induced by sympathetic ganglion stimulation (5 Hz for 30 seconds) in hearts perfused with 4 mmol/L or 10 mmol/L K+. Results are presented as percentages of the individual values of NE release without drugs (S,). *Denotes a significant difference between the 4 and 10 mmol/L K' groups by unpaired t test with Bonferroni's correction. n = 7 or 8 in each group. Propranolol, Lidocaine, and Norepinephrine Release in Myocardial Ischemia In hearts preperfused with 4 mmol/L K' and subsequently undergoing three periods of 6-minute total ischemia, norepinephrine release evoked by nerve stimulation was reproducible in the control group (Table 2). Treatment with DL-propranolol or lidocaine before ischemia resulted in a significant and dose-dependent inhibition of norepinephrine release starting at a concentration of 0.1 limol/L versus S, without drug (Table 2 and Fig 6). In the control group, each nerve stimulation (S1S3) during ischemia induced a significant increase in heart rate (+32±9, +32±9, and +36±10 beats per minute, respectively). This chronotropic response to nerve stimulation in the ischemic heart was partly or totally inhibited by lidocaine and propranolol (data not shown). control group, norepinephrine release was not affected by 10-minute perfusion (104±7% of S,, P=NS) but was reduced by 25-minute perfusion with the acidic buffer (79±t8% of S,, P<.05, Fig 5). In groups receiving drug treatment, DL-propranolol or lidocaine at 1 ,umol/L did not reduce norepinephrine release after 10-minute acidic perfusion (101±6% or 93±5% of S,, respectively, all P=NS). A 25-minute acidic perfusion together with propranolol of 10 limol/L suppressed norepinephrine release to 43±7% of S, (P<.01), a value significantly lower than the control group without drug treatment (P<.01). In the presence of lidocaine at 10 Mmol/L, norepinephrine release by S3 tended to be lower than the control group (56±10%, P=.09), but this was statistically insignificant. Acidic perfusion profoundly suppressed the systolic ventricular pressure during basal and nerve stimulation (data not shown). Discussion The present study demonstrates a dose-dependent inhibition of neural norepinephrine release by propranolol only at an increased [K']. and, to a lesser extent, at a reduced extracellular pH. Lidocaine, a specific Na' channel blocker, shows a very similar inhibitory effect on norepinephrine release with a marked potentiation 240 a 200 .0 160 -0- 4mM K+ 10mM K+ FIG 4. Plots of heart rate-lowering activity of DL-propranolol and idocaine and the potentiation by increasingK+ concentration from 4 to 10 mmoliL. Note the similar leftward shift of the dose-response curves for both agents by 10 mmol/L K' (arrows). HR indicates heart rate. / 804 r. 40. U ~0is 0 0 0.1 1.0 10 Concentration of propranolol (piM) 0 0.1 1 10 100 Concentration of lidocaine (gM) 1000 Circulation Vol 88, No 4, Part 1 October 1993 1890 TABLE 2. Effects of D,L-Propranolol (0.01 to 10 jumol/L) and Lidocaine (0.01 to 10 gmol/L) on the Neural Norepinephrine Release (pmollg) in Hearts Perfused With 4 mmol/L K+ and Subjected to 6-Minute Periods of Total Ischemia Group 1 (n=7) 2 (n=9) Drug None Propranolol 3 (n=10) Propranolol 4 (n=9) Udocaine 5 (n=8) Udocaine Nerve stimuli (S1S3) were applied treatment. *P<.001 vs S1 33.0+5.2 43.8+3.1 Downloaded from http://circ.ahajournals.org/ by guest on June 16, 2017 r1-rT 1T 80 oo a 0.01 gM * 0.1 pM 10LM * 10~±M * 20 * 40. 1- z 27.7+4.3 38.3±4.0 (0.01 ,umol/L) S1 in the same group by paired t test. Mechanism of the Inhibition of Norepinephrine Release by Propranolol or Lidocaine at High [K'], Several mechanisms could account for the inhibition of neural norepinephrine release by propranolol. As this inhibition is observed only at raised [K'], of 7 to 13 mmol/L, an inhibition by high K' of norepinephrine release is possible. Although in some models hyperkalemia alone can inhibit evoked norepinephrine overflow and postsynaptic responses,14,2425 previous studies and the present study with this model show no effect on norepinephrine release by increasing perfusate K' up to 13 mmol/L.19 Blockade of facilitatory presynaptic R2adrenoceptors could lead to a reduced norepinephrine release.6 In this model with a normal K', however, propranolol fails to suppress norepinephrine release - S3 30.2±4.5 27.3±3.6* (0.1 ,umol/L) 31.0+4.3 12.7±2.9* 5.8±0.6* (1 limol/L) (10 gmol/L) 45.3±5.7 33.7+5.7 28.1+±5.2* (0.1 ,umol/L) (0.01 umol/L) 46.4+6.8 17.4±4.6* 3.1+±0.4* (1 ,umol/L) (10 ,umol/L) in the last minute of ischemic periods. S1 served as a reference without drug by raised [K'].. Finally, norepinephrine release in ischemic hearts is dose dependently suppressed by both agents. 100- S2 0 20 Propanolol Ldocaine FIG 6. Bar graph of inhibition of neural norepinephrine (NE) release by concentrations of DL-propranolol and lidocaine in the ischemic heart. Data have been presented as percentages of the NE overflow by a control nerve stimulation in the absence ofdrug treatment (S,=100%) calculated from the absolutes presented in Table 2. In the control group (n = 7), there was no significant difference in the amount of NE released by S2 and 53 compared with that by S, (92.8±7.0% and 102.3+13.7% of 5,, respectively). Note the dose-dependent inhibition of NE release by both agents in the ischemic conditions. *P<.001 versus individual control values released by S, in the same group (paired t test). according to our previous and the present studies.18 Further evidence against such a possibility comes from the findings that the inhibitory effect of propranolol is not shared by timolol, a potent nonselective (-blocker, and that the two isomers of propranolol, with and without 13-blocking activity, are equally effective in the suppression of norepinephrine release at an increased [K'].. Finally, the inhibition of norepinephrine release by lidocaine is also potentiated by a raised [K']., and this again does not indicate a presynaptic f3-adrenergic mechanism. A mild inhibition of norepinephrine release was observed by butoxamine, a relatively selective 82antagonist, at 10 mmol/L K'. This is probably due to effects other than blockade of presynaptic P2-adrenoceptors, and the properties of butoxamine are still only partly understood. Propranolol also possesses membrane stabilizing activity, including the inhibition of Ca2' and Na+ channels.7 Theoretically, blockade of either channel (N-type Ca21 channels for neuronal tissues) could lead to an inhibited neurotransmission, as action potential propagation along the axons is mediated by Na+ influx and norepinephrine exocytosis is the result of Ca21 influx at the nerve varicosities. The dependency of the effect of propranolol on [K']. suggests that Ca21 channels are not involved as they function at near-zero membrane potential and therefore should not be sensitive to increased [K']. to the levels studied. In contrast, the functional state of Na+ channels depends on the resting membrane potential, which is in turn determined by the K' gradient across the membrane.9 The similar effect of lidocaine on both norepinephrine release and heart rate at increased [K']. provides further support for a Na+ channel-dependent mechanism. In our study, propranolol is also synergistic with an increased [K']. in the suppression of the basal heart rate. Sinus automaticity is determined by the rate of spontaneous depolarization of the resting membrane potential,26 and the main ionic currents involved in this pacemaking are a background inward Na+ current (IbNa) and a diminishing outward K' current (hk).26 Thus, an inhibition of the Na+ inward current may suppress the automaticity of the sinoatrial node. Du et al Propranolol, Lidocaine, and Norepinephrine Release Downloaded from http://circ.ahajournals.org/ by guest on June 16, 2017 The mechanism for the inhibition of norepinephrine release with raised [K']. may relate to changes in the functional state of Na' channels with a resultant change in the affinity of the channel for the two drugs. Na' channels exist in three functional states: resting (R), open (0), and inactivated (I).27-30 Blockade of Nal channels by drugs is more likely when the channel is in I form, perhaps due to an increased affinity and accessibility of agents to channel-binding sites.27-30 According to the K' equilibration potential Ek, an increase in [K']. from 4 to 10 mmol/L may lead to a 20-mV depolarization of the resting membrane potential,9 and this could result in an inactivation of about 90% of Na' channels. There is evidence that lidocaine binds mainly to Na' channels in I form, thereby blocking channels and inhibiting the transition of functional states from I to R. In addition, after binding with lidocaine, channel reactivation requires a much more negative membrane potential.27-30 This is largely prevented by a high [K+]0induced partial depolarization, leading to a progressively increased channel blockade. Studies have indeed shown that an increased [K']. enhances the depressant effects of lidocaine and other class I antiarrhythmic agents on the electrophysiology of myocytes.10-12'28 Thus, we speculate that a synergistic inhibition of Na' channels by propranolol or lidocaine and an increased [K']. is the ionic mechanism for the inhibition of norepinephrine release observed. Further studies are required to confirm this mechanism in neuronal preparations. Contribution of Metabolic Acidosis Reduction of external pH to 6.85 for 25 minutes had only a minor effect on neural norepinephrine release, in keeping with our previous observation.31 At the reduced pH, propranolol at 10 1£mol/L reduced norepinephrine release by 37%, although no such synergism was observed at 1 ,umol/L. The same tendency was also found for lidocaine. This could be due to both higher drug concentration and development of intracellular acidosis, via an enhanced H+/K' and inhibited H+/Na+ exchange,9'32 following longer acidotic perfusion. Potentiation by acidosis of the electrophysiological effects of lidocaine has been previously demonstrated.15"1628 Reduction in pH reduces Vma. and the resting membrane potential, which is due to an enhanced K' efflux via H+/K' exchange and a suppressed Na+/K+ ,ATPase.9"11,1516,28 Following reduction in the resting membrane potential, the fraction of inactivated Na+ channels may increase and hence the blockade of the Na+ channel by drugs."1128 In addition, acidosis lengthens the action potential duration, which may increase the time constant of recovery for the blocked and inactivated channels.1128 The present study provides data showing that the synergism of acidosis and Na+ channel blocker, observed previously in Purkinje fibers or myocytes, also pertains to the presynaptic adrenergic nerves. Inhibition of Neural Norepinephrine Release in Ischemic Heart Acute ischemia rapidly leads to an increase in [K']. and acidosis,8'9 and propranolol has no effect on the rise in [K+]0.8,33 Our results indicate that propranolol and lidocaine, while having little effect on norepinephrine release under physiological conditions, show a potent and dose-dependent inhibition of neural norepineph- 1891 rine release in the ischemic heart with a threshold effective dose of 0.1 ,umol/L. The extent of the inhibition of norepinephrine release by either propranolol or lidocaine at 10 ,mol/L is more pronounced in ischemia (-88.5% and -90%, respectively) than during normoxic perfusion with 10 mmol/L K' (-59---69% for propranolol and -75% for lidocaine), suggesting that additional factors in ischemia, such as acidosis and hypoxia,"1"15"16,28'34 may also contribute to the observed drug effect. Our experiments with acidosis support this view. However, a raised [K']. is by far the most important component. Interestingly, our results are in keeping with the findings from a study in in vivo rats with coronary artery occlusion.35 In that study, the myocardial norepinephrine content was unchanged, but a marked reduction in the density of fluorescing adrenergic fibers was found in the ischemic area after 60 minutes of local ischemia, indicating a local release and accumulation of norepinephrine in the ischemic zone. These changes could be partly or completely prevented by pretreatment with different doses of lidocaine.35 Our study provides direct evidence for the mechanism of this inhibited norepinephrine release in vivo. Clinical Implications Propranolol and lidocaine are effective in the suppression of malignant arrhythmias and cellular damage in the acute phase of myocardial infarction,'-5 20 and adrenergic involvement in these processes has been supported by a large number of studies.5,9,19 However, few of the previous studies have linked these therapeutic effects with norepinephrine release in the ischemic myocardium. The inhibition of neural norepinephrine release demonstrated in this study is likely to contribute to the therapeutic effects of propranolol and lidocaine in myocardial ischemia. This may also be the case for other class I and III antiarrhythmic agents. Our data may also help to explain the clinical findings that the class I antiarrhythmic agents, although particularly effective in suppressing ischemic arrhythmias, are much less effective in the attenuation of ventricular arrhythmias induced when exogenous catecholamines are given.Y6-38 This difference in efficacy of antiarrhythmic activity may indicate that suppression of endogenous norepinephrine release is an additional mechanism for the potent antiarrhythmic property of class I agents in ischemia. In addition, although clinical studies have shown that 3-blockers without membrane stabilizing activity reduce sudden cardiac death in patients after acute myocardial infarction,' it is not known if they are as effective as those with such activity in the inhibition of ventricular arrhythmias during acute myocardial ischemia. The generally accepted concept that the membrane stabilizing activity of ,3-antagonists is of little therapeutic importance is based primarily on data collected under physiological conditions. By simulating the metabolic changes seen in acute myocardial ischemia, we have shown a suppression of norepinephrine release by propranolol at concentrations found clinically.39-41 The importance of the experimental environment in the assessment of drug effects in cardiovascular tissues has been stressed by previous studies.9-6,28 The present study, concerning neural norepinephrine release during myocardial ischemia, provides another example of this 1892 Circulation Vol 88, No 4, Part 1 October 1993 issue whereby ischemic changes amplify drug effects leading to unexpected pharmacological actions. Acknowledgments The Cardiovascular Research Unit is supported by the British Heart Foundation. The part of this project conducted in Baker Medical Research Institute was supported by grants from the Alfred Group of Hospitals, Melbourne, and BP Australia Ltd. The excellent technical assistance of Miss Margaret Millar and Mrs Jean Samuel is greatly acknowledged. We thank Dr A. Ungar for his generous supply of butoxamine. We are grateful to Professor James Angus and Professor Murray Esler for their support with laboratory facilities. We also wish to thank Miss Helen Cox and Miss Andrea Turner for their help in the catechol assay. References Downloaded from http://circ.ahajournals.org/ by guest on June 16, 2017 1. Yusuf S, Peto R, Lewis J, Collins R, Sleight P. Beta blockade during and after myocardial infarction: an overview of the randomized trials. Prog Cardiovasc Dis. 1985;27:335-371. 2. Norris RM, Barnaby PF, Brown MA. Prevention of ventricular fibrillation during acute myocardial infarction by intravenous propranolol. Lancet. 1984;2:883-886. 3. Hjalmarson A, Olsson G. Myocardial infarction: effects of /3-blockade. Circulation. 1991;84(suppl VI):VI-101-VI-107. 4. Peter T. Norris RM, Clarke ED. Reduction of enzyme levels by propranolol after acute myocardial infarction. Circulation. 1978;57: 1091-1095. 5. Corr PB, Yamada KA, Witkowski FX. Mechanisms controlling cardiac autonomic function and their relation to arrhythmogenesis. In: Fozzard HA, Haber E, Jennings RB, Katz AM, eds. The Heart and Cardiovascular System: Scientific Foundations. New York, NY: Raven Press, Publishers; 1986:1343-1404. 6. Majewaki H. Modulation of noradrenaline release through activation of presynaptic 3-adrenoceptors. J Auton PharmacoL 1983; 3:47-60. 7. Smith HJ. The need to redefine membrane stabilizing activity of beta-adrenergic receptor antagonists. J Mol Cell Cardiol 1982;14: 495-500. 8. Kl6ber AG. Extracellular potassium accumulation in acute myocardial ischemia. J Mol Cell Cardiol. 1984;16:389-394. 9. Gettes LS, Cascio WE. Effect of acute ischemia on cardiac electrophysiology. In: Fozzard HA, Haber E, Jennings RB, Katz AM, Morgan HE, eds. The Heart and Cardiovascular System: Scientific Foundations. 2nd Ed. New York, NY: Raven Press, Publishers; 1991:2021-2054. Obayashi K, Hayakawa H, Mandel W. Interrelationships between external potassium concentration and lidocaine: effects on canine Purkinje fiber. Am Heart J. 1975;89:221-226. 11. Ye VZ, Wyse KR, Campbell TJ. Lidocaine shows greater selective depression of depolarized and acidotic myocardium than propafenone: possible implications for proarrhythmia. J Cardiovasc Pharmacol. 1993;21:47-55. 12. Singh BN, Vaughan-Williams EM. Effect of altering potassium concentration on the action of lidocaine and diphenylhydantoin on rabbit atrial and ventricular muscle. Circ Res. 1971;26:286-295. 13. Kodama I, Wilde A, Janse MJ, Durrer D, Yamada K. Combined effects of hypoxia, hyperkalemia and acidosis on membrane action potential and excitability of guinea-pig ventricular muscle. J Mol Cell Cardiol. 1984;16:247-259. 14. Miyazaki T, Zipes DP. Presynaptic modulation of efferent sympathetic and vagal neurotransmission in the canine heart by hypoxia, high K', low pH, and adenosine. Circ Res. 1990;66:289-301. 15. Grant AO, Strauss LU, Willance AG, Strauss HC. The influence of pH on the electrophysiological effects of lidocaine in guinea pig ventricular myocardium. Circ Res. 1980;47:542-550. 16. Nattel S, Elharrar V, Zipes DP, Bailey JC. pH-Dependent electrophysiological effects of quinidine and lidocaine on canine cardiac Purkinje fibers. Circ Res. 1981;48:55-61. 17. Rogart R. Sodium channels in nerve and muscle membrane. Ann Rev Physiol. 1981;43:711-725. 18. Dart AM, Dietz R, Hieronymus K, Kdbler W, Mayer E, Schomig A, Strasser R. Effects of a- and P-adrenoceptor blockade on the 10. neurally evoked overflow of endogenous noradrenaline from the rat isolated heart. BrJ Pharmacol. 1984;81:475-478. 19. Du X-J, Dart AM, Riemersma RA. Sympathetic activation and increased extracellular potassium: synergistic effects on cardiac potassium uptake and arrhythmias. J Cardiovasc Pharmacol. 1993; 21:977-982. 20. Lie KI, Wellens HJ, van Capelle FJ, Durrer D. Lidocaine in the prevention of primary ventricular fibrillation: a double-blind, randomized study of 212 consecutive patients. N Engl J Med. 1974; 291:1324-1326. 21. Da Prada M, Zurcher G. Simultaneous radioenzymatic determination of plasma and tissue adrenaline, noradrenaline and dopamine within the femtomole range. Life Sci. 1976;19:1161-1174. 22. Medvedev OS, Esler MD, Angus JA, Cocks HS, Eisenhofer G. Simultaneous determination of plasma norepinephrine and adrenaline kinetics. Naunyn Schmiedebergs Arch Pharmacol. 1990; 341:192-199. 23. Schomig A, Dart AM, Dietz R, Mayer E, Kubler W. Release of endogenous catecholamines in the ischemic myocardium of the rat: Part A. locally mediated release. Circ Res. 1984;55:689-701. 24. Forfar JC, Riemersma RA. Metabolic modulation of cardiac neurosympathetic activity in vivo: effects of potassium and adenosine. Cardiovasc Res. 1987;18:427-437. 25. Borda L, Shuchleib R, Henry PD. Effects of potassium on isolated canine coronary arteries: modulation of adrenergic responsiveness and release of norepinephrine. Circ Res. 1977;41:778-786. 26. Brown HF. Electrophysiology of the sinoatrial node. Physiol Rev. 1982;62:506-530. 27. Fozzard HA, Hanck DA. Sodium channels. In: Fozzard HA, Haber E, Jennings RB, Katz AM, Morgan HE, eds. The Heart and Cardiovascular System: Scientific Foundations. 2nd Ed. New York, NY: Raven Press, Publishers; 1991:1091-1120. 28. Hondeghem LM, Katzung BG. Antiarrhythmic agents: the modulated receptor mechanism of action of sodium and calcium channel-blocking drugs. Ann Rev Pharmacol ToxicoL 1984;24: 387-423. 29. Grant AO, Wendt DJ. Block and modulation of cardiac Na+ channels by antiarrhythmic drugs, neurotransmitters and hormones. Trends Pharmacol Sci. 1992;13:352-358. 30. Hille B. Local anesthetics: hydrophilic and hydrophobic pathways for the drug-receptor reaction. J Gen Physiol 1977;69:497-515. 31. Dart AM, Riemersma RA. Effects of acidosis on anoxic and exocytotic noradrenaline release from the heart. J Mol Cell CardioL 1989;21:75-83. 32. Skinner RB, Kunze DL. Changes in extracellular potassium activity in response to decreased pH in rabbit atrial muscle. Circ Res. 1976;39:678-683. 33. Knopf H, McDonald FM, Bischoff A, Hirche HJ, Addicks K. Effect of propranolol on early postischemia arrhythmias and norepinephrine and potassium release of ischemic myocardium in anesthetized pigs. J Cardiovasc PharmacoL 1988;12(suppl 1):S41-S47. 34. Hondeghem LM, Grant AO, Jensen RA. Antiarrhythmic drug action: selective depression of hypoxic cells. Am Heart J. 1974;87: 602-605. 35. Polwin W, McDonald FM, Brinkman C, Hirche H, Addicks K. Effects of lidocaine on catecholamine release in the ischemic rat heart. J Cardiovasc Pharmacol. 1987;9:6-11. 36. Morady F, Kou WH, Kadish AH, Nelson SD, Toivonen LK, Kushner JA, Schmaltz S, deBuitleir M. Antagonism of quinidine's electrophysiologic effects by epinephrine in patients with ventricular tachycardia. JAm Coil CardioL 1988;12:388-394. 37. Jazayeri MR, VanWyhe G, Avitall B, McKinnie J, Tchou P, Akhtar M. Isoproterenol reversal of antiarrhythmic effects in patients with inducible sustained ventricular tachyarrhythmias. JAm Coil Cardiol. 1989;14:705-711. 38. Calkins H, Sousa J, El-Atassi R, Schmaltz S, Kadish A, Morady F. Reversal of antiarrhythmic drug effects by epinephrine: quinidine versus amiodarone. J Am Coll Cardiol. 1992;19:347-352. 39. Coltart DJ, Gibson DG, Shand DG. Plasma propranolol levels associated with suppression of ventricular ectopic beats. BMJ. 1971;1:490-491. 40. Woosley RL, Kornhauser D, Smith R, Reele S, Higgins SB, Nies AS, Shand DG, Oates JA. Suppression of chronic ventricular arrhythmias with propranolol. Circulation. 1979;60:819-827. 41. Pine M, Favrot L, Smith S, McDonald K, Chidsey CA. Correlation of plasma propranolol concentration with therapeutic response in patients with angina pectoris. Circulation. 1975;52:886-893. Propranolol and lidocaine inhibit neural norepinephrine release in hearts with increased extracellular potassium and ischemia. X J Du, R A Riemersma, K A Fox and A M Dart Downloaded from http://circ.ahajournals.org/ by guest on June 16, 2017 Circulation. 1993;88:1885-1892 doi: 10.1161/01.CIR.88.4.1885 Circulation is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Copyright © 1993 American Heart Association, Inc. All rights reserved. Print ISSN: 0009-7322. Online ISSN: 1524-4539 The online version of this article, along with updated information and services, is located on the World Wide Web at: http://circ.ahajournals.org/content/88/4/1885 Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in Circulation can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office. Once the online version of the published article for which permission is being requested is located, click Request Permissions in the middle column of the Web page under Services. Further information about this process is available in the Permissions and Rights Question and Answer document. Reprints: Information about reprints can be found online at: http://www.lww.com/reprints Subscriptions: Information about subscribing to Circulation is online at: http://circ.ahajournals.org//subscriptions/