Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
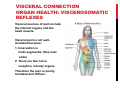
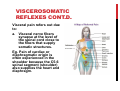
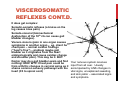
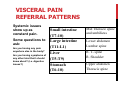
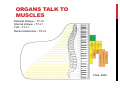
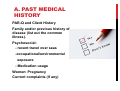
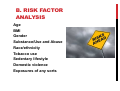
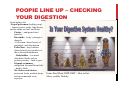
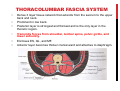
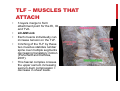
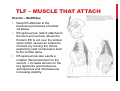
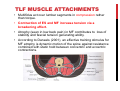
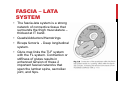
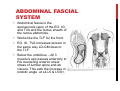
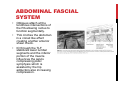
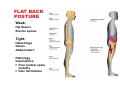
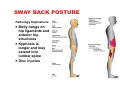
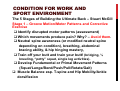
IT DEPENDS! A HOLISTIC VIEW TO DEALING WITH CLIENTS WITH LOW BACK ISSUES PRESENTED BY: BRIAN JUSTIN, MKIN, CEP, CSCS, NKT FMS, HLC2, CHEK-1 OBJECTIVES • To view low back issues with the following perspectives: • Visceral connections • Nutritional connections • Fascial connections • Emotional Connections • Postural connections • Movement Connections BACK FACTS 80% of the population will experience some form of back pain at some point during their lifetime. Back problems account for 40% of all work days missed due to injury or illness. Backache is second only to headache as a common medical complaint. Most back and neck pain stems from lifestyle choices or life experiences. VISCERAL CONNECTION ORGAN HEALTH: VISCEROSOMATIC REFLEXES Visceral sources of pain include the internal organs and the heart muscle. Visceral pain is not welllocalized because: 1. Innervation is multi-segmental. (See next slide) 2. There are few nerve receptors in body organs. Therefore the pain is poorly localized and diffuse. Even Chuck Norris is concerned VISCEROSOMATIC REFLEXES CONT.D. Visceral pain refers out due to: a. Visceral nerve fibers synapse at the level of the spinal cord close to the fibers that supply somatic structures. Eg. Pain of cardiac or diaphragmatic origin is often experienced in the shoulder because the C5-6 spinal segment (shoulder) also supplies the heart and diaphragm. VISCEROSOMATIC REFLEXES CONT.D. B. Viscera have few nerve endings and visceral pleura are insensitive to pain. It is not until the organ capsule is stretched (tumor or inflammation and distention) that pain is perceived. VISCEROSOMATIC REFLEXES CONT.D. It does get complex: Somatic-somatic reflexes (a bruise on the leg causes knee pain). Somato-visceral (biomechanical dysfunction of the 10th rib can cause gall bladder changes). Viscero-viscero (pain in one organ causes symptoms in another organ – eg. client has chest pain – normal cardiac findings (“heart’s fine”) – problem maybe gall bladder as it originates from the heart embryologically and cause cardiac changes and shoulder pain). This may be it. BUT: Doctor may do a gall bladder exam and find nothing! HUH! WTF! Chest pain could be from arthritic changes in cervical spine as it shares common sensory pathways with the heart (C3 to spinal cord) Your nervous system receives input from all over. Usually accompanied by ANS changes in vital signs, unexplained sweating, and skin pallor – associated signs and symptoms. VISCERAL PAIN REFERRAL PATTERNS Systemic issues show up as constant pain. Some questions to ask: Are you having any pain anywhere else in the body? Are you having symptoms of any other kind that I should know about? (i.e. digestive issues?) Small intestine (T7-10) Large intestine (T11-L1) Liver (T5-T9) Stomach (T6-10) Mid Thoracic spine and umbilicus Lower abdomen Lumbar spine R. T- spine R. Shoulder Upper abdomen Thoracic spine ORGANS TALK TO MUSCLES External oblique – T7-12 Internal oblique – T7-L1 TVA – T7-L1 Rectus Abdominis – T5-12 Chek, 2004 AS A KIN WHAT CAN YOU DO ABOUT THIS? Don’t throw up your hands and say, “ well I am not a Doctor, so what can I do about it?” Just be the identifier. Many people do not see their medical provider for symptoms. Before you load them up with training, if you identify something better to have it checked out. Quick Screen A. Past medical history (can be done on your intake/client history form). B. Risk Factor Analysis C. Signs and Symptoms. D. Measurements A. PAST MEDICAL HISTORY PAR-Q and Client History Family and/or previous history of disease (list out the common illness). Psychosocial: - recent travel over seas -occupational/environmental exposure - Medication usage Women: Pregnancy Current complaints (if any) B. RISK FACTOR ANALYSIS Age BMI Gender Substance/Use and Abuse Race/ethnicity Tobacco use Sedentary lifestyle Domestic violence Exposures of any sorts C. SIGNS AND SYMPTOMS Blood in urine, stool, vomit, mucus Client may have filled this out on your client history form. Difficulty chewing/swallowing/speaking But always ask the question: Dribbling or leaking urine Are there any symptoms of any kind anywhere else in your body? Fever, chills, sweats (day or night) Include the list to the right on your client history form as well. Heart palpitations or fluttering Use a review of systems in your client interview. If your client out pours symptoms they have been going through you can see if there are clusters indicating a systemic issue. If so, recommend a check up if you have concerns. Do not tell your client what you think as you are not a diagnostician and is out of your scope of practice just say, “based on what you have told me I would like you to talk to your doctor regarding these symptoms”. Memory loss Changes in bowel or bladder Confusion Cough Dizziness, fainting, blackouts Headaches Joint pain Nausea, vomiting, loss of appetite Numbness or tingling Problems seeing or hearing Skin rash or other changes Sudden weakness Swelling or lumps anywhere Trouble breathing Trouble sleeping Throbbing sensation/pain in bely or anywhere else Unusual fatigue, drowsiness D. MEASUREMENTS Blood pressure (< 144/94 mmHG) Resting Heart Rate (< 100 BPM Resting respiration (rate (10-14) and quality (2/3rd diaphragm and 1/3 chest)) NUTRITION CONNECTION Hierarchy of Health from the Ground up (Fors, 2007) Healthy mind/body/spirit Organ Systems Tissues Cells CHO, PRO, FAT, and Vitamins Earth elements (Hydrogen, etc.) Minerals and trace minerals Earth and its atmosphere NUTRITION’S CONNECTION Food intolerances/Quality Gluten and dairy – may lead to visceral stiffness/bloating leading to core muscle down regulation Artificial sweeteners are implicated in systemic causes of joint pain (Goodman& Snyder, 2007). Of course – quality of food dictates how strong their connective tissue will be. Disc and hydration. Some people think this is a breakfast food! NUTRITION’S CONNECTION Digestion Dysbiosis (bad bacterial growth in lower G.I. tract) is linked to chronic pain and disease (fibromyalgia – Pimentel, et al, 2004). Dysbiosis increases permeability of the small intestine leading to allergies due to absorption of partially digested proteins then spurring on inflammation and with this comes achiness, fatigue, and headaches. Toxins All human beings today store toxins in their tissues. Bell et al (1998), show that low levels of environmental toxins in tissues can cause muscle pain. How? Liver becomes overburdened and cant keep up with the demand. Toxins act like free radicals and accumulate in tissues leading to inflammation and oxidative stress. This leads to painful, stiff and easily fatigued muscles (energy production in tissues affected by above). (Fors, 2007) Vulnerability is based on your client’s biochemical individuality. STEPS FOR THE KIN TO HELP CLIENTS 1. Diet logs (2 weekdays and 1 weekend day) 2. Analyze the number of chemical sources in their diet. 3. Help make better lifestyle choices. 4. Assess digestion. I use this questionnaire from Paul Chek’s excellent manual, How to Eat, Move, and Be Healthy. Scores: 50-130 – High Priority to look into. 30-49 – Moderate priority to look into <30 – Low priority to look into Your nervous system will make adjustments to body systems based on the inputs it gets! This will reflect in movement competency and capacity POOPIE LINE UP – CHECKING YOUR DIGESTION From right to left -Poopie policeman (healthy poop) – formed, passes easily, light brown, smells earthy not foul, and floats. - Flasher – undigested food particles. - Diarrhella – body’s attempt to detoxify. - - Pellet man- altered states of peristalsis and dehydration - Pellet Man – may indicate altered states b/w peristalsis of the colon and dehydration - Bodybuilder – too much dehydrated foods such as protein powders – hard to pass - Olympic swimmers – undigested fat (insufficient bile) – hard to flush. - Mr. Sinker and Stinker – processed foods, medical drugs, and environmental toxin exposure From: Paul Chek, HHP, NMT – How to Eat, Move, and Be Healthy FASCIAL CONNECTIONS Slings: • Thoracolumbar Fascia System (TLF) - Latissimus Dorsi – Gluteus Maximus Link - Obliques – Transversus Abdominis Link - Erector spinae – Multifidus Link • Fascia Lata System - Gluteus Maximus Link - Quadriceps – Hamstring Link Abdominal Fascia System - Rectus abdominis – Obliques/Transversus Link - External oblique – Pectoralis/Serratus Anterior Link - Shoulder girdle – Abdominal Mechanism Link THORACOLUMBAR FASCIA SYSTEM • • • • • • Dense 3 layer tissue network that extends from the sacrum to the upper back and neck. Prominent in low back. Posterior layer is strongest and thickest and is the only layer in the thoracic region. Transmits forces from shoulder, lumbar spine, pelvic girdle, and lower extremity. Encloses ES, QL, and MF. Anterior layer becomes thicker cranial ward and attaches to diaphragm. TLF – MUSCLES THAT ATTACH • • • • • 3 layers merge to form attachment point for the EI, IO, and TVA. LD-GM Link Each muscle individually can increase tension on the TLF. Cinching of the TLF by these two muscles stabilize lumbar spine over multiple segments decreasing translatory motion (Porterfield and DeRosa, 2007). This fascial complex crosses the upper sacrum increasing sacrum-ilium compression = decrease in shear loads. TLF – MUSCLE THAT ATTACH Oblique-TVA Link • Attach at the lateral raphe (junction between posterior and middle TLF layers). • TVA – influences all lumbar levels. • IO – Primarily influences lower lumbar levels. • EO – Primarily influences upper lumbar levels. • TVA and IO have a strong attachment to the middle TLF provide a nearly direct pull to the lumbar transverse process providing excellent segmental stabilization in frontal and transverse planes. TLF – MUSCLE THAT ATTACH Erector – Multifidus • Deep ES attaches to the transverse processes of lumbar vertebrae. • ES aponeurosis (which attaches to the ilium and sacrum) allows the thoracic ES to act over the lumbar spine which causes an extension moment (by moving the thorax posteriorly) and compressive load to the lumbar spine. • ES aponeurosis also exerts a nutation (flexion)moment on the sacrum = increase tension on the key ligaments (sacrotuberous, sacrospinous and interosseous) increasing stability. TLF – MUSCLE ATTACHMENTS • Due to the ES anterior attachment to transverse process it checks anterior shear of lumbar vertebrae. • In concert with the psoas forms an anterior-posterior guy wire contributing compression and providing a dynamic restraint to antpost. shear stress. TLF MUSCLE ATTACHMENTS • Multifidus act over lumbar segments in compression rather than torque. • Contraction of ES and MF increase tension via a broadening effect. • Atrophy (seen in low back pain) in MF contributes to loss of stability and fascial tension generating ability. • According to Daneels (2001), an effective training stimulus for MF atrophy is dynamic motion of the spine against resistance combined with static hold between concentric and eccentric contractions. FASCIA – LATA SYSTEM • The fascia-lata system is a strong network of connective tissue that surrounds the thigh musculature – thickest at IT band. • Quads/Adductors/Hamstrings • Biceps femoris - Deep longitudinal system. • Glute max links the TLF system with the FL system. Contraction or stiffness of glutes results in enhanced tension of these 2 important fascial networks that span the lumbar spine, sacroiliac joint, and hips. ABDOMINAL FASCIAL SYSTEM • Abdominal fascia is the aponeurosis (apo) of the EO, IO, and TVA and the rectus sheath of the rectus abdominis. • Works like the TLF for the front. • EO, IO, TVA increases tension in the same way LD-GM does to the TLF. • Below the umbilicus – All 3 muscle’s apo passes anteriorly to RA countering anterior shear stress of lumbar spine and ab viscera. This aids the increase in lordotic angle at L4-L5 & L5/S1. ABDOMINAL FASCIAL SYSTEM • Obliques attach at the tendinous intersections of the RA allowing rectus to function segmentally. • TVA cinches the abdomen in a corset like effect creating another anterior shear check. • IO through the TLF stabilizes lower lumbar segments and the inferior portion of the muscle influences the pelvis compressing pubic symphysis which is assisted by the hip adductors also increasing compression. SHOULDER GIRDLE TO ABDOMINAL MECHANISM • Rhomboid major/minor attaches from thoracic spinous process to the scapula where it links with the serratus anterior. This then links with the EO and then the contralateral IO making a continuous sling from the shoulder to abdominal wall. SO WHAT DOES ALL THIS MEAN? • Sometimes isolated work is necessary to revascularize or hypertrophy a muscle. • But our bodies are an integrated system, so using multiple muscle groups and motor patterns through muscle slings and anatomical linkages that tie the pelvic and shoulder girdles to the spine should be the training focus. • Biotensegrity • Anatomy Trains • Who is the back picking up the slack for? STRESS CONNECTION (STIFFNESS) See diagram to the right. How does this affect your quality of movement during training? Last nights fight with the girl or boyfriend may elicit a different movement strategy in your client. Habitual hyperventilation (breathing problem) can trigger anxiety/stress (Chaitow, 2008). Depending on the degree of stress produced it can decrease mobility of the vertebra (Schafer, 1987). Stress Sympathetic Activation Sends out TGF-beta-1 cytokine to elicit an immune response 1. Immune system – T3 2. Myofibroblast activation (increases fascial stiffness) ANXIETYBREATHING STRESS AND KNOTS Recurrent physical (injury/ergonomics), chemical (nutrition/toxin), or emotional stress causes muscle fiber contraction. Prolonged contracted muscle fibers squeeze out blood reducing ATP to cells. Poor energy levels do not allow muscle fibers to relax. Creates a self-perpetuating taut band. Any more added stress causes the formation of pain-causing neuromyofascial lesions with abnormal nerve endings. These abnormal nerve endings is what creates that painful trigger point! They will alter your movement patterns. Think of the following: Physical – The obsessed runner who runs through pain daily! Chemical – The client who has a chronic poor diet full of toxins and deficiencies. Emotional – The person with job dissatisfaction. You don’t see these clients do you? ☺ WHAT IS A KIN TO DO? Assess stress via Fantastic Lifestyle Questionnaire or other. Implement stress management coaching Teach myofascial release techniques they can do at work and home. Incorporate myofascial release techniques as needed before training. Calm your client down with some play as a warm up! Lets try one now: ANIMAL MAGNETISM. (Forencich, 2010) POSTURAL CONNECTION Strong abdominals and flexible hip flexors keep the pelvis neutral and the body in alignment LUMBAR HYPER-LORDOSIS Pathology Weak abdominals Implications: and short hip • Highflexors contacttip the pelvisin forward and pressure facetincrease joints. back strain FLAT BACK POSTURE Weak: Hip flexors Erector spinae Tight: Hamstrings Glutes Abdominals? Pathology Implications: Poor lumbar spine mobility Disc herniations SWAY BACK POSTURE Pathology Implications: Body hangs on hip ligaments and anterior hip structures Kyphosis is longer and may extend into lumbar spine Disc injuries MOVEMENT CONNECTION Assess the client’s movement Tools: • Functional Movement Screen • The FMS is a ranking and grading system that documents 7 movement patterns that are key to normal function. By screening these patterns, the FMS readily identifies functional limitations and asymmetries. You will gain knowledge on the stability, mobility, balance, and injury risk of your client. • Core stability is movement pattern specific. • Movement Competence – Kelvin Giles • Gait Analysis • SFMA K. GILES – PHYSICAL COMPETENCE • Physical Competence testing is for the purpose of establishing the athlete/client’s training age and trainability across a wide range of movements. • Data from the competency tests will also form the detail from which the initial training programs will be determined. • It shows the competence in controlled movement rather than the amount of weight carried or the speed of movement. • Very useful for tracking movement improvement from a qualitative perspective but given in a quantitative manner. Gait Movement Pattern Compensations Associated Tests Patellar line drops inside 2nd toe Adductor length Gluteus maximus strength Gluteus medius strength Ant. Tibialis strength Post-Tibialis Strength This is a quick gait analysis. Unequal stride length Achilles line drops in. Ant. Tibialis strength Post. Tibialis Strength Big toe extension Thomas Test Straight leg raise Arm swing inadequate Trendelenburg Sign. Habit Or ask if there is a previous shoulder injury. Add in dorsiflexion test/big toe mobility here too! Gluteus medius strength IMPORTANT MOVEMENT’S TO CLEAR FOR PEOPLE WITH LOW BACK ISSUES Ankle dorsiflexion Hip mobility Thoracic spine mobility Big toe mobility Important to attain mobility in order to get some stability (although some practices challenge this concept) Hip Mobility Test Example Thoracic mobility tests example CORRECTIVE APPROACH (COOK, 2010) Corrective Strategies Approach: 1. Attain mobility first (Passive/Active/Assistive) – this allows more opportunity for sensory input therefore more information for the brain to coordinate stability. The recipe for the brain to make stability (Cook, 2010): a. Structural integrity – pain-free structures without significant damage, deficiency, or deformity. b. Sensory integrity – uncompromised reception and integration of sensory input. c. Motor integrity – uncompromised activation and refinement of motor output. d. Freedom of Movement – mobility adequate to perform within functional ranges and achieve appropriate end ranges and structural alignment. 2. Lock in Stability if improvement in mobility occurs from number 1. CONDITION FOR WORK AND SPORT ENVIRONMENT The 5 Stages of Building the Ultimate Back – Stuart McGill Stage 1 – Groove Motion/Motor Patterns and Corrective Exercise Identify disrupted motor patterns (assessment) Which movements produce pain? Why? – Avoid them. Neutral spine awareness (or modified neutral spine depending on condition), breathing, abdominal bracing ability, & hip hinging mastery, Train off your butt and train your butt! (bridging, ½ kneeling, “potty” squat, single leg activities). Develop Fundamental or Primal Movement Patterns (Squat/Lunge/Bend/Push/Pull/Rotate/Gait) Muscle Balance esp. T-spine and Hip Mobility/Ankle dorsiflexion CONDITION FOR WORK AND SPORT ENVIRONMENT Stage 2 – Build Whole body and Joint Stability The Big Three – McGill Curl, Side Bridge, and Birddog. Build on the Fundamental Patterns. Balance Training (can do daily) – discs, small muscles, and ligaments play apart in position sense to activate key muscles in stabilization (Jemmett, 2003) The Anti - Exrflex Stage 3 – Increase Muscle Endurance Russian Reverse Pyramid for Endurance Training Various options for exercises here depends on client needs. CONDITION FOR WORK AND SPORT ENVIRONMENT Stage 4 – Increase Strength Definitely no “one-size-fits-all” process here. Master body weight movements first. i.e. push ups before presses. Train the lats! – Remember the TLF system? Stage 5 – Power Power is developed in the extremities and transferred through the core! Efficient and effective power transfer through the torso requires spine posture control, spine stiffness and stability, and strength. Do not train spine power. Train power at adjacent joints! TECHNIQUE AWARENESS IN AND OUT OF THE GYM! Consider tissue tolerance – Educate your clients on proper posture and ergonomics. Poor movement and positioning during the day (ie. how they sit at work) reduces tissue tolerance which increases risk of breakdown. Make cognitive association about how alignment during exercise carries over to real life and vice-versa. McGill (2007) J. LEVINE – N.E.A.T. C. HALLFORD – D.A.M.S. Non-exercise activity thermogenesis • Don’t be sentenced to the chair! It kills the back! • Get clients to move as much as they can. DAMS – Daily Activity Modifications • They are used to teach the body how to move more efficiently and decrease wear and tear esp. for injured clients. • An example: Hip hinging before lifting something out of the trunk of your car. • Do as often as possible! • Cognitive Association!