Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Heart failure wikipedia , lookup
Coronary artery disease wikipedia , lookup
Jatene procedure wikipedia , lookup
Myocardial infarction wikipedia , lookup
Antihypertensive drug wikipedia , lookup
Mitral insufficiency wikipedia , lookup
Cardiac surgery wikipedia , lookup
Atrial septal defect wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Lutembacher's syndrome wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
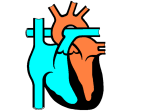
Heart Sounds The familiar lubb-dubb heart sounds are caused by the closing of the heart valves. When the atria are relaxed, they begin to fill with blood. The relaxation is called diastole. As the atria fill, the muscular walls contract, increasing fluid pressure and forcing the AV valves open. Blood flows from the atria into the ventricles. In turn, as the ventricles fill with fluid, they contract. The increasing pressure forces the AV valves shut, producing a lubb sound and pushing blood through the semilunar valves and into the arteries. The contraction is called systole. The ventricles then begin to relax, and the volume in the chambers increases. With increased volume, pressure in the ventricles begins to decrease and blood tends to be drawn from the arteries toward the area of lower pressure. Blood is prevented from reentering the ventricles by the semilunar valves. The closing of the semilunar valves creates the dubb sound. Occasionally, the valves do not close completely. This condition, referred to as a heart murmur, occurs when blood leaks past the closed heart valve because of an improper seal. The AV valves, especially the left AV valve (the bicuspid or mitral valve), must withstand increased pressure and are especially susceptible to defects. The rush of blood from the ventricle back into the atrium produces a gurgling sound that can be detected with the use of a stethoscope. Blood flowing back toward the atrium is inefficient because it is not directed to the systemic or pulmonary systems. The hearts of individuals who experience murmurs compensate for decreased oxygen delivery by beating faster. Diastole: relaxation (dilation) of the heart, during which the cavities of the heart fill with blood. Systole: contraction of the heart, during which blood is pushed out of the heart. A second mechanism helps compensate for a decreased blood flow in people with heart murmurs. Like an elastic band, the more cardiac muscle is stretched, the stronger is the force of contraction. When blood flows from the ventricle, and back into the atrium, blood volume in the atrium increases. The atrium accepts the normal volumes and the additional blood from the ventricle. The extra volume stretches the atrium and drives blood to the ventricle with greater force. The increased blood volume in the ventricle causes it to contract with greater force, driving more blood to the tissues. Research in Canada: Dr. Tofy Mussivand A team of Ottawa reseachers, under the direction of Dr. Tofy Mussivand, is closing in on the production of an artificial heart. The electrohydraulic ventricular device (EVAD) is capable of taking over partial or complete functioning of the ventricles. Unlike other attempts at producing an artificial heart, EVAD is powered and controlled externally by a small battery-powered coil taped to the chest. This eliminates the need for a permanent opening in the skin and allows freedom of movement to patients, as they would no longer need to be attached to a machine. While attending university, Dr. Mussivand learned that millions of people throughout the world were dying of heart disease, yet no one really had a solution. The best available treatment, heart transplants, did not provide the answer. The need for hearts far outstripped the supply of donor hearts and the cost of the operation was prohibitive. The more Dr. Mussivand looked at the options, the more convinced he became that the answer would be an artificial heart. The challenge is largely one of engineering. The question is whether humans can produce a machine that moves fluid as well as a biological system that has evolved over millions of years. A device that assists or takes over the function of a faulty ventricle could save thousands of lives per year.