Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
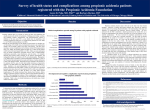
Propionic Acidemia Screening in the Amish and Mennonite Populations Zineb Ammous, MD Clinical Geneticist Medical Director, The Community Health Clinic “Be not conformed to this world….” Romans 12:2 Amish populations by state Topeka Indiana LaGrange/ Elkhart Counties Indiana Plain Church Population over 46,000 • Community supported clinic providing low cost, local care for patients with genetic disorders in the Plain Population of Northern Indiana. • Operations began in Sep 2013 • Now serving over 500 patients from 8 states with more than 100 different disorders. • Newborn screening follow-up for 11 northeastern Indiana counties since July 2013 • Full Service Dental Clinic • Offering Ancillary services to limit required travel – – – – – Medical Home/Care Coordination Dietary services Audiology, Speech Therapy, Occupational Therapy WES and Medical food assistance funds Host the Plain Church Group Ministry Background • Propionic Acidemia (PA) is found in Amish and Mennonite (“Plain”) populations throughout North America. • The founder mutation PCCB c.1606A>G has significant residual enzyme activity making acute neonatal presentations rare and leading to these cases often being described as phenotypically benign and not requiring medical intervention. • However episodic devastating ketoacidotic crises typically occur at times of illness or increased catabolism and can be associated with metabolic strokes resulting in movement disorders and other neurological complications as seen in some patients followed by two of the clinics providing care for Plain children with PA: the Community Health Clinic (CHC) in Indiana and the Clinic for Special Children (CSC) in Pennsylvania. Background • A cohort study performed by the CSC showed that at least 25% of the patients develop cardiac complications and heart failure, often following a minor illness without a metabolic crisis. • Propionyl-carnitine levels are >1000 times higher in the myocardium than the blood. Amino acids & odd chain fatty acids transported into myocardium & oxidized. • Although dilated cardiomyopathy and congestive heart failure can be reversed with treatment in some patients, others may still suffer from metabolic crises, irreversible heart failure, and sudden cardiac death when untreated. [D. Holmes Morton. Cardiomyopathy is common in the propionic acidemia Amish-Mennonite variant PCCBc.1606A>G and can be prevented & reversed by metabolic therapy. Society of Inherited Disorders of Metabolism, Asilomar California March 2014 ] Experience at the CSC [Propionogenesis in Brain: Implications for Management Disorders of Propionate Metabolism. Society for the Study of Inborn Errors of Metabolism, Lyon, France September 2015] Clinic observations of 69 Amish and Mennonite children & adults, homozygous for PCCB C.1606A>G, p.Asn536Asp: • Non-treatment group: historical controls, included 51 patients on selfselected low protein diets. • Treatment Group included 5 neonates managed over 4 years and 13 children & adults (median age 11 yrs, range 4-32 yrs) Treatment = Dietary protein intake of 1 g/kg/day (range 0.3 - 1.7), carnitine 25-100 mg/kg/day, PA-Amino Acid Supplements 0.5-1 g/kg-d, & Citrate 0.5-1 mEq/kg-d. Monitoring: Growth, exams, CBCs, chemistries, plasma amino acids & calculated LAT1-transport, urine methylcitrate/creatinine ratios, urine citrate/methylcitrate ratios, LV-ejection & shortening fractions, and QTc by EKG. OUTCOMES IN UNTREATED PATIENTS • High mortality – 9/51 (18%) • 1 heart transplant • 2/3 of the cardiac deaths were from dilated cardiomyopathy; 1/3 from sudden cardiac death, probably associated with long QTc. Age at death 2-24 yrs. • Neurological outcomes were also poor: seizures associated with illness were common. In some cases recurrent seizures evolved into intractable epilepsy, dystonia arising from internal globus pallidus degeneration, and poor school performance associated with Attention Deficit Hyperactivity Disorder. • Cardiomyopathy, lethal arrhythmias, seizures, encephalopathy, metabolic strokes and cognitive decline occurred at all ages, with or without keto-acidotic crisis. • Hyperammonemia was not reported. OUTCOMES IN TREATED PATIENTS • Cardiomyopathy improved or stabilized. • There were no cardiac deaths or heart transplants. • Seizures were rare, no patient developed epilepsy. • Growth & exams were normal. • Children attended school in normal classes and performances were similar to siblings & parents. Formal IQ-testing was not done. PCCB C.1606A>G IS NOT A BENIGN VARIANT OF PROPIONIC ACIDEMIA!!! Treatment improves cardiac & neurological outcomes. Preventing Newborn Screening Misses Algorithm proposed by Dr. Greg Rice - University of Wisconsin Screening for Propionic Acidemia – Amish variant • Propionyl-carnitine levels in the blood are typically low – often falling below screening MS/MS cut-off values. • The variant was not recognized in the Amish & Mennonite populations in Pennsylvania before MS/MS based NBS started in 1994 • The ratio of C3/C16 carnitine may be the most sensitive and specific value for detecting propionic acidemia. • If the cut-off is C3<5umol/L, 7 of 47 cases (15%) would be False Negatives. • If the cut-off is C3/C16 carnitine ratio < 2.2, all samples would have been positive, none of the 47 would have been reported as False Negative. If the C3/C16 ratio is abnormal then do targeted mutation analysis for PCCB c1606 A>G. (Dr. D. Holmes Morton – SIMD 2014) Screening for Propionic Acidemia – Amish variant Experience at the CSC Missed case in IN in 2013 • A two-week old Amish female presented to the CHC for counseling after receiving DNA results confirming homozygosity for PCCB c.1606A>G. • Initial NBS reported at 2 weeks of life with mild elevation of Tyrosine • Repeat NBS was reported as normal. • The C3 level was 3.60umol/L and 2.138umol/L respectively. • The idea of a high C3 cutoff as a reason for this false negative was considered but lowering it enough to detect all cases with the Amish/Mennonite variant would significantly increase the number of false positives in the general population. • The utility of certain acylcarnitine ratios as secondary screening analytes was questioned: • • • C3/C2: normal on initial screen (0.15), elevated on repeat (0.25) C3/C0: elevated on initial screen (0.19), normal normal on repeat (0.15) C3/C16: normal on initial screen (1.11), elevated on repeat (3.01) These ratios, therefore, are not consistently diagnostic. What about the others? • In addition to this confirmed missed case, we have received reports from community members of several cases of sudden cardiac death in young Amish adults with known family history of PA who were never diagnosed or treated. Their postmortem examination revealed dilated cardiomyopathy and signs of heart failure. Conclusions • These observations and cases suggest that supplemental NBS for unique populations may be merited. Targeted mutation analysis with realtime PCR for the Plain community would enhance specificity for PA and other potentially lifethreatening disorders with known founder mutations. • Other conditions to be considered: SCID - ADA deficiency and RAG1 in the Old Order Amish and IL7R in the Mennonites. Summary • Propionic Acidemia due to homozygosity for PCCB C.1606A>G is one of the most common inherited metabolic disorders in the Plain populations in the United States. • PCCB C.1606A>G is not a benign variant • Identification through NBS and early treatment is crucial in the prevention of neurological and cardiac morbidities and mortality. • Due to low accumulations of propionyl-carnitine, cases can be missed by MS/MS screening. • Supplemental NBS for such unique populations using targeted mutation analysis with real-time PCR should be considered and carefully implemented. Acknowledgments • Christopher Roberson, JD, MPH, director of the Das KIND Program • D. Holmes Morton, MD, founder of the Clinic for Special Children. • CHC and CSC PA Patients and their families