Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
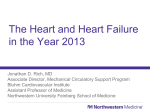
Coronary Physiologic Assessment and Imaging Functional Assessment of Coronary Artery Disease in Patients Undergoing Transcatheter Aortic Valve Implantation Influence of Pressure Overload on the Evaluation of Lesions Severity Gabriele Pesarini, MD; Roberto Scarsini, MD; Carlo Zivelonghi, MD; Anna Piccoli, MD; Alessia Gambaro, MD; Leonardo Gottin, MD; Andrea Rossi, MD; Valeria Ferrero, MD; Corrado Vassanelli, MD; Flavio Ribichini, MD Downloaded from http://circinterventions.ahajournals.org/ by guest on May 2, 2017 Background—Aortic valve stenosis may influence fractional flow reserve (FFR) of concomitant coronary artery disease by causing hypertrophy and reducing the vasodilatory reserve of the coronary circulation. We sought to investigate whether FFR values might change after valve replacement. Methods and Results—The functional relevance of 133 coronary lesions was assessed by FFR in 54 patients with severe aortic valve stenosis before and after transcatheter aortic valve implantation (TAVI) during the same procedure. A linear mixed model was used to verify the interaction of TAVI effect with the FFR values. No significant overall change in FFR values was found before and after the aortic valve stenosis removal (0.89±0.10 versus 0.89±0.13; P=0.73). A different trend in FFR groups (positive if ≤0.8; negative if >0.8) was found after TAVI (P for interaction <0.001). Positive FFR values worsened after TAVI (0.71±0.11 versus 0.66±0.14). Conversely, negative FFR values improved after TAVI (0.92±0.06 versus 0.93±0.07). Similarly, FFR values in coronary arteries with lesions presenting percent diameter stenosis >50 worsened after TAVI (0.84±0.12 versus 0.82±0.16; P=0.02), whereas FFR values in arteries with mild lesions (percent diameter stenosis <50) tended toward improvement after TAVI (0.90±0.07 versus 0.91±0.09; P=0.69). Functional FFR variations after TAVI changed the indication to treat the coronary stenosis in 8 of 133 (6%) lesions. Conclusions—Coronary hemodynamics are influenced by aortic valve stenosis removal. Nevertheless, FFR variations after TAVI are minor and crossed the diagnostic cutoff of 0.8 in a small number of patients after valve replacement. Borderline coronary lesions might become functionally significant after valve replacement, although FFR-guided interventions were infrequent even in patients with angiographically significant lesions. (Circ Cardiovasc Interv. 2016;9:e004088. DOI: 10.1161/CIRCINTERVENTIONS.116.004088.) Key Words: aortic valve stenosis ◼ coronary artery disease ◼ fractional flow reserve, myocardial ◼ myocardial revascularization ◼ transcatheter aortic valve replacement T he prevalence of coronary artery disease (CAD) ranges from 25% to 50% of all patients with aortic valve stenosis (AVS).1 Observational studies reporting outcomes of patients undergoing transcatheter aortic valve implantation (TAVI) revealed a prevalence of CAD in the range of 40% to 75%.2–4 Current guidelines state that myocardial revascularization at the time of surgical aortic valve repair is a class I recommendation in the presence of coronary stenosis ≥70% and a class IIa recommendation for angiographic stenosis 50% to 70%.5 Conversely, the best management of CAD in TAVI candidates is unclear.6 There is no evidence, at present, of increased survival or symptoms relief with a full revascularization strategy, thus raising concerns about the real functional meaning of coronary lesions incidentally found in this specific subset during the routine diagnostic workout. In this context, fractional flow reserve (FFR) measured during diagnostic angiograms may prove useful. Nevertheless, it has been demonstrated that AVS may influence coronary hemodynamics and represents a clinical and physiological condition in which functional indexes may vary consistently.7–9 TAVI has been demonstrated to exert an immediate effect on coronary flow,10 and recently, the immediate improvement in the coronary physiological reserve induced by the aortic valve replacement has been demonstrated using wave intensity analysis.11,12 However, little is known about the functional effects of the pressure overload on coronary stenosis and if, and to which extent, the removal of the outflow obstruction may influence the relation between coronary stenosis and FFR in severe AVS. TAVI can be a useful clinical research model of isolated valvular intervention to unmask underlying valvular–coronary interactions in AVS. Received April 9, 2016; accepted September 26, 2016. From the Division of Cardiology, Department of Medicine, School of Medicine (G.P., R.S., C.Z., A.P., A.G., A.R., V.F., C.V., F.R.) and Department of Anesthesia and Intensive Care (L.G.), University of Verona, Italy. Correspondence to Flavio Ribichini, MD, Division of Cardiology, Department of Medicine, University of Verona, Piazzale Aristide Stefani 1, 37126 Verona, Italy. E-mail [email protected] © 2016 American Heart Association, Inc. Circ Cardiovasc Interv is available at http://circinterventions.ahajournals.org 1 DOI: 10.1161/CIRCINTERVENTIONS.116.004088 2 Pesarini et al Coronary Assessment With FFR in TAVI What Is Known • Coronary artery disease has a high prevalence in patients undergoing transcatheter aortic valve valve implantation (TAVI). • However, coronary hemodynamics is influenced by the presence of severe aortic valve stenosis, and the functional evaluation of coronary stenosis may be altered in this context. • No recommendations are available regarding indication for myocardial revascularization in TAVI candidates. What the Study Adds • Functional assessment with fractional flow reserve is Downloaded from http://circinterventions.ahajournals.org/ by guest on May 2, 2017 a feasible and safe method to determine the severity of coronary artery disease in TAVI patients. • Overall, fractional flow reserve variations after TAVI are minor compared with baseline measurements. • However, post-TAVI functional assessment may change the indication to perform percutaneous coronary intervention in ≈15% of patients with coronary artery disease undergoing TAVI; therefore, functional assessment with fractional flow reserve may be more reliable after the aortic valve replacement. The acute improvement in ventricular mechanics and function due to the removal of severe afterload following successful TAVI may improve coronary blood flow, possibly influencing functional assessment of coronary lesions significance. The purpose of the study is, therefore, to detect eventual changes of FFR values in patients with severe AVS caused by the removal of the aortic valve pressure overload after TAVI. To this aim, FFR values were obtained during the same interventional procedure, before and immediately after transfemoral TAVI. Next, we sought to observe whether functionally significant coronary lesions present at baseline associate with the occurrence of ischemic complications during the transfemoral TAVI procedure and the immediately after procedural period. Methods In this prospective, observational study, FFR measurements were attempted in the 3 major epicardial arteries before TAVI and immediately after the transcatheter valve implantation maintaining similar hemodynamic conditions (Figure 1). The study was approved by the ethical review board of the University of Verona (ID CESC 2015-498), and all patients eligible for the protocol provided their written consent. Selection of Patients Patients included in the study presented with severe symptomatic AVS defined according to the current European Society of Cardiology (ESC) Guidelines,13 showing at least 1 coronary artery stenosis and having clinical indication to elective TAVI as jointly evaluated by the local Heart Team. No patient had predominant aortic regurgitation. Severe AVS was diagnosed by transthoracic echocardiogram combining the assessment of valve area (<1.0 cm2; indexed valve area <0.6 cm2/m2 body surface area) with flow-dependent indices (mean gradient >40 mm Hg, maximum jet velocity >4.0 m/s, and velocity ratio <0.25).13 Aortic gradients, valvular areas, and left ventricular function were measured before and after valve implantation. Inclusion Criteria 1.Written informed consent 2.Diagnosis of severe AVS with preserved left ventricular function and high transvalvular gradient, with indication to TAVI Exclusion Criteria 1. Lack of informed consent 2. Previous myocardial infarction 3. Previous coronary intervention or tandem lesions in the same coronary artery 4. Contraindication to adenosine administration (eg, severe asthma or chronic obstructive pulmonary disease, heart rate <50 beats/min, and systolic blood pressure <90 mm Hg) 5. Acute presentation of CAD (unstable angina or myocardial infarction) or heart failure 6. Residual aortic regurgitation greater than mild (≥grade 2) after TAVI All TAVI procedures, including hemodynamic and FFR measurements, were performed by the percutaneous transfemoral approach with the use of local anesthesia and mild conscious sedation with low-dose intravenous bolus of fentanyl or midazolam. The choice of the aortic valve prosthesis was left to the operator’s discretion. The Medtronic CoreValve Evolut-R bioprosthesis (Medtronic Inc, Minneapolis, MN) or Edwards Sapien-3 bioprosthesis (Edwards Lifesciences LLC, Irvine, CA) has been used in this study. Coronary Angiography and Quantitative Coronary Analysis Coronary angiography was performed by a standard percutaneous femoral approach with 6F guiding catheters using the same vascular access predisposed for the valve implantation. The severity of the CAD was graded by quantitative coronary analysis (QCA) performed off-line using the software CASS-II QCA package (Pie Medical Imaging, Maastricht, the Netherlands) in a previously validated core laboratory (NBR, Verona, Italy).14 Coronary stenosis were classified after the surgical recommendations for the treatment of CAD in surgical aortic valve repair candidates.2,11 Therefore, arteries showing minimal angiographic lesions with a percent diameter stenosis (%DS) ≤30% were considered angiographically unobstructed; those with a %DS≥30≤50 were classified as having intermediate lesions and those with %DS>50%, as having severe lesions. The contrast-filled catheter was used for calibration. Reference vessel diameter (mm), minimum luminal diameter (mm), %DS, and lesion length were calculated using enddiastolic still-frame images. Pressure Measurements A pressure monitoring guidewire (PrimeWire, Volcano Therapeutics, Rancho Cordova, CA) was advanced distally to the coronary artery stenosis after normalization. Because the continuous intravenous infusion of adenosine in severe AVS may raise hemodynamic concerns, hyperemia was obtained after administration of intracoronary bolus of 150 to 250 mg adenosine as previously indicated by other authors, who reported equivalent diagnostic capabilities.9,10,15,16 The high doses of adenosine bolus were expected to induce effective hyperemia because for clinical reasons nitroglycerin was not administered, given the presence of severe AVS.10 An FFR value ≤0.80 was considered pathological, whereas an FFR value >0.80 was considered negative, that is, unlikely to induce reversible myocardial ischemia according to current recommendations.17 3 Pesarini et al Coronary Assessment With FFR in TAVI Downloaded from http://circinterventions.ahajournals.org/ by guest on May 2, 2017 Figure 1. Case example of the study methods: quantitative coronary analysis and fractional flow reserve (FFR) measurements in a patient with 3-vessel coronary artery disease. Before transcatheter aortic valve implantation baseline analysis shows %DS=62 in the left anterior descending artery (LAD), 46% in the left circumflex coronary artery (LCx), and 75% in the right coronary artery (RCA; A, D, G); 0.014″ pressure guidewire in each corresponding vessel and FFR values 0.86, 0.97, and 0.76 respectively (B, E, H). After valve replacement with a 26-mm Sapien-3 Edwards aortic valve, FFR values decreased to 0.77 in the LAD, 0.89 in the LCx, and 0.57 in the RCA (C, F, I). %DS indicates percent diameter stenosis. Clinical Follow-Up The occurrence of any procedure-related clinical complication was prospectively evaluated. After discharge, patients were contacted at 30 days, as per usual clinical practice to assess the clinical status (New York Heart Association [NYHA] and Canadian Cardiovascular Society [CCS] classes) and the eventual occurrence of major adverse cardiovascular events: death, clinically manifested myocardial infarction, stroke, angina, or the need for hospitalization because of congestive heart failure or chest pain at rest. Statistical Analysis Continuous variables are presented as mean and standard deviation, whereas categorical variables are presented as frequencies (percentages). Correlation among variables was determined by Pearson or Spearman correlation tests as appropriate and expressed as r value. FFR has been classified according to the basal value as positive if the ratio was ≤0.8 or as negative if >0.8. Comparison of variables before and after TAVI was performed using a repeated measures mixed model, with vessel nested within the patient. The TAVI effect was considered as a binary variable (before versus after TAVI). Sensitivity, specificity, diagnostic accuracy, and optimal cutoff value were defined from the calculated receiver operator characteristic curve. The optimal diagnostic cutoff value was defined based on the Youden index. A P value <0.05 was considered statistical significant. All statistical analyses were performed using Stata/SE 14.0 (Stata Corp LP, College Station, TX). Results Patient Population Between January 2015 and June 2016, 57 patients with severe AVS and concomitant CAD underwent TAVI and were included in the study. Fourteen patients received a CoreValve Evolut-R valve, and 43 patients received an Edwards Sapien-3 valve. In 2 patients, a full assessment of the FFR before and after TAVI could not be completed because of difficulties in reengaging the coronary ostia after the valve implantation (1 patient) and a temporary hemodynamic instability related to bleeding (1 patient). In 1 patient, aortic regurgitation of grade 4 Pesarini et al Coronary Assessment With FFR in TAVI >2 was found immediately after valve replacement. These 3 patients have been excluded from this analysis; therefore, coronary angiography and functional assessment before and after TAVI were completed in 54 patients with 133 coronary lesions. Baseline and angiographic characteristic of the overall patient cohort are shown in Table 1. Effect of TAVI on Functional Assessment of Coronary Lesions Downloaded from http://circinterventions.ahajournals.org/ by guest on May 2, 2017 Table 1. Clinical and Angiographic Characteristics of the Studied Cohort Variable Demographic data Age, y 54 80±7.2 Sex male, % 41 Dyslipidemia, % 87 Hypertension, % 80 Smoke, % 48 Diabetes mellitus, % 47 Ejection fraction, % 56±14 Angiographic characteristics Number of lesions 133 Lesion length, mm 12±6 D-Ref, mm 2.9±0.8 MLD, mm 1.8±0.6 DS, % Mean FFR ratio Variables Pre-TAVI Post-TAVI P Value SBP, mm Hg 130±14 135±16 0.08 DBP, mm Hg 74±12 68±14 0.01 HR, bpm 79±9 78±10 0.57 CVP, mm Hg Mean valvular gradient pre-TAVI was 44.1±11 mm Hg, and it dropped to 7.2±5 mm Hg after intervention (P<0.001). The hemodynamic measures remained stable before and after TAVI, as shown in Table 2. TAVI effect has no significant interaction with the overall FFR measurements (z=0.35; P=0.73). In fact, overall FFR values did not change significantly after TAVI compared with the baseline (0.89±0.10 versus 0.89±0.13; Figure 2). When baseline FFR group was included in the model as a binary variable (positive if the ratio was ≤0.8 and negative if >0.8), its interaction with TAVI effect was statistically significant (z=5.54; P<0.0001), indicating a different trend between the 2 groups. Positive FFR values (≤0.8) at baseline were found in 21 of 133(16%) lesions, and in these patients, a significant decrease in the FFR ratio after aortic valve replacement was observed (0.71±0.11 versus 0.66±0.14; Figure 3C). On the contrary, negative FFR values at baseline improved after valve replacement (0.92±0.06 versus 0.93±0.07). Functional FFR variations after TAVI changed the indication to treat coronary stenosis (according to the 0.80 FFR threshold) in 8 of 133 (6%) coronary lesions, that is, 15% of all patients. Seventy-three percent (97/133) of all Number of patients Table 2. Pre- and Postprocedural Hemodynamic and Echocardiographic Characteristics 40±19.7 0.89±0.07 DS% indicates percent diameter stenosis; FFR, fractional flow reserve; and MLD, minimal lumen diameter. 11±3.8 AVA, cm2 0.63±0.11 AVPG mean, mm Hg 44.1±11 AVPG max, mm Hg 68±19.2 11.8±4 0.32 1.84±0.6 <0.001 7.2±5 <0.001 17.4±9.8 <0.001 AVA indicates aortic valve area; AVPG, aortic valve pressure gradient; CVP, central venous pressure; DBP, diastolic blood pressure; HR, heart rate; SBP, systolic blood pressure; and TAVI, transcatheter aortic valve implantation. coronary obstructions were classified as intermediate or severe (%DS>30), and among these, FFR variations across the 0.80 threshold after TAVI occurred in 8% of lesions (8/97). Negative FFR values, intended as >0.80, shifted below the 0.80 threshold in 7 of 112 (6%), whereas only 1 of 21 (5%) positive borderline FFR value (0.79) became negative (0.86) after TAVI. All these cases showed intermediate lesions at QCA (%DS range, 43–63) and similar lesion length (Figure 4). The FFR variations after TAVI stratified by different coronary vessels are shown in Table 3. Because of the low number of lesions in the right coronary artery and in the left circumflex coronary artery, the coronary vessels were classified as left anterior descending (LAD) (n=56) and non-LAD (n=77). When the coronary vessel was added to the model, no significant interaction with TAVI effect was evident (z=0.29; P=0.78), indicating a similar trend between the 2 groups. Mean FFR values in LAD varied from 0.84±0.09 at baseline to 0.83±0.13 after TAVI. In non-LAD coronary arteries, the FFR measurements were 0.92±0.09 before TAVI and 0.92±0.11 after TAVI. Effect of TAVI on Coronary Lesions Stratified by QCA When DS% was included in the model as a categorical variable, its interaction with TAVI had a mild statistical significance (χ2=6.38; P=0.04), indicating a different trend between the groups. The interaction of TAVI effect with FFR values was significant in coronary arteries with %DS≥50 (z=2.31; P=0.02), with a significant worsening of the functional indexes (0.84±0.12 versus 0.82±0.16) after the AVS removal. In coronary arteries with %DS<50, the withdrawal of the afterload obstruction by TAVI caused a relatively small, still constant, improvement of the FFR values both in coronary arteries with a normal angiographic aspect (%DS<30, 0.95±0.05 versus 0.96±0.06) and in the presence of intermediate coronary lesions (%DS=30–50, 0.90±0.07 versus 0.91±0.09). However, the interaction of TAVI effect did not reach statistical significance (z=0.39; P=0.69). Correlation Between FFR and QCA in Patients With AVS The %DS at QCA at baseline showed a significant correlation with the FFR measurements (r=0.58; P<0.0001) and had 5 Pesarini et al Coronary Assessment With FFR in TAVI Figure 2. Left, the overall individual fractional flow reserve (FFR) in aortic valve stenosis patients before and after transcatheter aortic valve implantation (TAVI). The blue lines represent patients with FFR >0.8 at baseline, and the dashed black line shows the average trend of this subgroup. The red lines represent patients with FFR pre-TAVI ≤0.8, and the dashed red line shows their average trend. Right, FFR values before and after TAVI in left anterior descending (LAD), left circumflex coronary artery (LCx), and right coronary artery (RCA). Downloaded from http://circinterventions.ahajournals.org/ by guest on May 2, 2017 a good accuracy (AUC=0.78; 95% confidence interval, 0.70– 0.84; P<0.001) in predicting positive FFR. The best %DS cutoff value to predict a positive FFR at receiver operator characteristic curve analysis was >39% (Youden index=0.53), with a sensibility of 93.7% (95% confidence interval, 69.8–99.8) and a specificity of 60% (95% confidence interval, 49.4–69.8). FFR values in intermediate coronary stenoses (%DS 30–50) located in the proximal LAD did not change significantly after TAVI (0.84±0.05 versus 0.83±0.07). In the study cohort, 57 of 133 (43%) coronary lesions had a %DS≥50 at QCA. Among these, 38 (67%) resulted functionally negative at FFR measurement (FFR>0.8) before TAVI and 3 with borderline baseline FFR values became positive (FFR≤0.8) after TAVI. The remaining 35 of 57 (61%) lesions with %DS≥50 remained FFR negative after aortic valve replacement. Procedural and 30-Day Outcome In no patient, the administration of intracoronary adenosine caused hemodynamic or clinical adverse effects. No clinical complication was observed in relation to the catheterization of the coronary arteries for FFR measurements before and after TAVI. Most importantly, no patient with FFR-positive values at baseline experienced clinical consequences related to the valve positioning procedure (sustained angina or hypotension, myocardial infarction, or heart failure) during the procedure or within the 30 days that followed the intervention, despite Figure 3. Fractional flow reserve (FFR) variations in patients with aortic valve stenosis before and after transcatheter aortic valve implantation (TAVI) of coronary lesions with percent diameter stenosis (%DS) <50 (A) and ≥50 (B) at quantitative coronary analysis (QCA). FFR values pre- and post-TAVI of coronary lesions with %DS≥50% at QCA. FFR values preand post-TAVI of functionally significant coronary lesions (FFR ≤0.8) at baseline (C). Coronary lesions with significant functional stenosis found at post-TAVI FFR and treated with percutaneous coronary intervention (PCI) are presented with the postprocedural FFR controls (D). The dashed black lines show the average trends of each subgroup. 6 Pesarini et al Coronary Assessment With FFR in TAVI Downloaded from http://circinterventions.ahajournals.org/ by guest on May 2, 2017 Figure 4. Subgroup of coronary lesions that crossed through the 0.8 fractional flow reserve (FFR) threshold after transcatheter aortic valve implantation (TAVI). LAD indicates left anterior descending artery; LCx, left circumflex coronary artery; QCA, quantitative coronary analysis; and RCA, right coronary artery. the presence of at least 1 critical coronary stenosis, including the proximal LAD in 6 lesions and the unprotected left main in 1 patient (Figure 5). In 17 (31%) patients, 19 percutaneous coronary interventions (PCIs) were performed during the same TAVI procedure because of FFR values ≤0.8 after the valve replacement (1 unprotected left main, 9 LAD, 5 right coronary artery, and 4 left circumflex coronary artery). In all cases, the PCI was successful, and no complications occurred. In all treated lesions, FFR values normalized after stenting (Figure 3D). The remaining 3 positive lesions located in distal LAD (1 lesion) and in distal right coronary artery (2 lesions) were left on medical therapy because of angiographic complexity, distal location, and advanced age of the patients. In addition, these patients remained asymptomatic during the study period observation. Discussion The main finding of our study is that FFR variations after TAVI performed with the 2 more commonly used types of valves are minor, confirming the validity of FFR in this specific clinical setting. However, significant changes may occur after TAVI in patients with different degrees of CAD. Therefore, FFR values measured after valve replacement may be more accurate to evaluate the need for myocardial revascularization compared with values obtained during preintervention diagnostic examinations. In particular, Table 3. Functional Assessment of Coronary Lesions Stratified by Coronary Segment Pre-TAVI vs Post-TAVI Subset of Patients at Baseline Number of Lesions Pre-TAVI Post-TAVI FFR≤0.8 15 0.72±0.12 0.69±0.13 FFR>0.8 41 0.88±0.12 0.89±0.13 LAD Coronary segment other than LAD FFR≤0.8 6 0.69±0.12 0.62±0.14 FFR>0.8 71 0.94±0.12 0.95±0.13 When the coronary artery (LAD vs non-LAD) was included in the mixedmodel, no significant interaction with TAVI effect was evident (z=0.29; P=0.78), indicating a similar trend between the groups (see text for details). Values are mean±SD. Coronary segments other than LAD include left circumflex coronary artery and right coronary artery. FFR indicates fractional flow reserve; LAD, left anterior descending; and TAVI, transcatheter aortic valve implantation. 7 Pesarini et al Coronary Assessment With FFR in TAVI Downloaded from http://circinterventions.ahajournals.org/ by guest on May 2, 2017 Figure 5. Case example of a significant unprotected left main lesion. At the quantitative coronary analysis, a 57%DS in the left main trunk was evident (A, F). Pressure guidewire was advanced in the left anterior descending (LAD) and left circumflex coronary artery (LCx) before (B, G) and after (D, I) a 29-mm CoreValve Evolute-R implantation. Fractional flow reserve (FFR) values worsened after transcatheter aortic valve implantation both in the LAD (from 0.65 to 0.57; C, E) and in the LCx territory (from 0.66 to 0.62; H, J). %DS indicates percent diameter stenosis. TAVI may unmask functionally significant coronary lesions among angiographically intermediate stenosis because borderline or positive FFR values at baseline decrease significantly after the AVS removal, in particular in the LAD territory. However, in our series that includes also FFR measurements in mild CAD, such functional variations changed the indication to treat the coronary stenosis in a relatively low percentage of lesions (6%). A percentage that rises to 8% when only angiographically intermediate to severe lesions (DS%>30) is considered. Interestingly, in the absence of significant CAD, FFR improved after TAVI in our series, and in angiographically normal arteries, it tended toward normalization. Moreover, our findings support the feasibility and the safety of assessing angiographically and functionally coronary stenosis in patients undergoing TAVI before and after the aortic valve replacement. In fact, no ischemic complication related to the administration of intracoronary adenosine or the use of the pressure wire during the procedure and at 30 days of follow-up was observed, even in patients with angiographically severe lesions with confirmed positive FFR ratios at baseline in the LAD territory. In summary, our findings demonstrate the usefulness of FFR in this clinical setting and suggest that angiographically intermediate lesions may become functionally significant after TAVI, while FFR variations would not affect the diagnostic 8 Pesarini et al Coronary Assessment With FFR in TAVI Downloaded from http://circinterventions.ahajournals.org/ by guest on May 2, 2017 decision based on the 0.80 cutoff in patients at the extremes of the QCA spectrum (unobstructed arteries or severe lesions). Fifty-seven of 133 (43%) coronary lesions presented angiographically significant stenosis (%DS≥50) at QCA, a percentage in agreement with previous observations.1,3 However, the majority of these lesions were functionally negative before (66%) and after TAVI (61%), strongly supporting the need for physiological evaluation before attempting revascularization of lesions incidentally found during a workout AVS examination. Safety and clinical reliability of FFR-guided revascularization in AVS has been recently demonstrated.18 The relationship among QCA, FFR, and inducible myocardial ischemia assessed by imaging or metabolic studies in patients with AVS is unknown. Therefore, the capability of inducing ischemia of the QCA–FFR interaction observed in our patients using the standard 0.80 cutoff cannot be interpreted. Keeping in adherence with current knowledge, the number of functionally guided PCI required in TAVI patients may be quite limited, even in patients with coronary lesions showing %DS≥50 at QCA. This observation is important for the management of TAVI patients in the near future because, by downgrading the severity of CAD, FFR may reduce the need for (useless) myocardial revascularizations in analogy with the observations of the SYNTAX functional study.19 Such a less-invasive approach would make the AVS population even more suitable for transcatheter treatments. Recently, the introduction of TAVI has expanded the opportunity of treating much older and fragile patients that drive significant survival benefit from valve implantation.3,20,21 Few studies have, however, evaluated the impact of CAD on outcomes of patients after TAVI with conflicting results.1 Indeed, unlike CABG at the time of surgical aortic valve repair,22,23 there is no agreement about the real benefit of treating coronary stenosis before or after TAVI in the absence of clear signs of ischemia.24 In a group of 730 consecutive patients who underwent transapical TAVI, a single-stage combined treatment of severe AVS and CAD with PCI has been shown safe and feasible. Early and 3-year survival was comparable with that observed in patients without CAD who received TAVI only.25 Conversely, others analyzed the clinical outcome of 411 TAVIs, 16% of which had significant CAD and received PCI. Incidence of myocardial infarction and 30-day mortality were much higher in the TAVI+PCI group compared with the TAVI alone group (P=0.01). Synchronous versus staged approach for PCI had comparable early mortality (P=1.0).26 The management of CAD in TAVI patients represents an important challenge in the immediate future of transcatheter therapeutics, and the precise identification of the functional significance of coronary stenosis may reveal fundamental for the risk stratification and the safe and effective management of TAVI candidates. This observation may acquire particular importance in view of the expanding indications for TAVI in younger and lower risk patients. From a physiological standpoint, the reduction of the wall stress and the end-diastolic pressure that follows the removal of the left ventricle afterload causes a rapid increase in the coronary flow,27 independent of the presence of CAD in patients with preserved contractile function.28 Recently, wave intensity analysis, derived from simultaneously acquired measures of coronary pressure and velocity using invasive intracoronary wires, has been used to investigate changes in coronary physiology before and after TAVI. Normal coronary perfusion is maintained by coupling between the pressure originating from the proximal (aortic) and the distal (microcirculatory) ends of the coronary circulation.11 At wave intensity analysis, the microcirculatory decompression (suction) was found to decrease and the forward compression wave to increase after TAVI, reflecting the reduction in myocardial work required to eject blood past a stenosed aortic valve and the immediate improvement in the coronary physiological reserve induced by the aortic valve replacement.11,12,29 TAVI, inducing an immediate decrease in hyperemic microvascular resistance and an increase in hyperemic flow velocity, is associated with an immediate improvement in the reserve vasodilator capacity of the coronary microcirculation.10 Increased extravascular compression and reduced diastolic perfusion time, rather than vascular remodeling, influence coronary microvascular dysfunction in AVS. After aortic valve replacement, the improvement in coronary microcirculatory function and the consequent improvement in transmural myocardial perfusion have been related to a combination of reduction in extravascular compressive forces, as well as improved hyperemic diastolic perfusion time.30,31 The pathophysiologic explanations for these changes may be multiple and complex, and their interactions may be involved in the FFR changes after TAVI observed in our study. These, however, go beyond the aims of this observational study and warrant further investigation in dedicated study models. Limitations Given the global complexity of the TAVI patients and the study protocol, the present analysis was conducted on a still limited number of patients, and this may induce some analytic drawbacks. For example, grouping the coronary lesions per coronary segment, our results were not confirmed in vessels other than LAD. Because the coronary obstructions investigated were located in the LAD in a majority of cases (56/133; 42%), it is plausible that the limited sample size influenced the analysis in left circumflex coronary artery and right coronary artery. The general trends are in fact maintained in vessels other than LAD, but larger studies are needed to further investigate the complex crosstalk between QCA and FFR in AVS. Hemodynamic variables, such as the left ventricular filling pressures or the central venous pressure, were not analyzed because, recently, it has been demonstrated that these have no implications in the measurement of FFR while limited within normal values.32 Not administering nitrates in patients with AVS is a limitation to optimal FFR measuring, but this was a request of the reviewers of the study protocol; large doses of adenosine were used in an attempt to optimize hyperemia, however. Conclusions Our findings suggest that FFR measurements are influenced by the presence of AVS. Positive FFR values at baseline will likely decrease further after TAVI, whereas negative FFR 9 Pesarini et al Coronary Assessment With FFR in TAVI values at baseline may not change or tend to improve. Borderline lesions might differ significantly after valve replacement, potentially changing patients’ management in a relatively small percentage of high-risk TAVI procedures. FFR assessment in patients with severe AVS undergoing TAVI is safe, provides reliable information about the functional relevance of coronary lesions, and should be ideally obtained after AVS removal by transcatheter valve implantation. Acknowledgments We thank Dr Luisa Zanolla, from the Biostatistical Department, for her valuable contribution to the statistical analysis of the manuscript. Sources of Funding This study was partially supported by a scholarship grant from Volcano Corp. Downloaded from http://circinterventions.ahajournals.org/ by guest on May 2, 2017 Disclosures None. References 1. Goel SS, Ige M, Tuzcu EM, Ellis SG, Stewart WJ, Svensson LG, Lytle BW, Kapadia SR. Severe aortic stenosis and coronary artery disease– implications for management in the transcatheter aortic valve replacement era: a comprehensive review. J Am Coll Cardiol. 2013;62:1–10. doi: 10.1016/j.jacc.2013.01.096. 2. Bonow RO, Carabello BA, Chatterjee K, de Leon AC Jr, Faxon DP, Freed MD, Gaasch WH, Lytle BW, Nishimura RA, O’Gara PT, O’Rourke RA, Otto CM, Shah PM, Shanewise JS; 2006 Writing Committee Members; American College of Cardiology/American Heart Association Task Force. 2008 Focused update incorporated into the ACC/AHA 2006 guidelines for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 1998 Guidelines for the Management of Patients With Valvular Heart Disease): endorsed by the Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons. Circulation. 2008;118:e523–e661. doi: 10.1161/ CIRCULATIONAHA.108.190748. 3. Leon MB, Smith CR, Mack M, Miller DC, Moses JW, Svensson LG, Tuzcu EM, Webb JG, Fontana GP, Makkar RR, Brown DL, Block PC, Guyton RA, Pichard AD, Bavaria JE, Herrmann HC, Douglas PS, Petersen JL, Akin JJ, Anderson WN, Wang D, Pocock S; PARTNER Trial Investigators. Transcatheter aortic-valve implantation for aortic stenosis in patients who cannot undergo surgery. N Engl J Med. 2010;363:1597– 1607. doi: 10.1056/NEJMoa1008232. 4. Rapp AH, Hillis LD, Lange RA, Cigarroa JE. Prevalence of coronary artery disease in patients with aortic stenosis with and without angina pectoris. Am J Cardiol. 2001;87:1216–1217, A7. 5.Vahanian A, Alfieri O, Andreotti F, Antunes MJ, Barón-Esquivias G, Baumgartner H, Borger MA, Carrel TP, De Bonis M, Evangelista A, Falk V, Iung B, Lancellotti P, Pierard L, Price S, Schäfers HJ, Schuler G, Stepinska J, Swedberg K, Takkenberg J, Von Oppell UO, Windecker S, Zamorano JL, Zembala M; (ESC) and (EACTS) EAfC-TS. Guidelines on the management of valvular heart disease. Eur Heart J. 2012;33:2451–2496. 6. Snow TM, Ludman P, Banya W, DeBelder M, MacCarthy PM, Davies SW, Di Mario C, Moat NE. Management of concomitant coronary artery disease in patients undergoing transcatheter aortic valve implantation: the United Kingdom TAVI Registry. Int J Cardiol. 2015;199:253–260. doi: 10.1016/j.ijcard.2015.06.166. 7. van de Hoef TP, van Lavieren MA, Damman P, Delewi R, Piek MA, Chamuleau SA, Voskuil M, Henriques JP, Koch KT, de Winter RJ, Spaan JA, Siebes M, Tijssen JG, Meuwissen M and Piek JJ. Physiological basis and long-term clinical outcome of discordance between fractional flow reserve and coronary flow velocity reserve in coronary stenoses of intermediate severity. Circ Cardiovasc Interv. 2014;7:301–311. 8. van de Hoef TP, Siebes M, Spaan JA, Piek JJ. Fundamentals in clinical coronary physiology: why coronary flow is more important than coronary pressure. Eur Heart J. 2015;36:3312–3319. 9. van de Hoef TP, Meuwissen M, Escaned J, Davies JE, Siebes M, Spaan JA, Piek JJ. Fractional flow reserve as a surrogate for inducible myocardial ischaemia. Nat Rev Cardiol. 2013;10:439–452. 10.Wiegerinck EM, van de Hoef TP, Rolandi MC, Yong Z, van Kesteren F, Koch KT, Vis MM, de Mol BA, Piek JJ, Baan J Jr. Impact of aortic valve stenosis on coronary hemodynamics and the instantaneous effect of transcatheter aortic valve implantation. Circ Cardiovasc Interv. 2015;8:e002443. doi: 10.1161/CIRCINTERVENTIONS.114.002443. 11. Davies JE, Sen S, Broyd C, Hadjiloizou N, Baksi J, Francis DP, Foale RA, Parker KH, Hughes AD, Chukwuemeka A, Casula R, Malik IS, Mikhail GW, Mayet J. Arterial pulse wave dynamics after percutaneous aortic valve replacement: fall in coronary diastolic suction with increasing heart rate as a basis for angina symptoms in aortic stenosis. Circulation. 2011;124:1565–1572. doi: 10.1161/CIRCULATIONAHA.110.011916. 12.Rolandi MC, Wiegerinck EM, Casadonte L, Yong ZY, Koch KT, Vis M, Piek JJ, Baan J Jr, Spaan JA, Siebes M. Transcatheter replacement of stenotic aortic valve normalizes cardiac-coronary interaction by restoration of systolic coronary flow dynamics as assessed by wave intensity analysis. Circ Cardiovasc Interv. 2016;9:e002356. doi: 10.1161/ CIRCINTERVENTIONS.114.002356. 13. Vahanian A, Baumgartner H, Bax J, Butchart E, Dion R, Filippatos G, Flachskampf F, Hall R, Iung B, Kasprzak J, Nataf P, Tornos P, Torracca L, Wenink A; Task Force on the Management of Valvular Heart Disease of the European Society of Cardiology; ESC Committee for Practice Guidelines. Guidelines on the management of valvular heart disease: the Task Force on the Management of Valvular Heart Disease of the European Society of Cardiology. Eur Heart J. 2007;28:230–268. doi: 10.1093/ eurheartj/ehl428. 14. Ribichini F, Tomai F, De Luca G, Boccuzzi G, Presbitero P, Pesarini G, Ferrero V, Ghini AS, Abukaresh R, Aurigemma C, De Luca L, Zavalloni D, Soregaroli D, Marino P, Garbo R, Zanolla L, Vassanelli C; CEREADES Investigators. Immunosuppressive therapy with oral prednisone to prevent restenosis after PCI. A multicenter randomized trial. Am J Med. 2011;124:434–443. doi: 10.1016/j.amjmed.2010.11.027. 15. De Bruyne B, Gould KL. Standardized hyperemic stress for fractional flow reserve. Circ Cardiovasc Interv. 2013;6:602–603. doi: 10.1161/ CIRCINTERVENTIONS.113.001034. 16.Li J, Elrashidi MY, Flammer AJ, Lennon RJ, Bell MR, Holmes DR, Bresnahan JF, Rihal CS, Lerman LO, Lerman A. Long-term outcomes of fractional flow reserve-guided vs. angiography-guided percutaneous coronary intervention in contemporary practice. Eur Heart J. 2013;34:1375– 1383. doi: 10.1093/eurheartj/eht005. 17.Tonino PA, De Bruyne B, Pijls NH, Siebert U, Ikeno F, van’ t Veer M, Klauss V, Manoharan G, Engstrøm T, Oldroyd KG, Ver Lee PN, MacCarthy PA, Fearon WF; FAME Study Investigators. Fractional flow reserve versus angiography for guiding percutaneous coronary intervention. N Engl J Med. 2009;360:213–224. doi: 10.1056/NEJMoa0807611. 18. Di Gioia G, Pellicano M, Toth GG, Casselman F, Adjedj J, Van Praet F, Ferrara A, Stockman B, Degrieck I, Bartunek J, Trimarco B, Wijns W, De Bruyne B, Barbato E. Fractional flow reserve-guided revascularization in patients with aortic stenosis. Am J Cardiol. 2016;117:1511–1515. doi: 10.1016/j.amjcard.2016.02.023. 19. Nam CW, Mangiacapra F, Entjes R, Chung IS, Sels JW, Tonino PA, De Bruyne B, Pijls NH, Fearon WF; FAME Study Investigators. Functional SYNTAX score for risk assessment in multivessel coronary artery disease. J Am Coll Cardiol. 2011;58:1211–1218. doi: 10.1016/j.jacc.2011.06.020. 20. Smith CR, Leon MB, Mack MJ, Miller DC, Moses JW, Svensson LG, Tuzcu EM, Webb JG, Fontana GP, Makkar RR, Williams M, Dewey T, Kapadia S, Babaliaros V, Thourani VH, Corso P, Pichard AD, Bavaria JE, Herrmann HC, Akin JJ, Anderson WN, Wang D, Pocock SJ; PARTNER Trial Investigators. Transcatheter versus surgical aortic-valve replacement in high-risk patients. N Engl J Med. 2011;364:2187–2198. doi: 10.1056/ NEJMoa1103510. 21.Gurvitch R, Wood DA, Tay EL, Leipsic J, Ye J, Lichtenstein SV, Thompson CR, Carere RG, Wijesinghe N, Nietlispach F, Boone RH, Lauck S, Cheung A, Webb JG. Transcatheter aortic valve implantation: durability of clinical and hemodynamic outcomes beyond 3 years in a large patient cohort. Circulation. 2010;122:1319–1327. doi: 10.1161/ CIRCULATIONAHA.110.948877. 22. Hamm CW, Möllmann H, Holzhey D, Beckmann A, Veit C, Figulla HR, Cremer J, Kuck KH, Lange R, Zahn R, Sack S, Schuler G, Walther T, Beyersdorf F, Böhm M, Heusch G, Funkat AK, Meinertz T, Neumann T, Papoutsis K, Schneider S, Welz A, Mohr FW; GARY-Executive Board. The German Aortic Valve Registry (GARY): in-hospital outcome. Eur Heart J. 2014;35:1588–1598. doi: 10.1093/eurheartj/eht381. 10 Pesarini et al Coronary Assessment With FFR in TAVI Downloaded from http://circinterventions.ahajournals.org/ by guest on May 2, 2017 23.Hannan EL, Wu C, Bennett EV, Carlson RE, Culliford AT, Gold JP, Higgins RS, Smith CR, Jones RH. Risk index for predicting in-hospital mortality for cardiac valve surgery. Ann Thorac Surg. 2007;83:921–929. doi: 10.1016/j.athoracsur.2006.09.051. 24. D’Ascenzo F, Conrotto F, Giordana F, Moretti C, D’Amico M, Salizzoni S, Omedè P, La Torre M, Thomas M, Khawaja Z, Hildick-Smith D, Ussia G, Barbanti M, Tamburino C, Webb J, Schnabel RB, Seiffert M, Wilde S, Treede H, Gasparetto V, Napodano M, Tarantini G, Presbitero P, Mennuni M, Rossi ML, Gasparini M, Biondi Zoccai G, Lupo M, Rinaldi M, Gaita F, Marra S. Mid-term prognostic value of coronary artery disease in patients undergoing transcatheter aortic valve implantation: a meta-analysis of adjusted observational results. Int J Cardiol. 2013;168:2528–2532. doi: 10.1016/j.ijcard.2013.03.062. 25. Penkalla A, Pasic M, Drews T, Buz S, Dreysse S, Kukucka M, Mladenow A, Hetzer R, Unbehaun A. Transcatheter aortic valve implantation combined with elective coronary artery stenting: a simultaneous approach†. Eur J Cardiothorac Surg. 2015;47:1083–1089. doi: 10.1093/ejcts/ezu339. 26.Griese DP, Reents W, Tóth A, Kerber S, Diegeler A, Babin-Ebell J. Concomitant coronary intervention is associated with poorer early and late clinical outcomes in selected elderly patients receiving transcatheter aortic valve implantation. Eur J Cardiothorac Surg. 2014;46:e1–e7. doi: 10.1093/ejcts/ezu187. 27. Ben-Dor I, Malik R, Minha S, Goldstein SA, Wang Z, Magalhaes MA, Weissman G, Okubagzi PG, Torguson R, Lindsay J, Satler LF, Pichard AD, Waksman R. Coronary blood flow in patients with severe aortic stenosis before and after transcatheter aortic valve implantation. Am J Cardiol. 2014;114:1264–1268. doi: 10.1016/j.amjcard.2014.07.054. 28. Banovic MD, Vujisic-Tesic BD, Kujacic VG, Callahan MJ, Nedeljkovic IP, Trifunovic DD, Aleksandric SB, Petrovic MZ, Obradovic SD, Ostojic MC. Coronary flow reserve in patients with aortic stenosis and nonobstructed coronary arteries. Acta Cardiol. 2011;66:743–749. doi: 10.2143/ AC.66.6.2136958. 29. Broyd CJ, Sen S, Mikhail GW, Francis DP, Mayet J, Davies JE. Myocardial ischemia in aortic stenosis: insights from arterial pulse-wave dynamics after percutaneous aortic valve replacement. Trends Cardiovasc Med. 2013;23:185–191. doi: 10.1016/j.tcm.2012.12.001. 30. Rajappan K, Rimoldi OE, Dutka DP, Ariff B, Pennell DJ, Sheridan DJ, Camici PG. Mechanisms of coronary microcirculatory dysfunction in patients with aortic stenosis and angiographically normal coronary arteries. Circulation. 2002;105:470–476. 31. Rajappan K, Rimoldi OE, Camici PG, Bellenger NG, Pennell DJ, Sheridan DJ. Functional changes in coronary microcirculation after valve replacement in patients with aortic stenosis. Circulation. 2003;107:3170–3175. doi: 10.1161/01.CIR.0000074211.28917.31. 32. Toth GG, De Bruyne B, Rusinaru D, Di Gioia G, Bartunek J, Pellicano M, Vanderheyden M, Adjedj J, Wijns W, Pijls NH, Barbato E. Impact of right atrial pressure on fractional flow reserve measurements: comparison of fractional flow reserve and myocardial fractional flow reserve in 1,600 coronary stenoses. JACC Cardiovasc Interv. 2016;9:453–459. doi: 10.1016/j.jcin.2015.11.021. Downloaded from http://circinterventions.ahajournals.org/ by guest on May 2, 2017 Functional Assessment of Coronary Artery Disease in Patients Undergoing Transcatheter Aortic Valve Implantation: Influence of Pressure Overload on the Evaluation of Lesions Severity Gabriele Pesarini, Roberto Scarsini, Carlo Zivelonghi, Anna Piccoli, Alessia Gambaro, Leonardo Gottin, Andrea Rossi, Valeria Ferrero, Corrado Vassanelli and Flavio Ribichini Circ Cardiovasc Interv. 2016;9: doi: 10.1161/CIRCINTERVENTIONS.116.004088 Circulation: Cardiovascular Interventions is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Copyright © 2016 American Heart Association, Inc. All rights reserved. Print ISSN: 1941-7640. Online ISSN: 1941-7632 The online version of this article, along with updated information and services, is located on the World Wide Web at: http://circinterventions.ahajournals.org/content/9/11/e004088 Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in Circulation: Cardiovascular Interventions can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office. Once the online version of the published article for which permission is being requested is located, click Request Permissions in the middle column of the Web page under Services. Further information about this process is available in the Permissions and Rights Question and Answer document. Reprints: Information about reprints can be found online at: http://www.lww.com/reprints Subscriptions: Information about subscribing to Circulation: Cardiovascular Interventions is online at: http://circinterventions.ahajournals.org//subscriptions/