Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
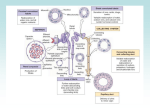
Osmoregulation: Urinary System Maintaining H2O & ion homeostasis Excreting wastes Problems Anatomy of kidney Physiology of nephrons Osmoregulation • Excreting excess – Water and Nitrogenous wastes (N waste = toxic!) – Creatinine – Toxic products (poisons, etc.) – Sugars, salts, organic acids, phosphates, sulfate ions – CO2 • Moves across Transport Epithelium – With or against concentration gradients (ATP dependent) Nitrogenous Waste • By product of metabolic activity – Typically starts as - NH2 (amino) – Combines with H+ to form Ammonia – NH3 • This forms an ammonium ion (NH4+) which is toxic because it interferes with oxidative phosphorylation & therefore, ATP production. – Excreted in a variety of forms – Depends of water availability Urea • Cost: Energetically costly • Benefit: Relatively nontoxic • Can transport in high concentration • Produced in liver • H2O soluble…but we need to conserve water Avenues of H2O loss • Urine: lots of water reclamation occurs in kidneys – Response to increased salt concentrations of extracellular (interstitial fluid) • Sweat: Radiant heat & convective currents evaporate H20 from skin • Exhalation: Lose some moisture, but we do dehumidify air as is passes over mucous membranes of nasal turbinates • Feces: Little lost here Basic Excretion • Blood driven through cell membrane via hydrostatic pressure = filtration • Small stuff crosses, large stuff stays • Selective reabsorptions • Selective additions = secretions • Excretion = “urine” Osmoregulatory organ • Kidney (Cortex, medulla, renal pelvis) ureter, bladder, urethra • Pyramids & nephrons Juxtamedullary & Cortical nephrons • Glomerulus, Bowman’s capsule, proximal tubule, loops of Henle, distal tubule, collecting duct Renal corpuscle structure • Bowman’s capsule: filtration unit – Fenestrated capillaries - pores – Podocytes create filtration slits – Contractile mesangial cells Hydrostatic & Osmotic pressures • • • • Glomerular hydrostatic pressure = 50 Capsular hydrostatic pressure = 15 Osmotic pressure = 25 Net Filtration Pressure NFP = GHP-CsHPOP = 10mm Hg Bridge question • What would happen to filtration rate if GSP increased? If capsular OP increased? • Under what natural conditions do you think GHP might drop? Controlling GFR • Autoregulation – Local contraction or dilation • Hormonal – Renin, Angiotensin, Aldosterone • Autonomic – Angiotensin increases thirst, ADH secretion, systemic BP Increase CO, reduce venous blood reservoir, increase vasoconstriction RAA pathway • Renin, Angiotensin, Aldosterone • Increases blood volume & blood pressure • Stimulus: low BP, measured at glomerulus • Response: JGA releases Renin – Arteriole & precapillary constriction Methods of Reabsorption • Countercurrent multiplier • Carrier-mediated transport – – – – Passive Active Cotransport countertransport Bridge Question • As most reabsorption occurs in the PCT, do you expect those epithelial cells to have any special structure (think of your digestive system)? Why or why not? Secretion & absorption • Countercurrent multiplier – Salt concentration gradient – Huge ATP hog • Active & passive transport of solutes into interstitial fluid • H2O follows • Reabsorb useful ions • Secrete waste, toxins & acidifying ions • Loop some nitrogenous wastes PCT • Reabsorption of useful stuff – H20 – Organic nutrients – Valuable ions • Secretion of excess Loop of Henle • Descending – Passive Reabsorption – H2O: Many aquaporins = passive transport • Ascending - Reabsorption – NaCl, both passive & active – Impermeable to H2O DCT Secretion: K+ , H+, Cl- and NH4+ Reabsorption: HCO3- & Na+ Solute & Urea concentration increase • Urea concentration increases due to impermeability of tubules & ducts Collecting duct • Reabsorption…or not – Transport epithelia adjusts its aquaporin density • Increasing concentration of filtrate ADH • Stimulus: Hypothalamus measures high blood osmolality OR Angiotensin II is present. • Pituitary releases ADH • Binds to PM receptor – Intracellular 2nd messenger cascade • Response: More aquaporin channels produced