Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
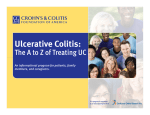
Am J Physiol Gastrointest Liver Physiol 287: G7–G17, 2004; 10.1152/ajpgi.00079.2004. Theme Inflammation and Cancer IV. Colorectal cancer in inflammatory bowel disease: the role of inflammation Steven H. Itzkowitz and Xianyang Yio Gastrointestinal Division, Mount Sinai School of Medicine, New York, New York 10029 multifocal and, once found, marks the entire colon as being at heightened risk of neoplasia, thereby warranting surgical removal of the entire colon and rectum. These differences in morphology and biological behavior not only make clinical cancer surveillance in IBD patients more challenging than in the general population, but they raise the important question of how chronic inflammation contributes to the development of CRC. The “adenoma-carcinoma” sequence found in the sporadic setting becomes the “inflammation-dysplasia-carcinoma” sequence in IBD. The object of this theme article is to first review the clinical and molecular features of CRC in IBD and then discuss how inflammation may contribute to CRC pathogenesis. CLINICAL FEATURES OF COLITIS-ASSOCIATED CRC (IBD), both ulcerative colitis (UC) and Crohn’s colitis, are at increased risk of developing colorectal cancer (CRC). Indeed, IBD ranks among the top three high-risk conditions for CRC, together with the hereditary syndromes of familial adenomatous polyposis (FAP) and hereditary nonpolyposis colorectal cancer (HNPCC). Unlike the latter two conditions that have a well-defined genetic etiology, CRC risk in IBD appears to be related more to chronic inflammation of the gastrointestinal mucosa than to any clear-cut genetic predisposition. Regardless of the underlying condition, essentially all CRCs develop from a dysplastic precursor lesion. In sporadic CRC, the dysplastic precursor is the adenomatous polyp (adenoma), a discrete focus of neoplasia that is typically removed by simple endoscopic polypectomy. In contrast, dysplasia in patients with IBD can be polypoid or flat, localized, diffuse, or Compared with sporadic colorectal carcinoma (SCC), CRC arising in patients with IBD has several distinguishing clinical features. Colitis-associated colorectal cancer (CAC) affects individuals at a younger age than the general population. They more often have a mucinous or signet ring cell histology, there is a higher rate of two or more synchronous primary CRCs, and in some studies, they demonstrate a more proximal distribution in the colon. Curiously, these same features are found in CRCs arising in individuals with HNPCC, although there has been no clear genetic etiology to CAC. A germline hMSH2 mutation (a gene responsible for HNPCC) was reported to be more frequent in UC patients who developed high-grade dysplasia (HGD) and cancer than in those who did not (11), but this has not been substantiated by other investigators (60). The fact that a positive family history of CRC confers a twofold greater risk of developing CRC to the patient with IBD can be viewed as evidence for a genetic etiology, but this same degree of risk attributed to a positive family history of CRC also applies to the general population in whom no clear genetic etiology has yet been elucidated. There must be other factors besides genetic predisposition that contribute to cancer development in IBD. Several lines of evidence implicate chronic inflammation as a key predisposing factor to CRC in IBD (46). First, the risk for developing CRC increases with longer duration of colitis. Although, for some reason, CRC is rarely encountered before seven years of colitis; thereafter, the risk increases at a rate of ⬃0.5–1.0% per year. Second, the extent of colitis is another important risk factor; the more colonic surface that is involved with colitis, the greater the colon cancer risk. Paradoxically, however, patients who have inflammation limited only to the rectum do not have an appreciably increased risk of cancer. Third, the risk of CRC is much greater in the small subset of Address for reprint requests and other correspondence: S. H. Itzkowitz, GI Division, Box 1069, Mount Sinai School of Medicine, One Gustave Levy Place, New York, NY 10029 (E-mail: [email protected]). The costs of publication of this article were defrayed in part by the payment of page charges. The article must therefore be hereby marked “advertisement” in accordance with 18 U.S.C. Section 1734 solely to indicate this fact. inflammatory bowel disease; colorectal cancer; colitis; oxidative stress; animal models PATIENTS WITH INFLAMMATORY BOWEL DISEASE http://www.ajpgi.org 0193-1857/04 $5.00 Copyright © 2004 the American Physiological Society G7 Downloaded from http://ajpgi.physiology.org/ by 10.220.33.5 on June 15, 2017 Itzkowitz, Steven H., and Xianyang Yio. Inflammation and Cancer. IV. Colorectal cancer in inflammatory bowel disease: the role of inflammation. Am J Physiol Gastrointest Liver Physiol 287: G7–G17, 2004; 10.1152/ajpgi.00079.2004.—Patients with ulcerative colitis and Crohn’s disease are at increased risk for developing colorectal cancer. To date, no known genetic basis has been identified to explain colorectal cancer predisposition in these inflammatory bowel diseases. Instead, it is assumed that chronic inflammation is what causes cancer. This is supported by the fact that colon cancer risk increases with longer duration of colitis, greater anatomic extent of colitis, the concomitant presence of other inflammatory manifestations such as primary sclerosing cholangitis, and the fact that certain drugs used to treat inflammation, such as 5-aminosalicylates and steroids, may prevent the development of colorectal cancer. The major carcinogenic pathways that lead to sporadic colorectal cancer, namely chromosomal instability, microsatellite instability, and hypermethylation, also occur in colitis-associated colorectal cancers. Unlike normal colonic mucosa, however, inflamed colonic mucosa demonstrates abnormalities in these molecular pathways even before any histological evidence of dysplasia or cancer. Whereas the reasons for this are unknown, oxidative stress likely plays a role. Reactive oxygen and nitrogen species produced by inflammatory cells can interact with key genes involved in carcinogenic pathways such as p53, DNA mismatch repair genes, and even DNA base excision-repair genes. Other factors such as NF-B and cyclooxygenases may also contribute. Administering agents that cause colitis in healthy rodents or genetically engineered cancer-prone mice accelerates the development of colorectal cancer. Mice genetically prone to inflammatory bowel disease also develop colorectal cancer especially in the presence of bacterial colonization. These observations offer compelling support for the role of inflammation in colon carcinogenesis. Theme G8 ROLE OF INFLAMMATION IN COLITIS-ASSOCIATED COLORECTAL CANCER their products. This will be reviewed below, following a brief overview of the molecular pathogenesis of CAC. MOLECULAR PATHOGENESIS OF SPORADIC CRC To place the molecular pathogenesis of CAC in proper perspective, it is first helpful to appreciate the molecular events involved in the development of SCC. SCC arises as a result of genomic instability. The two main types of genomic instability that contribute to colon carcinogenesis are chromosomal instability (CIN) and microsatellite instability (MSI), accounting for 85 and 15% of SCC, respectively. Chromosomal instability results in abnormal segregation of chromosomes and abnormal DNA content (aneuploidy). As a result, loss of chromosomal material [loss of heterozygosity (LOH)] often occurs, contributing to the loss of function of key tumor suppressor genes such as adenomatous polyposis coli (APC) and p53. These genes can also be rendered nonfunctional by mutation. In either event, it is the accumulation of molecular disturbances mainly in tumor suppressor genes that drives the sporadic adenomacarcinoma progression, and therefore this pathway has sometimes been referred to as the “suppressor pathway.” Colon cancers arising in patients with FAP tend to proceed via this pathway. Loss of APC function is typically an early event in SCC pathogenesis, giving the APC gene the monicker of “gatekeeper” of the colon (Fig. 1). Although some have argued that APC mutation may not be the universal initiating event but may instead occur at somewhat later stages of adenoma progression (48), APC still contributes to the process of CIN (32). During the progression of the adenoma, whereby increases in adenoma size, degree of dysplasia, and degree of villous histology take place, other changes in genetic regulation occur, such as induction of the k-ras oncogene and loss of function of tumor suppressor genes on chromosome 18q in the region of the deleted in colon cancer (DCC) and deleted in pancreatic cancer (DPC4) genes. Loss of p53 gene function occurs late and is believed to be the defining event that drives the adenoma to carcinoma. Fig. 1. Molecular pathogenesis of sporadic colon cancer (top) and colitis-associated colon cancer (bottom). COX-2, cyclooxygenase-2; CIN, chromasomal instability; MSI, microsatellite instability; mut., mutation; LOH, loss of heterozygosity; DCC, deleted in colon cancer; DPC, deleted in pancreatic cancer; APC, adenomatous polyposis coli. AJP-Gastrointest Liver Physiol • VOL 287 • JULY 2004 • www.ajpgi.org Downloaded from http://ajpgi.physiology.org/ by 10.220.33.5 on June 15, 2017 IBD patients who also have primary sclerosing cholangitis, an idiopathic condition characterized by chronic inflammation of the bile ducts, which predisposes not only to CRC but also to biliary tract cancer. Fourth, evidence is mounting to suggest that anti-inflammatory medications, especially 5-aminosalicylates but possibly corticosteroids, can reduce the development of colorectal dysplasia and cancer in IBD. This situation is similar to healthy individuals and even those with FAP, in whom the use of aspirin or other nonsteroidal anti-inflammatory agents has been shown to diminish the growth and subsequent development of colorectal neoplasia. Despite all of the evidence strongly implicating chronic inflammation as the culprit, surprisingly little research has directly addressed the question of whether inflammation per se correlates with CRC risk in IBD. In fact, historically, the degree of colitis activity has been considered not to be an independent risk factor for CRC, probably because of the way that disease activity was defined. For example, when activity of disease was measured according to the frequency of clinical (symptomatic) exacerbations, there did not appear to be a correlation with CRC risk (25, 64). However, when colitis activity has been defined histologically, a recent case-control study found that greater degrees of histologically active inflammation were indeed associated with increased risk of CRC (74). New evidence also indicates that CRC can arise in areas of microscopic colitis proximal to areas of gross colitis, suggesting that histological change, even without colonoscopic alteration, is a better determinant of inflammation for the purposes of cancer risk (54). It is important to realize though, that patients with the most severe inflammation often undergo colectomy early in their disease because they are not responding to medical therapy. As such, they are no longer at risk for developing CRC. Ironically then, many patients who develop CRC in IBD have clinically, as well as histologically, quiescent inflammation. Active inflammation in colorectal mucosa is characterized by a predominant neutrophilic infiltration with crypt abscesses and ulceration of the epithelium. Inactive, or quiescent, inflammation is marked by a predominance of lymphocytes. Thus better insight into the pathogenesis of CAC will likely come from studying the role of the immune cells and Theme ROLE OF INFLAMMATION IN COLITIS-ASSOCIATED COLORECTAL CANCER MOLECULAR PATHOGENESIS OF COLITIS-ASSOCIATED CRC Cancers in the setting of IBD are believed to occur by a progression from no dysplasia to indefinite dysplasia to lowgrade dysplasia (LGD) to HGD to carcinoma (Fig. 1). It is important to realize that in clinical practice, cancers can arise without proceeding through each of these steps (47). Similar to sporadic CRC, colon carcinogenesis in IBD is a consequence of sequential episodes of somatic genetic mutation and clonal expansion. However, unlike SCC, where dysplastic lesions arise in one or two focal areas of the colon, in colitic mucosa, it is not unusual for dysplasia or cancer to be multifocal, reflecting a broader “field change.” Careful mapping studies using DNA aneuploidy as a marker of genomic instability indicate that individual cell populations are observed in the same locations of the colon on repeated colonoscopic examinations and became more widely distributed over time, occupying larger areas of the mucosa (72). Moreover, within an aneuploid area, additional subclones of aneuploidy seem to emerge from their predecessors. Thus genomic instability of increasingly dysregulated subclones of cells with clonal expansion of mutant cell populations occurs at the expense of the normal surrounding epithelium. For the most part, in IBD, neoplastic lesions arise within areas of the mucosa that have been involved with colonic inflammation. It is not known whether the reepithelialization of large patches of colonic mucosa by abnormal clones is simply a consequence of the healing response to ulceration caused by chronic inflammation or whether the epithelial cells of IBD patients have an innate ability to replace surrounding epithelium. Regardless, aneuploidy is often more widespread than dysplasia, and this indicates that substantial genomic alterations can occur in colonic mucosa without disturbing morphology. Perhaps not surprisingly, many of the molecular alterations responsible for SCC development also play a role in colitisassociated colon carcinogenesis. In fact, emerging evidence suggests that in CAC, the frequency of CIN (85%) and MSI (15%) is roughly the same as in SCC (87). Distinguishing features of CAC, however, are differences in the timing and frequency of these alterations (Fig. 1). For example, APC loss of function, considered to be a very common early event in SCC, is much less frequent and usually occurs late in the colitis-associated dysplasia-carcinoma sequence (4, 68, 84). Mutations in APC are rarely, if ever, encountered in colitic mucosa that is negative or indefinite for dysplasia, and fewer than 14% of tissues manifesting LGD or cancer harbor APC mutations (4, 68, 86). Likewise, allelic deletion of APC occurs in fewer than 33% of colitis-associated neoplasms (86). Greater evidence implicates p53 as playing an instrumental role in CAC. Allelic deletion of p53 occurs in ⬃50 – 85% of cancers (13, 89). Indeed, p53 LOH correlates with malignant progression, occurring in 6% of biopsies without dysplasia, 9% with indefinite dysplasia, 33% with LGD, 63% with HGD, and 85% with cancer (13). In the setting of colitis, p53 mutations occur early and are often detected in mucosa that is nondysplastic or only indefinite for dysplasia (10, 13). In carefully mapped colectomy specimens, p53 mutation was an early molecular change that occurred before aneuploidy, which, in turn, preceded p53 LOH (Fig. 1) (10). In fact, a high frequency of p53 mutations was found in inflamed mucosa from UC patients who did not have cancer, indicating that chronic inflammation predisposes to these early mutations (see below) (43). Methylation is assuming increasing importance as a mechanism contributing to the genetic alterations in CAC (Fig. 1). Indeed, methylation of CpG islands in several genes seems to precede dysplasia and is more widespread throughout the AJP-Gastrointest Liver Physiol • VOL 287 • JULY 2004 • www.ajpgi.org Downloaded from http://ajpgi.physiology.org/ by 10.220.33.5 on June 15, 2017 Tumors that arise via the CIN/tumor suppressor gene pathway are typically microsatellite stable (MSS). The remaining 15% of sporadic CRCs arise through the MSI pathway. This pathway is preferred by the vast majority of CRCs that occur in patients with HNPCC. The MSI pathway involves the primary loss of function of genes that usuallly repair DNA base-pair mismatches that occur during the normal process of DNA replication in dividing cells. Although two of these genes, human MutL homolog-1 (hMLH1) and human MutS homolog-2 (hMSH2), are most commonly affected by loss of function in CRC, several other DNA mismatch repair (MMR) genes cooperate to repair DNA base mismatches, and the mutation or loss of any one of them gives rise to DNA replication errors throughout the genome. These errors preferentially affect target genes such as transforming growth factor (TGF)RII, IGF2R, and BAX, which contain in their coding regions short nucleotide repeats that are intrinsically unstable and therefore prone to be copied incorrectly during DNA replication. The resulting microsatellite instability renders these genes incapable of normal colonocyte homeostasis resulting in malignant growth. This pathway of colon carcinogenesis has been referred to as the “mutator” pathway because of the many mutations in key genes involved. Compared with MSS sporadic colon cancers, MSI sporadic colon cancers are more likely to be diploid (normal DNA content), located in the proximal colon, mucinous, poorly differentiated, show lymphocytic infiltration, and associated with a more favorable prognosis (48). MSI-positive CRCs can be further classified into those with high (MSI-H) or low (MSI-L) degrees of MSI depending on how many markers of a consensus panel are found to be unstable (8). Epigenetic alterations also contribute to altered gene expression in colon carcinogenesis. A recently recognized molecular alteration is the CpG island methylator phenotype (CIMP) (85). CpG islands are dense aggregates of cytosine-guanine dinucleotide sequences that may occur in the promoter region of genes. Extensive methylation of the cytosine bases is associated with promoter silencing and loss of gene expression. Many genes involved in cell cycle control, cell adhesion, and DNA repair can be methylated in colon cancer (75). So-called type A methylation, i.e., the estrogen receptor, occurs as a function of age and is found in both normal colon and colon cancer. Type C methylation, however, is cancer associated, leading to pathogenic silencing of genes such as hMLH1, MGMT, p16, and p14. In general, tumors manifest either the CIN or the MSI phenotype. However, there can be overlap between the CIMP and MSI phenotype. For example, hypermethylation of hMLH1 can produce the MSI-H cancer phenotype. By the same token, methylation of MGMT rather than hMLH1 underlies MSI-L cancers (48). The process of methylation is an area of intense investigation, and it is anticipated that this line of research will help to better define the molecular pathways involved in CRC in a variety of clinical settings including IBD. G9 Theme G10 ROLE OF INFLAMMATION IN COLITIS-ASSOCIATED COLORECTAL CANCER mucosa of UC patients (45). In colitis-associated neoplasms, hMLH1 hypermethylation was observed in 6 of 13 (46%) MSI-H, 1 of 6 (16%) MSI-L, and 4 of 27 (15%) MSS specimens, implicating this epigenetic change as a cause of microsatellite instability (31). The cell cycle inhibitor p16INK4a, the loss of which has been implicated in sporadic CRC, is commonly hypermethylated in UC neoplasms (42). Approximately 10% of biopsies without dysplasia already demonstrate p16 promoter hypermethylation, the rate increasing with higher grades of dysplasia and reaching 100% in cancer specimens. p14ARF is an indirect regulator of p53, and it resides at the same locus as p16INK4␣. Loss of p14ARF function by promoter hypermethylation has been reported in 50% of adenocarcinomas, 33% of dysplastic lesions, and even in 60% of mucosal samples without dysplasia from patients with UC (76). Thus the three main molecular pathways of colon carcinogenesis (the APC/tumor suppressor gene/CIN pathway, the MSI pathway, and the CIMP pathway) can all be induced early in the process of CAC, in colitic mucosa before dysplasia develops (Fig. 1). This strongly suggests that inflammation plays a causative role. In addition to the above-mentioned tumor-associated genes that are progressively expressed in the process of CAC carcinogenesis, in UC patients, several inflammation-associated genes such as cyclooxygenase-2 (COX-2) (1), nitric oxide (NO) synthase-2 (NOS)-2 (43), and the interferon-inducible gene 1– 8U (38) are also increased in inflamed mucosa and remain elevated in colonic neoplasms. The central question is how inflammation results in neoplastic transformation and progression. For one thing, the colonic mucosa of patients with IBD demonstrates enhanced epithelial cell turnover. Compared with normal colonic biopsies taken from patients with sporadic adenomas, mucosal biopsies from patients with UC demonstrate higher rates of mitosis as well as apoptosis, especially in areas of active, as opposed to quiescent, inflammation (3). However, whereas increased epithelial cell turnover likely contributes to carcinogenesis, it is insufficient to cause cancer. Rather, in the setting of heightened epithelial cell turnover, mutagenic assault and sustained DNA damage caused by factors within an inflammatory cell-rich microenvironment appear to drive the carcinogenic process. As such, tumors behave similar to wounds that fail to heal (20). A leading theory is that the oxidative stress that accompanies chronic inflammation contributes to neoplastic transformation. Indeed, IBD is considered one of the main “oxyradical overload” diseases whereby chronic inflammation, be it inherited or acquired, results in a cancer-prone phenotype (44). Oxidative stress, with its associated cellular damage, is thought to play a key role in the pathogenesis of the colitis itself as well as in colon carcinogenesis (Fig. 2). Colitis is triggered in a genetically susceptible individual by an environmental insult such as gastrointestinal infection, NSAID use, or other environmental toxins. The inflammatory cells that contribute to the colitis generate reactive oxygen and nitrogen species (RONS). Neutrophils and macrophages, which are important in the acute inflammatory process, generate free radicals and other prooxidant molecules. Inflamed tissues from patients with active UC Fig. 2. Proposed model of how inflammation associated with colitis promotes the development of colonic dysplasia and cancer. or Crohn’s colitis demonstrate increased expression of NOS and other RONS (40, 43, 50, 66). With the use of GAPDH enzyme as a molecular marker, McKenzie et al. (55) showed that oxidation of thiols in the active site of GAPDH, with subsequent inhibition of enzyme activity, occurred in colonic epithelial cells from inflamed mucosa of Crohn’s disease and UC but not from paired samples of unaffected mucosa. Measurements of 8-hydroxydeoxyguanosine (8-OHdG), a mutagen formed by the action of hydroxyl radical at the C8 position of deoxyguanosine DNA base, in mucosal biopsies of patients with UC were reported to be increased in patients with UC compared with normal controls, with levels even higher in UC patients who had dysplasia (23). Interestingly, 8-OHdG levels were increased with longer duration of UC and were lowest in the rectum, suggesting that the meselamine enemas that most of these patients were using might have had an antioxidant effect. Direct support that RONS participate in colonic inflammation comes from interventional studies in animals. Intrarectal administration of peroxynitrite causes colonic inflammation in rats (67). The use of oxygen radical scavengers such as superoxide dismutase, catalase, and NOS inhibitors attenuate colonic inflammation in animal models of chemical-induced colonic injury (78). Likewise, inducible NOS knockout mice (iNOS⫺/⫺) manifest an attenuated colitis in response to injury (41), and in the APCMin/⫹ mouse, which is genetically susceptible to multiple intestinal adenomas, crossing them with iNOS⫺/⫺ mice or treating them with an iNOS inhibitor significantly reduced the prevalence of adenomas (2). Curiously, however, treating APCMin/⫹ mice with 5-ASA did not appreciably reduce adenoma size or number, although treatment with other NSAIDs (piroxicam, sulindac) was effective (70). Although the APCMin/⫹ mouse is not a model of colon cancers that arises in the setting of inflammation, these data still offer insights into mechanisms of colon carcinogenesis. The role AJP-Gastrointest Liver Physiol • VOL 287 • JULY 2004 • www.ajpgi.org Downloaded from http://ajpgi.physiology.org/ by 10.220.33.5 on June 15, 2017 THE ROLE OF CHRONIC INFLAMMATION IN COLON CARCINOGENESIS Theme ROLE OF INFLAMMATION IN COLITIS-ASSOCIATED COLORECTAL CANCER It is not yet clear whether chronic inflammation contributes to this molecular pathway or whether some other factor(s) predisposes. For example, using fluorescent in situ hybridization with probes specific for chromosomes 8, 11, 17, and 18, Rabinovitch et al. (65) reported that patients with UC who had a neoplasm (HGD or cancer) in the colon (so-called progressors) demonstrated CIN both in the neoplastic lesions themselves as well as in nondysplastic rectal mucosa remote from the neoplastic areas. Although normal mucosa from control subjects without UC did not display CIN, inflamed but nondysplastic mucosa of UC patients who did not harbor a neoplasm in their colon (nonprogressors) also did not exhibit CIN. This observation was reinforced by studies in which DNA fingerprinting demonstrated substantial genomic instability in both the dysplastic as well as nondysplastic mucosa of UC patients harboring a neoplasm (16). These findings suggest that widespread genomic instability occurs in patients with UC who develop colonic neoplasia but not in patients with UC who have not yet developed neoplasia despite comparable disease duration and the presence of inflammation. Thus this type of genomic instability may be a marker of cancer risk in UC perhaps apart from the inflammatory process. It has been observed that a possible mechanism to explain the chromosomal instability associated with UC is telomere shortening (63). Given the importance of the CIN pathway in CAC, it will be important to more directly study the role of inflammation in this process. Oxidants can also alter DNA methylation patterns (78). It is not yet known whether the hypermethylation of genes involved in CAC (45) are affected by oxidant injury. In addition to damaging DNA and other macromolecules, oxyradicals can also induce key genes involved in the inflammatory and carcinogenic process. For example, the transcription factor NF-B can stimulate iNOS to generate NO and COX-2 to generate prostanoids that have proinflammatory and carcinogenic effects (88). Activated NF-kB is found in inflamed mucosal biopsies of patients with IBD (71). Among the factors that can regulate NF-kB activity, TNF-␣ induces NFkB, whereas peroxisome proliferator-activated receptor-␥ (PPAR␥) attenuates NF-kB. At the present time, it is not clear whether TNF-␣ itself plays a role in carcinogenesis nor is it known whether inhibiting TNF-␣, which is so effective in reducing the inflammation of Crohn’s disease, can abrogate the carcinogenic process. PPAR␥ ligands have been shown to inhibit intestinal inflammation (83), and impaired expression of PPAR␥ has been described in colonic epithelial cells of patients with UC (24). Treatment of APC deficient mice with PPAR␥ ligands has yielded mixed results, with both increases and decreases in adenoma growth reported (12, 58). The role of PPAR␥ in colitis-associated cancer has not been investigated. COX-2 activity plays an important role in sporadic carcinogenesis where it has been shown that normal colonic mucosa does not express COX-2, but with the adenoma-carcinoma sequence, this enzyme is induced. Among the many effects of cyclooxygenases, they can activate procarcinogens, indirectly produce free radicals, and promote angiogenesis (81). In animal models, COX-2 inhibition can dramatically reduce the development of colon cancers, just as in humans, use of COX-2 inhibitors and other NSAIDs is protective against colon cancer (34). In UC, COX-2 expression is somewhat enhanced in inflamed mucosa, but it is further induced in dysplastic and AJP-Gastrointest Liver Physiol • VOL 287 • JULY 2004 • www.ajpgi.org Downloaded from http://ajpgi.physiology.org/ by 10.220.33.5 on June 15, 2017 played by the NO/iNOS system in both colonic inflammation and tumor development is quite complex and does not permit simple conclusions or extrapolation to the issue of carcinogenesis in UC at the present time (6, 22). The fact that mice deficient in glutathione peroxidase enzymes develop inflammation and cancer of the small and large intestine further supports the notion that antioxidant pathways are important for preventing the inflammation-neoplasia sequence (17). How then might oxidative stress contribute to colorectal carcinogenesis? Free radicals have the potential to affect a large array of metabolic processes, because their targets include DNA, RNA, proteins, and lipids (44, 53). If key genes or proteins responsible for colonocyte homeostasis are targeted, dysplasia and subsequent carcinoma arise. The p53 tumor suppressor gene is one important target. Hussain et al. (43) examined the mutation spectrum of p53 at codons 247 and 248 in biopsies taken from inflamed colonic mucosa of UC patients compared with normal, non-UC controls. They noted that more than half of the UC cases exhibited a higher frequency of G-to-A transitions at the CpG site of codon 248 and C-to-T transitions at the third base of codon 247 compared with controls. Moreover, in paired biopsies from UC patients, this pattern of mutation was only seen in inflamed rather than noninflamed mucosa. Increased NOS-2 activity was associated with these p53 mutations, suggesting that oxidative stress was playing a role. These investigators also observed that increases in posttranslational modifications of p53 were associated with increased iNOS activity in inflamed tissues from UC patients, further implicating activated p53 in response to oxidant injury (40). More direct evidence for the role of RONS in colon carcinogenesis comes from the work of Gasche et al. (33), who used model colon cancer cell lines to observe that hydrogen peroxide (H2O2) produced frameshift mutations in a reporter gene. In their system, cells that were genetically deficient in DNA MMR activity were particularly susceptible to frameshift mutations, but even at higher concentrations of H2O2, cells with normal MMR activity displayed frameshift mutations. In subsequent studies, these investigators found that H2O2 inactivated the DNA MMR system, apparently by damaging the protein complexes responsible for DNA base mismatch repair (15). Conceivably therefore, even in the absence of mutations of the relevant genes, oxidative stress may put enough “pressure” on the DNA MMR system to create microsatellite instability, and this presumably contributes to the MSI phenotype seen both in nonneoplastic and in neoplastic mucosa of UC patients. A recent discovery suggests that increased activity of enzymes responsible for the process of base excision-repair might also contribute to MSI in UC tissues (39). MSI can be detected in chronically inflamed mucosa from UC patients, even in those with rather short disease duration before the risk of neoplasia ostensibly rises (9). This lends credence to the concept that inflammation alone can cause MSI. Curiously, however, MSI is not found in normal colonic mucosa from healthy controls or from patients with other types of benign inflammatory colitis including Crohn’s colitis (9, 59). It is tempting to speculate that certain RONS may cause MSI and that the spectrum of RONS differs in the local tissue microenvironment depending on the inflammatory background of the underlying disease. As mentioned above, chromosomal instability represents the major pathway by which cancers seem to arise in IBD patients. G11 Theme G12 ROLE OF INFLAMMATION IN COLITIS-ASSOCIATED COLORECTAL CANCER cancerous lesions (1). Whether COX-2 inhibition would be chemopreventive against CRC in the setting of UC is not known. Concern has been raised by a study in the IL-10deficient mouse model of chronic colitis, where COX-2 inhibitors paradoxically enhanced the frequency of colonic dysplasia (see below) (35). among mice receiving only one or two cycles of DSS was 22 and 40%, respectively. Likewise, DSS induced a very high frequency of dysplasia that arose in areas of healed mucosa as well as those of acute and chronic inflammation. Animals with higher inflammation scores had significantly more dysplastic lesions. Thus colitis markedly accelerates the development of neoplasia in APC mutant mice. LESSONS FROM ANIMAL MODELS DSS COLITIS IN HEALTHY RODENTS Dysplasia and cancer can be induced in healthy mice or rats when colitis is induced by repeated cycles (19, 52, 61) or rarely after a single cycle (19) of DSS. In this model, longer disease duration (3– 6 mo) was associated with an increased rate of neoplasia, even in mice given the identical initial colitis insult and in the setting of clinical remission (19). The localization of dysplasia and/or cancer is ⬃20, 44, and 36% for the proximal, middle, and distal colon, respectively (19). Animals that developed neoplasia demonstrated more severe degrees of inflammation, especially in the distal colon (19, 61). The histology of dysplastic and cancerous lesions resembles that of IBD neoplasms, but in contrast to the human situation, none of the cancers and only 7% of dysplasias induced by DSS manifested nuclear p53 immunostaining (19). Parenthetically, in the DSS model, treatment with the antioxidant N-acetylcysteine reduced both the inflammation and tumor incidence (77). In general, these observations support the concept that prolonged and repetitive inflammation promotes colon cancer. DSS COLITIS IN CANCER-PRONE MICE The induction of chronic inflammation by DSS results in more frequent development of cancer and dysplasia in mice prone to MSI (51). For example, 28/30 MSH2⫺/⫺ mice developed dysplasia or cancer in response to DSS, and the frequency of HGD was 47, 23, and 8% for MSH2⫺/⫺, MSH2⫹/⫺, and MSH2⫹/⫹, respectively. Perhaps not surprisingly, 89% of colonic dysplasias or cancers from MSH2⫺/⫺ mice were MSI positive, whereas the majority of neoplasms arising in DSStreated heterozygotes or wild-type mice developed independently of the mismatch repair system, because very little MSI was found in these groups. The inflamed and uninflamed colonic mucosa remote from dysplastic lesions in the MSH2⫺/⫺ mice also demonstrated MSI, implying that, similar to humans, MSI is induced by colonic inflammation and can precede dysplasia. The APCMin/⫹ mouse has also been studied in the context of DSS-induced colitis (18). No cancers arose in APCMin/⫹ mice that did not receive DSS. In contrast, the frequency of cancers CANCER AND DYSPLASIA IN IBD-PRONE MICE Of greater relevance to human CAC, the genetically engineered immunodeficient mice have provided new insights into aspects of the inflammatory response that may be responsible for instigating neoplastic progression (Table 1). IL-2-Deficient, IL-2, and 2-Microglobulin Double Knockout Mice IL-2 is an essential regulatory cytokine of the immune system. Among IL-2-deficient mice, 50% die within 9 wk with splenomegaly, lymphadenopathy, and severe autoimmune hemolytic anemia (37). The rest develop chronic colitis resembling UC and a systemic wasting disease resulting in death within 6 mo. Within the limited lifespan, dysplasia (37) but not cancers (80) has been observed. The IL-2null and 2-Mnull double knockout mouse develops pancolitis similar to IL-2 knockout mice, but these mice have milder overall disease and are able to survive ⬎6 mo. This offers an opportunity to study colon carcinogenesis. With prolonged observation (6 –12 mo), 32% of these mice develop adenocarcinoma in the proximal colon. In addition, LGD and HGD are also noted in these animals (80). Molecular characterization of these cancers revealed that all of the cancers harbored APC gene mutations, more than one-half had p53 gene mutations, and most exhibited MSI (80). IL-10 KNOCKOUT MICE When the IL-10 gene is disrupted, mice develop spontaneous generalized enterocolitis under conventional conditions. Specific pathogen-free (SPF) housing conditions reduce the severity and limit the disease to the proximal colon (7). The development of colitis in these mice is dependent on IL-12 and requires the presence of enteric bacteria (57). Under SPF conditions, 100% of the mice develop colitis after 3 mo of age. After 3 and 6 mo, 25 and 60% of the mice, respectively, develop adenocarcinoma. Cancers arise mainly in the proximal colon, and they often express COX-2 in regions containing inflammatory cells and myofibroblasts (79). Ironically, these cancers do not seem to manifest alterations of APC, p53, K-ras, or Msh2 genes, and although circulating TGF- levels are elevated, there does not appear to be any downregulation or truncation of the TGF- receptor type II (82). Thus the molecular mechanism of these tumors remains elusive. IL-10 treatment was shown to ameliorate the colitis in all animals and decreased the cancer occurrence by half even after the colitis had been established (7). Likewise, in a small study (62), probiotics also reduced the prevalence of colon cancer and mucosal inflammatory activity. On the other hand, pure cultures of Enterococcus faecalis induced both IBD and, after 20 wk, dysplasia and cancer of the rectum in IL-10⫺/⫺ mice (5). Paradoxically, COX-2 inhibitors have been shown to exacerbate, rather than ameliorate, the severity of colitis and the AJP-Gastrointest Liver Physiol • VOL 287 • JULY 2004 • www.ajpgi.org Downloaded from http://ajpgi.physiology.org/ by 10.220.33.5 on June 15, 2017 To help better understand the role of inflammation in vivo, investigators have turned to animal models, and indeed, the existing data suggest that inflammation predisposes to colorectal cancer. Three main approaches have been used: 1) inducing inflammation with injurious agents such as dextran sulfate sodium (DSS) in otherwise healthy rodents and monitoring for the development of neoplasia; 2) inducing inflammation in mice with a genetic predisposition to colon cancer; and 3) studying mice with a genetic predisposition to inflammatory bowel disease for the development of neoplasia. Of the three approaches, the latter is the most physiologically relevant to human disease. Theme G13 ROLE OF INFLAMMATION IN COLITIS-ASSOCIATED COLORECTAL CANCER Table 1. Summary of colorectal neoplasia in genetically engineered IBD animal models Knockout Mouse (Ref) Background Strain Inflammation Tumor Location Tumor Histology C57BL/6 ⫻ 129 UC-like Carcinoma (32%) IL-10 KO (7) C57BL/6 ⫻ 129 Colitis with some features of Crohn’s, duodenitis Carcinoma (60%) Rag2 KO (28,29) 129/SvEv Induced by infecting with Helicobacter hepaticus dysplasia, tubular adenoma, carcinoma in situ, adenocarcinoma (100%) Cecum Colon Rag2/Tgf1 DKO (27) 129S6 ⫻ CF1 Colitis Cecum Colon TCR/p53 DKO (49) C57BL/6jjcl UC-like Gpx1/Gpx2 DKO (17) Mixed C57BL/6J and 129Sv/J or 129S3 Ileocolitis N-cadherin dominant negative (36) 129/Sv3B6 Crohn’s-like Dysplasia, adenocarcinoma (100%) Dysplasia, adenocarcinoma (70%) Dysplasia, adenocarcinoma (28%); signet ring cell carcinoma Adenomas, not cancer G␣i2 KO (73) 129/Sv UC-like Carcinoma (31%) Rectum Colon Colon Rectum Ileocecum Cecum Ileum Colon Small bowel Colon Spontaneous development of colitis and carcinoma Colitis induced by normal flora; colitis and cancer caused by Enterococcus faecalis 1. Both colitis and neoplasm are induced by H. hepaticus. 2. CD4⫹ CD45RBlo (IL-10) prevents colitis and cancer. Require H. hepaticus to induce inflammation and neoplasms Normal flora is required to produce inflammation and tumors Require bacterial flora, including Helicobacter species Chimeric mouse; adenomas form in inflamed and noninflamed areas. Colitis and cancer occur even in SPF barrier facility. KO, knockout; DKO, double knockout; IBD, inflammatory bowel disease; UC, ulcerative colitis; GPx, glutathione peroxidase; TCR, T cell receptor; SPF, specific-pathogen free. frequency of dysplasia in IL-10⫺/⫺ mice (35). The effect of IL-10 in IBD has also been studied in other colitis models (57). In SCID mice, transfer of CD4⫹CD45RBhi T cells from normal donors into CB-17 SCID mice resulted in severe colitis. IL-10 has been shown to prevent colitis in this setting. Oral administration of Lactococcus lactis-secreting IL-10 reduced DSS-induced colitis. Taken together, it appears that IL-10 plays an inhibitory/regulatory role in these animal models and that lacking IL-10 resulted in colitis. The chronic inflammation further contributed to the formation of adenocarcinoma. RAG2-DEFICIENT MICE Rag2-deficient mice lack functional T and B lymphocytes because of an inability to properly rearrange antigen receptors. This mouse has been a valuable model to study the function of various subsets of lymphocytes by transferring specific lymphocytes from immunocompetent mice. Colitis can be induced in this mouse by adoptive transfer of CD4⫹CD45RBhi T cells. This colitis is preventable by cotransfer of CD4⫹CD25⫹ or CD4⫹CD45RBlo regulatory T cells. The latter subset of T cells is believed to harbor regulatory cells that inhibit intestinal inflammation. In this animal, significant colitis may also be induced by infection with a widespread enteric mouse bacterial pathogen, Helicobacter hepaticus, in the absence of T cells (28). Interestingly, after the infection, these mice not only contract colitis, but also inevitably develop colonic tumors, including sessile tubular adenoma, dysplasia, carcinoma in situ, and adenocarcinoma (100%) (28). However, they do not produce pedunculated or villous adenomas. In contrast, if they are maintained in a H. hepaticus-free environment, these ani- mals do not have colon tumors or colitis. Adoptive transfer of CD4⫹CD45RBlo regulatory T cells to these mice significantly suppressed colitis. After the regulatory T cell transfer, the majority of animals had minimal or no colitis and did not develop neoplasia; neoplasia was found in those animals that developed moderate to severe local colitis. It is believed that IL-10 produced by these regulatory T cell is pivotal in inhibiting inflammation and interrupting carcinogenesis, because transferring IL-10-deficient CD4⫹CD45RBlo regulatory cells did not protect these animals from colitis and carcinoma (29). This model provides further evidence supporting IL-10 as a protective agent against colitis and that there is a link between chronic colitis and the formation of colonic neoplasms. Alternatively, IL-10 may be able to inhibit or arrest carcinogenesis via a T cell-independent mechanism, because administration of IL-10 has been shown to suppress cancers in SCID mice (57). TGF-1 AND RAG2 DOUBLE KNOCKOUT MICE Tgfb1⫺/⫺ mice develop an autoimmune disease with inflammatory lesions in multiple organs. Crossing these mice with Rag2 knockout mice rescues them from the autoimmune phenotype and permits them to live as long as 8 mo. They develop hyperplasia of the cecum and colon, with a primarily granulocytic inflammation of the submucosa. This model shares similarity with Rag2-deficient mice, including the location of colitis, the universal development of both dysplasia and adenocarcinoma, and the requirement of H. hepaticus for the induction of colitis and colon tumors (26 –29). The most significant difference, perhaps, is the genetic background of these two models. In this model, colitis is required but is not AJP-Gastrointest Liver Physiol • VOL 287 • JULY 2004 • www.ajpgi.org Downloaded from http://ajpgi.physiology.org/ by 10.220.33.5 on June 15, 2017 IL-2/2M DKO (80) Comments Theme G14 ROLE OF INFLAMMATION IN COLITIS-ASSOCIATED COLORECTAL CANCER sufficient for cancer formation; a genetic predisposition to cancer appears to contribute. Whether the enteric bacteria directly affect carcinogenesis or induce inflammation that results in neoplastic events is unclear. The cancers in this model do not demonstrate MSI. T CELL RECEPTOR- KNOCKOUT MICE GLUTATHIONE PEROXIDASE-1/-2 DOUBLE KNOCKOUT MICE Glutathione peroxidases (GPX) are a family of intracellular antioxidant enzymes that reduce H2O2 and organic hydroperoxides by oxidizing glutathione. Mice with targeted disruption of both Gpx1 and Gpx2 develop ileocolitis between 2 and 7 wk of age. After 4 mo of age, ⬃40% of animals develop tumors (28% adenocarcinomas) that are often nonpolypoid and primarily located in the distal ileum (17). Higher tumor rates were correlated with higher inflammation scores in the ileum but not the colon, suggesting that inflammation is necessary but not sufficient to cause tumors. Tumor incidence was highest in colonies that were raised in non-SPF conditions. Essentially no tumors developed in germ-free or SPF colonies nor were there any tumors noted in animals that had at least one wild-type Gpx1 or Gpx2 allele. This model is instructive, because these mice have otherwise intact immune systems and mucosal barrier function, and it highlights the importance of the antioxidant system in protecting against inflammation and neoplasia in the setting of bacterial infection. N-CADHERIN DOMINANT-NEGATIVE MICE These mice are immunologically intact but have a defect in their intestinal mucosal barrier. Cadherins are essential for mediating cell adhesion and normal development. Expression of a dominant-negative form of N-cadherin lacking extracellular domain (NCAD⌬) resulted in loss of endogenous Ecadherin from the cell surface. Because complete disruption of cadherin production results in embryonic lethality in mice, a chimeric mouse model was created that expressed dominantnegative N-cadherin in the small intestine (36). This was generated by introducing genetically manipulated embryonic stem cells from 129/Sv strain (NCAD⌬) into normal B6 blastocytes. The resultant 129/Sv3 B6 chimeric mouse intestine contained patches of 129/Sv (NCAD⌬)-derived cryptvillus units and patches of crypt-villus units of B6 background that were easily distinguishable from 129/Sv by their lectinbinding properties. All chimeric mice developed IBD similar to Crohn’s disease, presumably because disruption of the epithelial barrier results in inflammation. Inflammation is present only in 129/Sv (NCAD⌬) patches but not in B6 epithelium, and consequently, foci of dysplasia and adenoma were only found in 129/Sv (NCAD⌬) areas. No adenocarcinomas were observed during the 19 mo of the experiment. This model supports the association between inflammation and tumorogen- G␣i2ⴚ/ⴚ MICE Mice deficient in the G protein subunit ␣i2 develop profound alterations in thymocyte maturation and function (73). From 13 wk of age onward, these mice develop severely active colitis, especially in the distal colon, and the intensity and extent of colitis progress with age. By 15–36 wk of age, 31% of mice developed cancer that was not polypoid or metastatic. Large pools of mucin were found in some cancers. FUTURE DIRECTIONS Chemoprevention of CRC is an area of great interest and intense investigation. Just as aspirin and NSAIDs appear to prevent CRC in the general population, evidence is accumulating that 5-aminosalicylic acid (5-ASA) compounds may prevent colorectal neoplasia in patients with UC (21). Whereas the mechanism of this is not known, it has been shown experimentally that 5-ASA is able to prevent damage to GAPDH caused by exposure to hypochlorite, the most potent oxidant produced by neutrophils (56). This ability of 5-ASA to scavenge RONS was not shared by other medications used to treat IBD such as methylprednisolone, 6-mercaptopurine, or metronidazaole (56). Rectal administration of 5-ASA in patients without IBD has been shown to induce apoptosis selectively in tumor cells but not in nearby normal epithelial cells (14). The chemopreventive role of 5-ASA in IBD deserves further study in humans and in animal models. In addition, given the importance of prooxidants in causing molecular damage to colonic epithelium, further investigating the potential role of antioxidants as chemopreventive agents is also worthwhile. Moreover, more work is needed to identify the molecular underpinnings of how inflammation might contribute to chromosomal instability and abnormal methylation of genes. Another area of interest is the role of bacteria in causing cancer. Although an infectious origin to human CRC is not usually considered, recent data suggest that polyoma virus infection can cause CIN in human colonic epithelial cells (69). Whether bacteria can also cause CRC in humans, analogous to H. pylori causing gastric cancer, is not known. Because several of the animal models of CRC in IBD implicate bacteria in the pathogenesis of both the inflammation and cancer, insights from these studies, in addition to asking why some colitis models do not get CRC, may provide further food for thought. Finally, to date, researchers in the field of CAC have typically drawn insights from the work performed on SCC. Curiously, a recent study (30) showing elevated C-reactive protein levels in individuals who were prone to sporadic CRC suggests that inflammation may play more of a role in SCC than previously appreciated. So, just as understanding the uncommon conditions FAP and HNPCC have taught us about the pathogenesis of SCC, lessons learned from IBD as a model of colonic inflammation might also help us further our knowledge about how inflammation might cause CRC in general. REFERENCES AJP-Gastrointest Liver Physiol • VOL 1. Agoff SN, Brentnall TA, Crispin DA, Taylor SL, Raaka S, Haggitt RC, Reed MW, Afonina IA, Rabinovitch PS, Stevens AC, Feng Z, and 287 • JULY 2004 • www.ajpgi.org Downloaded from http://ajpgi.physiology.org/ by 10.220.33.5 on June 15, 2017 T cell receptor (TCR)--deficient mice have defective intestinal mucosal immune systems and develop UC-like colitis. When raised under conventional conditions, TCR- and p53 double knockout mice are not only susceptible to chronic inflammation (90%, most limited to ileocecum and cecum) but are also prone to dysplasia (50 –70%) and adenocarcinoma (70%) (49). Germ-free conditions prevent both chronic inflammation and neoplasms. esis. However, the fact that adenomas occurred in both inflamed and noninflamed 129/Sv (NCAD⌬) patches indicates that a noninflammatory-driven process, such as aberrant cell migration, may also play a role. Theme ROLE OF INFLAMMATION IN COLITIS-ASSOCIATED COLORECTAL CANCER 2. 3. 4. 5. 6. 8. 9. 10. 11. 12. 13. 14. 15. 16. 17. 18. 19. 20. Coussens LM and Werb Z. Inflammation and cancer. Nature 420: 860 – 867, 2002. 21. Croog VJ, Ullman TA, and Itzkowitz SH. Chemoprevention of colorectal cancer in ulcerative colitis. Int J Colorectal Dis 18: 392– 400, 2003. 22. Crowell JA, Steele VE, Sigman CC, and Fay JR. Is inducible nitric oxide synthase a target for chemoprevention? Mol Cancer Ther 2: 815– 823, 2003. 23. D’Inca R, Cardin R, Benazzato L, Angriman I, Martines D, and Sturniolo GC. Oxidative DNA damage in the mucosa of ulcerative colitis increases with disease duration and dysplasia. Inflamm Bowel Dis 10: 23–27, 2004. 24. Dubuquoy L, Jansson EA, Deeb S, Rakotobe S, Karoui M, Colombel JF, Auwerx J, Pettersson S, and Desreumaux P. Impaired expression of peroxisome proliferator-activated receptor ␥ in ulcerative colitis. Gastroenterology 124: 1265–1276, 2003. 25. Eaden J, Abrams K, Ekbom A, Jackson E, and Mayberry J. Colorectal cancer prevention in ulcerative colitis: a case-control study. Aliment Pharmacol Ther 14: 145–153, 2000. 26. Engle SJ, Hoying JB, Boivin GP, Ormsby I, Gartside PS, and Doetschman T. Transforming growth factor 1 suppresses nonmetastatic colon cancer at an early stage of tumorigenesis. Cancer Res 59: 3379 – 3386, 1999. 27. Engle SJ, Ormsby I, Pawlowski S, Boivin GP, Croft J, Balish E, and Doetschman T. Elimination of colon cancer in germ-free transforming growth factor 1-deficient mice. Cancer Res 62: 6362– 6326, 2002. 28. Erdman SE, Poutahidis T, Tomczak M, Rogers AB, Cormier K, Plank B, Horwitz BH, and Fox JG. CD4⫹ CD25⫹ regulatory T lymphocytes inhibit microbially induced colon cancer in Rag2-deficient mice. Am J Pathol 162: 691–702, 2003. 29. Erdman SE, Rao VP, Poutahidis T, Ihrig MM, Ge Z, Feng Y, Tomczak M, Rogers AB, Horwitz BH, and Fox JG. CD4⫹CD25⫹ regulatory lymphocytes require interleukin 10 to interrupt colon carcinogenesis in mice. Cancer Res 63: 6042– 6250, 2003. 30. Erlinger TP, Platz EA, Rifai N, and Helzlsouer KJ. C-reactive protein and the risk of incident colorectal cancer. JAMA 291: 585–590, 2004. 31. Fleisher AS, Esteller M, Harpaz N, Leytin A, Rashid A, Xu Y, Liang J, Stine OC, Yin J, Zou TT, Abraham JM, Kong D, Wilson KT, James SP, Herman JG, and Meltzer SJ. Microsatellite instability in inflammatory bowel disease-associated neoplastic lesions is associated with hypermethylation and diminished expression of the DNA mismatch repair gene, hMLH1. Cancer Res 60: 4864 – 4868, 2000. 32. Fodde R, Kuipers J, Rosenberg C, Smits R, Kielman M, Gaspar C, van Es JH, Breukel C, Wiegant J, Giles RH, and Clevers H. Mutations in the APC tumour suppressor gene cause chromosomal instability. Nat Cell Biol 3: 433– 438, 2001. 33. Gasche C, Chang CL, Rhees J, Goel A, and Boland CR. Oxidative stress increases frameshift mutations in human colorectal cancer cells. Cancer Res 61: 7444 –7448, 2001. 34. Gupta RA, DuBois RN, and Wallace MC. New avenues for the prevention of colorectal cancer: targeting cyclo-oxygenase-2 activity. Best Pract Res Clin Gastroenterol 16: 945–956, 2002. 35. Hegazi RA, Mady HH, Melhem MF, Sepulveda AR, Mohi M, and Kandil HM. Celecoxib and rofecoxib potentiate chronic colitis and premalignant changes in interleukin 10 knockout mice. Inflamm Bowel Dis 9: 230 –236, 2003. 36. Hermiston ML and Gordon JI. Inflammatory bowel disease and adenomas in mice expressing a dominant negative N-cadherin. Science 270: 1203–1207, 1995. 37. Hibi T, Ogata H, and Sakuraba A. Animal models of inflammatory bowel disease. J Gastroenterol 37: 409 – 417, 2002. 38. Hisamatsu T, Watanabe M, Ogata H, Ezaki T, Hozawa S, Ishii H, Kanai T, and Hibi T. Interferon-inducible gene family 1– 8U expression in colitis-associated colon cancer and severely inflamed mucosa in ulcerative colitis. Cancer Res 59: 5927–5931, 1999. 39. Hofseth LJ, Khan MA, Ambrose M, Nikolayeva O, Xu-Welliver M, Kartalou M, Hussain SP, Roth RB, Zhou X, Mechanic LE, Zurer I, Rotter V, Samson LD, and Harris CC. The adaptive imbalance in base excision-repair enzymes generates microsatellite instability in chronic inflammation. J Clin Invest 112: 1887–1894, 2003. 40. Hofseth LJ, Saito S, Hussain SP, Espey MG, Miranda KM, Araki Y, Jhappan C, Higashimoto Y, He P, Linke SP, Quezado MM, Zurer I, Rotter V, Wink DA, Appella E, and Harris CC. Nitric oxide-induced cellular stress and p53 activation in chronic inflammation. Proc Natl Acad Sci USA 100: 143–148, 2003. AJP-Gastrointest Liver Physiol • VOL 287 • JULY 2004 • www.ajpgi.org Downloaded from http://ajpgi.physiology.org/ by 10.220.33.5 on June 15, 2017 7. Bronner MP. The role of cyclooxygenase 2 in ulcerative colitis-associated neoplasia. Am J Pathol 157: 737–745, 2000. Ahn B and Ohshima H. Suppression of intestinal polyposis in Apc(Min/⫹) mice by inhibiting nitric oxide production. Cancer Res 61: 8357– 8360, 2001. Arai N, Mitomi H, Ohtani Y, Igarashi M, Kakita A, and Okayasu I. Enhanced epithelial cell turnover associated with p53 accumulation and high p21WAF1/CIP1 expression in ulcerative colitis. Mod Pathol 12: 604 – 611, 1999. Aust DE, Terdiman JP, Willenbucher RF, Chang CG, MolinaroClark A, Baretton GB, Loehrs U, and Waldman FM. The APC/catenin pathway in ulcerative colitis-related colorectal carcinomas: a mutational analysis. Cancer 94: 1421–1427, 2002. Balish E and Warner T. Enterococcus faecalis induces inflammatory bowel disease in interleukin-10 knockout mice. Am J Pathol 160: 2253– 2257, 2002. Beck PL, Xavier R, Wong J, Ezedi I, Mashimo H, Mizoguchi A, Mizoguchi E, Bhan AK, and Podolsky DK. Paradoxical roles of different nitric oxide synthase isoforms in colonic injury. Am J Physiol Gastrointest Liver Physiol 286: G137–G147, 2004. Berg DJ, Davidson N, Kuhn R, Muller W, Menon S, Holland G, Thompson-Snipes L, Leach MW, and Rennick D. Enterocolitis and colon cancer in interleukin-10-deficient mice are associated with aberrant cytokine production and CD4⫹ TH1-like responses. J Clin Invest 98: 1010 –1020, 1996. Boland CR, Thibodeau SN, Hamilton SR, Sidransky D, Eshleman JR, Burt RW, Meltzer SJ, Rodriguez-Bigas MA, Fodde R, Ranzani GN, and Srivastava S. A National Cancer Institute Workshop on Microsatellite Instability for cancer detection and familial predisposition: development of international criteria for the determination of microsatellite instability in colorectal cancer. Cancer Res 58: 5248 –5257, 1998. Brentnall TA, Crispin DA, Bronner MP, Cherian SP, Hueffed M, Rabinovitch PS, Rubin CE, Haggitt RC, and Boland CR. Microsatellite instability in nonneoplastic mucosa from patients with chronic ulcerative colitis. Cancer Res 56: 1237–1240, 1996. Brentnall TA, Crispin DA, Rabinovitch PS, Haggitt RC, Rubin CE, Stevens AC, and Burmer GC. Mutations in the p53 gene: an early marker of neoplastic progression in ulcerative colitis. Gastroenterology 107: 369 –378, 1994. Brentnall TA, Rubin CE, Crispin DA, Stevens A, Batchelor RH, Haggitt RC, Bronner MP, Evans JP, McCahill LE, Bilir N, Boland CR, and Rabinovitch PS. A germline substitution in the human MSH2 gene is associated with high-grade dysplasia and cancer in ulcerative colitis. Gastroenterology 109: 151–155, 1995. Bull AW. The role of peroxisome proliferator-activated receptor gamma in colon cancer and inflammatory bowel disease. Arch Pathol Lab Med 127: 1121–1123, 2003. Burmer GC, Rabinovitch PS, Haggitt RC, Crispin DA, Brentnall TA, Kolli VR, Stevens AC, and Rubin CE. Neoplastic progression in ulcerative colitis: histology, DNA content, and loss of a p53 allele. Gastroenterology 103: 1602–1610, 1992. Bus PJ, Nagtegaal ID, Verspaget HW, Lamers CB, Geldof H, Van Krieken JH, and Griffioen G. Mesalazine-induced apoptosis of colorectal cancer: on the verge of a new chemopreventive era? Aliment Pharmacol Ther 13: 1397–1402, 1999. Chang CL, Marra G, Chauhan DP, Ha HT, and Chang DK, Ricciardiello L, Randolph A, Carethers JM, Boland CR. Oxidative stress inactivates the human DNA mismatch repair system. Am J Physiol Cell Physiol 283: C148 –C154, 2002. Chen R, Rabinovitch PS, Crispin DA, Emond MJ, Koprowicz KM, Bronner MP, and Brentnall TA. DNA fingerprinting abnormalities can distinguish ulcerative colitis patients with dysplasia and cancer from those who are dysplasia/cancer-free. Am J Pathol 162: 665– 672, 2003. Chu FF, Esworthy RS, Chu PG, Longmate JA, Huycke MM, Wilczynski S, and Doroshow JH. Bacteria-induced intestinal cancer in mice with disrupted Gpx1 and Gpx2 Genes. Cancer Res 64: 962–968, 2004. Cooper HS, Everley L, Chang WC, Pfeiffer G, Lee B, Murthy S, and Clapper ML. The role of mutant Apc in the development of dysplasia and cancer in the mouse model of dextran sulfate sodium-induced colitis. Gastroenterology 121: 1407–1416, 2001. Cooper HS, Murthy S, Kido K, Yoshitake H, and Flanigan A. Dysplasia and cancer in the dextran sulfate sodium mouse colitis model: relevance to colitis-associated neoplasia in the human. Carcinogenesis 21: 757–768, 2000. G15 Theme G16 ROLE OF INFLAMMATION IN COLITIS-ASSOCIATED COLORECTAL CANCER 63. 64. 65. 66. 67. 68. 69. 70. 71. 72. 73. 74. 75. 76. 77. 78. 79. 80. 81. AJP-Gastrointest Liver Physiol • VOL impact on microbial flora, inflammation and tumour development in IL-10 knockout mice. Aliment Pharmacol Ther 15: 1219 –1225, 2001. O’Sullivan JN, Bronner MP, Brentnall TA, Finley JC, Shen WT, Emerson S, Emond MJ, Gollahon KA, Moskovitz AH, Crispin DA, Potter JD, and Rabinovitch PS. Chromosomal instability in ulcerative colitis is related to telomere shortening. Nat Genet 32: 280 –284, 2002. Pinczowski D, Ekbom A, Baron J, Yuen J, and Adami HO. Risk factors for colorectal cancer in patients with ulcerative colitis: a casecontrol study. Gastroenterology 107: 117–120, 1994. Rabinovitch PS, Dziadon S, Brentnall TA, Emond MJ, Crispin DA, Haggitt RC, and Bronner MP. Pancolonic chromosomal instability precedes dysplasia and cancer in ulcerative colitis. Cancer Res 59: 5148 – 5153, 1999. Rachmilewitz D, Stamler JS, Bachwich D, Karmeli F, Ackerman Z, and Podolsky DK. Enhanced colonic nitric oxide generation and nitric oxide synthase activity in ulcerative colitis and Crohn’s disease. Gut 36: 718 –723, 1995. Rachmilewitz D, Stamler JS, Karmeli F, Mullins ME, Singel DJ, Loscalzo J, Xavier RJ, and Podolsky DK. Peroxynitrite-induced rat colitis–a new model of colonic inflammation. Gastroenterology 105: 1681–1688, 1993. Redston MS, Papadopoulos N, Caldas C, Kinzler KW, and Kern SE. Common occurrence of APC and K-ras gene mutations in the spectrum of colitis-associated neoplasias. Gastroenterology 108: 383–392, 1995. Ricciardiello L, Baglioni M, Giovannini C, Pariali M, Cenacchi G, Ripalti A, Landini MP, Sawa H, Nagashima K, Frisque RJ, Goel A, Boland CR, Tognon M, Roda E, and Bazzoli F. Induction of chromosomal instability in colonic cells by the human polyomavirus JC virus. Cancer Res 63: 7256 –7262, 2003. Ritland SR, Leighton JA, Hirsch RE, Morrow JD, Weaver AL, and Gendler SJ. Evaluation of 5-aminosalicylic acid (5-ASA) for cancer chemoprevention: lack of efficacy against nascent adenomatous polyps in the Apc(Min) mouse. Clin Cancer Res 5: 855– 863, 1999. Rogler G, Brand K, Vogl D, Page S, Hofmeister R, Andus T, Knuechel R, Baeuerle PA, Scholmerich J, and Gross V. Nuclear factor B is activated in macrophages and epithelial cells of inflamed intestinal mucosa. Gastroenterology 115: 357–369, 1998. Rubin CE, Haggitt RC, Burmer GC, Brentnall TA, Stevens AC, Levine DS, Dean PJ, Kimmey M, Perera DR, and Rabinovitch PS. DNA aneuploidy in colonic biopsies predicts future development of dysplasia in ulcerative colitis. Gastroenterology 103: 1611–1620, 1992. Rudolph U, Finegold MJ, Rich SS, Harriman GR, Srinivasan Y, Brabet P, Boulay G, Bradley A, and Birnbaumer L. Ulcerative colitis and adenocarcinoma of the colon in G␣i2-deficient mice. Nat Genet 10: 143–150, 1995. Rutter M, Saunders B, Wilkinson K, Rumbles S, Schofield G, Kamm M, Williams C, Price A, Talbot I, and Forbes A. Severity of inflammation is a risk factor for colorectal neoplasia in ulcerative colitis. Gastroenterology 126: 451– 459, 2004. Santini V, Kantarjian HM, and Issa JP. Changes in DNA methylation in neoplasia: pathophysiology and therapeutic implications. Ann Intern Med 134: 573–586, 2001. Sato F, Harpaz N, Shibata D, Xu Y, Yin J, Mori Y, Zou TT, Wang S, Desai K, Leytin A, Selaru FM, Abraham JM, and Meltzer SJ. Hypermethylation of the p14(ARF) gene in ulcerative colitis-associated colorectal carcinogenesis. Cancer Res 62: 1148 –1151, 2002. Seril DN, Liao J, Ho KL, Yang CS, and Yang GY. Inhibition of chronic ulcerative colitis-associated colorectal adenocarcinoma development in a murine model by N-acetylcysteine. Carcinogenesis 23: 993–1001, 2002. Seril DN, Liao J, Yang GY, and Yang CS. Oxidative stress and ulcerative colitis-associated carcinogenesis: studies in humans and animal models. Carcinogenesis 24: 353–362, 2003. Shattuck-Brandt RL, Varilek GW, Radhika A, Yang F, Washington MK, and DuBois RN. Cyclooxygenase 2 expression is increased in the stroma of colon carcinomas from IL-10(⫺/⫺) mice. Gastroenterology 118: 337–345, 2000. Sohn KJ, Shah SA, Reid S, Choi M, Carrier J, Comiskey M, Terhorst C, and Kim YI. Molecular genetics of ulcerative colitis-associated colon cancer in the interleukin 2- and 2-microglobulin-deficient mouse. Cancer Res 61: 6912– 6917, 2001. Steele VE, Hawk ET, Viner JL, and Lubet RA. Mechanisms and applications of non-steroidal anti-inflammatory drugs in the chemoprevention of cancer. Mutat Res 523–524: 137–144, 2003. 287 • JULY 2004 • www.ajpgi.org Downloaded from http://ajpgi.physiology.org/ by 10.220.33.5 on June 15, 2017 41. Hokari R, Kato S, Matsuzaki K, Kuroki M, Iwai A, Kawaguchi A, Nagao S, Miyahara T, Itoh K, Sekizuka E, Nagata H, Ishii H, and Miura S. Reduced sensitivity of inducible nitric oxide synthase-deficient mice to chronic colitis. Free Radic Biol Med 31: 153–163, 2001. 42. Hsieh CJ, Klump B, Holzmann K, Borchard F, Gregor M, and Porschen R. Hypermethylation of the p16INK4a promoter in colectomy specimens of patients with long-standing and extensive ulcerative colitis. Cancer Res 58: 3942–3945, 1998. 43. Hussain SP, Amstad P, Raja K, Ambs S, Nagashima M, Bennett WP, Shields PG, Ham AJ, Swenberg JA, Marrogi AJ, and Harris CC. Increased p53 mutation load in noncancerous colon tissue from ulcerative colitis: a cancer-prone chronic inflammatory disease. Cancer Res 60: 3333–3337, 2000. 44. Hussain SP, Hofseth LJ, and Harris CC. Radical causes of cancer. Nature Rev Cancer 276: 276 –285, 2003. 45. Issa JP, Ahuja N, Toyota M, Bronner MP, and Brentnall TA. Accelerated age-related CpG island methylation in ulcerative colitis. Cancer Res 61: 3573–3577, 2001. 46. Itzkowitz SH. Cancer prevention in patients with inflammatory bowel disease. Gastroenterol Clin North Am 31: 1133–1144, 2002. 47. Itzkowitz SH and Harpaz N. Diagnosis and management of dysplasia in patients with inflammatory bowel disease. Gastroenterology 126: 2004. In press. 48. Jass JR, Whitehall VL, Young J, and Leggett BA. Emerging concepts in colorectal neoplasia. Gastroenterology 123: 862– 876, 2002. 49. Kado S, Uchida K, Funabashi H, Iwata S, Nagata Y, Ando M, Onoue M, Matsuoka Y, Ohwaki M, and Morotomi M. Intestinal microflora are necessary for development of spontaneous adenocarcinoma of the large intestine in T-cell receptor  chain and p53 double-knockout mice. Cancer Res 61: 2395–2398, 2001. 50. Kimura H, Hokari R, Miura S, Shigematsu T, Hirokawa M, Akiba Y, Kurose I, Higuchi H, Fujimori H, Tsuzuki Y, Serizawa H, and Ishii H. Increased expression of an inducible isoform of nitric oxide synthase and the formation of peroxynitrite in colonic mucosa of patients with active ulcerative colitis. Gut 42: 180 –187, 1998. 51. Kohonen-Corish MR, Daniel JJ, te Riele H, Buffinton GD, and Dahlstrom JE. Susceptibility of Msh2-deficient mice to inflammationassociated colorectal tumors. Cancer Res 62: 2092–2097, 2002. 52. Kullmann F, Messmann H, Alt M, Gross V, Bocker T, Scholmerich J, and Ruschoff J. Clinical and histopathological features of dextran sulfate sodium induced acute and chronic colitis associated with dysplasia in rats. Int J Colorectal Dis 16:238 – 46, 2001. 53. Marnett LJ. Oxyradicals and DNA damage. Carcinogenesis 21: 361– 370, 2000. 54. Mathy C, Schneider K, Chen YY, Varma M, Terdiman JP, and Mahadevan U. Gross versus microscopic pancolitis and the occurrence of neoplasia in ulcerative colitis. Inflamm Bowel Dis 9: 351–355, 2003. 55. McKenzie SJ, Baker MS, Buffinton GD, and Doe WF. Evidence of oxidant-induced injury to epithelial cells during inflammatory bowel disease. J Clin Invest 98: 136 –141, 1996. 56. McKenzie SM, Doe WF, and Buffinton GD. 5-aminosalicylic acid prevents oxidant mediated damage of glyceraldehyde-3-phosphate dehydrogenase in colon epithelial cells. Gut 44: 180 –185, 1999. 57. Moore KW, de Waal Malefyt R, Coffman RL, and O’Garra A. Interleukin-10 and the interleukin-10 receptor. Annu Rev Immunol 19: 683–765, 2001. 58. Niho N, Takahashi M, Kitamura T, Shoji Y, Itoh M, Noda T, Sugimura T, and Wakabayashi K. Concomitant suppression of hyperlipidemia and intestinal polyp formation in Apc-deficient mice by peroxisome proliferator-activated receptor ligands. Cancer Res 63: 6090 – 6095, 2003. 59. Noffsinger A, Kretschmer S, Belli J, Fogt F, and Fenoglio-Preiser C. Microsatellite instability is uncommon in intestinal mucosa of patients with Crohn’s disease. Dig Dis Sci 45: 378 –384, 2000. 60. Noffsinger AE, Belli JM, Fogt F, Fischer J, Goldman H, and FenoglioPreiser CM. A germline hMSH2 alteration is unrelated to colonic microsatellite instability in patients with ulcerative colitis. Hum Pathol 30: 8 –12, 1999. 61. Okayasu I, Yamada M, Mikami T, Yoshida T, Kanno J, and Ohkusa T. Dysplasia and carcinoma development in a repeated dextran sulfate sodium-induced colitis model. J Gastroenterol Hepatol 17: 1078 –1083, 2002. 62. O’Mahony L, Feeney M, O’Halloran S, Murphy L, Kiely B, Fitzgibbon J, Lee G, O’Sullivan G, Shanahan F, and Collins JK. Probiotic Theme ROLE OF INFLAMMATION IN COLITIS-ASSOCIATED COLORECTAL CANCER 82. Sturlan S, Oberhuber G, Beinhauer BG, Tichy B, Kappel S, Wang J, and Rogy MA. Interleukin-10-deficient mice and inflammatory bowel disease associated cancer development. Carcinogenesis 22: 665– 671, 2001. 83. Su CG, Wen X, Bailey ST, Jiang W, Rangwala SM, Keilbaugh SA, Flanigan A, Murthy S, Lazar MA, and Wu GD. A novel therapy for colitis utilizing PPAR-␥ ligands to inhibit the epithelial inflammatory response. J Clin Invest 104: 383–389, 1999. 84. Tarmin L, Yin J, Harpaz N, Kozam M, Noordzij J, Antonio LB, Jiang HY, Chan O, Cymes K, and Meltzer SJ. Adenomatous polyposis coli gene mutations in ulcerative colitis-associated dysplasias and cancers versus sporadic colon neoplasms. Cancer Res 55: 2035–2038, 1995. 85. Toyota M, Ahuja N, Ohe-Toyota M, Herman JG, Baylin SB, and Issa JP. CpG island methylator phenotype in colorectal cancer. Proc Natl Acad Sci USA 96: 8681– 8686, 1999. G17 86. Umetani N, Sasaki S, Watanabe T, Shinozaki M, Matsuda K, Ishigami H, Ueda E, and Muto T. Genetic alterations in ulcerative colitisassociated neoplasia focusing on APC, K-ras gene and microsatellite instability. Jpn J Cancer Res 90: 1081–1087, 1999. 87. Willenbucher RF, Aust DE, Chang CG, Zelman SJ, Ferrell LD, Moore DH 2nd, and Waldman FM. Genomic instability is an early event during the progression pathway of ulcerative-colitis-related neoplasia. Am J Pathol 154: 1825–1830, 1999. 88. Yamamoto Y and Gaynor RB. Therapeutic potential of inhibition of the NF-kB pathway in the treatment of inflammation and cancer. J Clin Invest 107: 135–142, 2001. 89. Yin J, Harpaz N, Tong Y, Huang Y, Laurin J, Greenwald BD, Hontanosas M, Newkirk C, and Meltzer SJ. p53 point mutations in dysplastic and cancerous ulcerative colitis lesions. Gastroenterology 104: 1633–1639, 1993. Downloaded from http://ajpgi.physiology.org/ by 10.220.33.5 on June 15, 2017 AJP-Gastrointest Liver Physiol • VOL 287 • JULY 2004 • www.ajpgi.org