Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
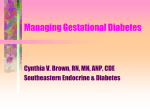
CASE STUDY www.nature.com/clinicalpractice/endmet A patient with severe, recurrent hypoglycemia and glycemic lability who underwent islet transplantation Edmond A Ryan* and AM James Shapiro S U M M A RY Background A 48-year-old woman who was diagnosed with type 1 diabetes at 5 years of age presented to our Clinical Islet Transplant Program with severe, recurrent hypoglycemia and glycemic lability. She was diligent with her diet, used a continuous subcutaneous insulin infusion pump (32 U per day), and monitored her glucose levels typically eight times a day. The patient usually had one hypoglycemic reaction a day, experienced a severe reaction once a month, and had marked variability of her glucose values. On presentation, her HYPO score was 584 and her lability index was 868 mmol/l2/h per week. Investigations HYPO score, lability index score, screening for diabetes complications, and routine pretransplant evaluation. Diagnosis Severe, recurrent hypoglycemia and glycemic lability associated with type 1 diabetes. Management The patient underwent islet transplantation. Posttransplant, the problems with hypoglycemia abated and excellent stable glycemic control was attained, although some side effects from the immunosuppressive drug, sirolimus, were evident. Insulin was reinstituted 2.5 years after surgery, at lower doses than before the transplant because of deterioration in graft function. Occasional episodes of hypoglycemia have occurred and some glycemic lability has recurred, although endogenous insulin secretion is still preserved. KEYWORDS glycemic lability, hypoglycemia, immunosuppression, islet transplantation, type 1 diabetes CME EA Ryan is the Medical Director and AMJ Shapiro is the Director of the Clinical Islet Transplant Program, AB, Canada. Correspondence *Clinical Islet Transplant Program, 2000 College Plaza, 8215 112th Street, Edmonton, AB, T6G 2C8, Canada [email protected] Received 10 January 2006 Accepted 7 April 2006 www.nature.com/clinicalpractice doi:10.1038/ncpendmet0201 JUNE 2006 VOL 2 NO 6 This article offers the opportunity to earn one Category 1 credit toward the AMA Physician’s Recognition Award. THE CASE A 48-year-old woman who was diagnosed with type 1 diabetes 43 years previously, presented early in 2001 to our Clinical Islet Transplant Program with recurrent hypoglycemia and glycemic lability that had been present for several years. She was diligent with her diet, used a continuous subcutaneous insulin infusion pump, and monitored her glucose levels typically eight times a day. Total insulin requirements were 32 U per day (0.6 U/kg). Despite these efforts, she usually had one hypoglycemic reaction a day. The patient felt she needed outside help to recognize the hypoglycemia about twice a month, and third-party assistance to treat the hypoglycemia reaction once a month. In the year before presentation, she had required glucagon therapy twice for her hypoglycemia. On presentation, the patient’s HYPO SCORE was 584 (median in a typical patient with type 1 diabetes 143; interquartile range 46–423) and her LABILITY INDEX (LI) was 868 mmol/l2/h per week (median in a typical patient with type 1 diabetes 223 mmol/l2/h per week; interquartile range 130–329 mmol/l2/h per week).1 The glycated hemoglobin A1c (HbA1c) was 6.6% (normal range 4.3–6.1%). Given that her problems with hypoglycemia and glycemic lability were serious, and that both her HYPO score and LI exceeded the 75th percentile, she was offered an islet transplant. The patient’s past history was noncontributory. In terms of diabetes complications, she had been treated for proliferative retinopathy, her microalbumin excretion rate was 9 μg/min (she had been taking 10 mg enalapril per day for 3 years) and she experienced no neuropathy or vascular disease. The patient underwent an islet transplant in late 2001. Briefly, percutaneous access to the portal vein was established in the radiology suite and the islet preparation was allowed to infuse slowly with regular monitoring of the NATURE CLINICAL PRACTICE ENDOCRINOLOGY & METABOLISM 349 ©2006 Nature Publishing Group CASE STUDY www.nature.com/clinicalpractice/endmet Capillary fasting glucose (mmol/l) 11 – 10 – 9– 8– 7– 6– 5– Insulin units/kg per day Capillary postmeal glucose (mmol/l) 16 – 14 – 12 – 10 – 8– 6– 4– Capillary premeal glucose (mmol/l) HbA1c (%) 7.0 – 6.8 – 6.6 – 6.4 – 6.2 – 6.0 – 5.8 – 10 – 9– 8– 7– 6– 5– 0.6 – 0.5 – 0.4 – 0.3 – 0.2 – 0.1 – 0– Lability score 1000 – 800 – 600 – 400 – 200 – Hypoglycemia score 0– 700 – 600 – 500 – 400 – 300 – 200 – 100 – 0– Pre-TX 6 months 12 months 24 months 36 months 48 months Time Figure 1 Changes in hemoglobin A1c, capillary fasting, premeal and postmeal glucose levels, insulin use, lability index, and hypoglycemia score pretransplant and over 4 years of follow-up post-transplant in the patient described. HbA1c, hemoglobin A1c; pre-TX, pretransplant. 350 NATURE CLINICAL PRACTICE ENDOCRINOLOGY & METABOLISM ©2006 Nature Publishing Group portal pressure to help detect any possible thrombosis. Once the infusion was complete, the catheter was removed and the tract plugged to lessen the risk of bleeding. After the transplant, she was given the immunosuppressant drugs sirolimus, starting dose of 0.1 mg/kg per day (target trough levels 12–15 ng/ml), and tacrolimus, starting dose of 2 mg twice daily (target trough levels 3–6 ng/ml). The problems with hypoglycemia resolved, and the patient’s glucose levels stabilized, but she still required 10 U of insulin per day. The patient had a second transplant 4 months later because of her need for continuing exogenous insulin; she received a total of 593,270 islet equivalents or 10,594 islet equivalents per kg over the two procedures. After the second transplant, the patient became insulin independent and remained off insulin for 2.5 years (Figure 1). Her HbA1c fell to 6%, and 77% of her premeal capillary glucose values were in the target range of 3.5–7.8 mmol/l. Over a 1-month period, no glucose values were under 3.5 mmol/l and only three values were over 10.0 mmol/l. The patient continued to receive immunosuppressive therapy: sirolimus (target trough levels 8–10 ng/ml) and tacrolimus (target trough levels 3–6 ng/ml). In 2003, 2 years after the transplants, she had no problems with hypoglycemia, her HYPO score was 0, and the LI was 90 mmol/l2/h per week. The patient’s mean premeal capillary glucose levels were 6.5 mmol/l (target levels 5.0–7.2 mmol/l), but her fasting glucose levels were elevated to 7.2 mmol/l (normal <5.6 mmol/l). Renal function remained normal, with serum creatinine levels of 63 μmol/l, an albumin excretion rate of 11 μg/min, and the creatinine clearance was 1.79 ml/sec/1.73m2. Hypercholesterolemia developed and she was given 40 mg simvastatin per day and enalapril was continued at a higher dose of 10 mg twice daily because her blood pressure had risen. The patient experienced problems with mouth ulcers, gastrointestinal upset, and peripheral edema that were thought to be side effects of sirolimus therapy. Sirolimus was, therefore, stopped and 1,000 mg mycophenolate mofetil was given twice daily to the patient. The side effects improved within 3 months of discontinuing sirolimus, but she continued on statin therapy for hypercholesterolemia and antihypertensive medications. In 2004, the patient resumed insulin therapy of 12 U per day because of a deterioration in graft function and because her postmeal capillary RYAN AND SHAPIRO JUNE 2006 VOL 2 NO 6 CASE STUDY www.nature.com/clinicalpractice/endmet glucose values had risen to 9.1 mmol/l. After the patient resumed insulin therapy, she experienced occasional hypoglycemic episodes that gave some warning symptoms and did not require third-party assistance. Some glycemic lability had also recurred. The patient felt that the islet transplant had improved her major concerns relating to severe hypoglycemia and glycemic lability. In 2006, at the last patient followup, she was taking 23 U of insulin therapy per day. DISCUSSION OF DIAGNOSIS Hypoglycemia is, by far, the most common acute complication of patients with type 1 diabetes; for a minority of patients the problem progresses to episodes of severe hypoglycemia, such that the patients become a risk to themselves and their surroundings. Severe hypoglycemia is defined as an episode of hypoglycemia in which third-party assistance is required, and up to one third of patients with type 1 diabetes might have episodes of severe hypoglycemia in a year.2 Typically, severe hypoglycemia is associated with hypoglycemic unawareness—the occurrence of hypoglycemia without symptoms that permit recognition of the condition. Hypoglycemia elicits the classic defense mechanism, causing the release of catecholamines, glucagon, cortisol, and growth hormone; the former two hormones act within minutes of the occurrence of hypoglycemia. In patients without diabetes, a decrease in the levels of endogenous insulin and increase in levels of glucagon are the pre-eminent defenses. Neither of these mechanisms is operative in patients with type 1 diabetes. Characteristically, patients with type 1 diabetes lose their glucagon response to hypoglycemia.3 The presence of hyperinsulinemia and the lack of a fall in levels of intraislet insulin are responsible for the loss of the glucagon response to hypoglycemia.4 A patient with type 1 diabetes, therefore, is completely dependent on the catecholamine response to correct falling glucose levels, and the associated sympathoadrenal response for warning of the glucose decrement.5 The loss of autonomic warning symptoms with a foundation of a blunted glucagon and catecholamine response sets the stage for recurrent, severe hypoglycemia. Typically, this loss of sympathoadrenal response is inducible by recurrent episodes of hypoglycemia6 and is potentially correctable by the scrupulous avoidance of hypoglycemia.7 Even though hypoglycemia JUNE 2006 VOL 2 NO 6 RYAN AND SHAPIRO is more common in the presence of severe autonomic neuropathy, it is not thought to be caused by a structural defect in the autonomic nervous system. Some have proposed that the defect is cause by hypoglycemia-induced autonomic failure, but the exact mechanism remains unclear.5 If a patient has severe hypoglycemia it is mandatory to review dietary practices, insulin injection techniques and timing, and insulin regimen. Exclusion of associated diseases, such as celiac disease, Addison’s disease, thyroid disease, and gastroparesis, that might have a role is essential. All of these associated diseases were examined in the patient described and, as often occurs, no obvious cause was found. Some patients seem to have ongoing low glucose levels and resist all attempts to raise the ambient glucose values, as they feel unwell with glucose values that are any higher. Other patients have very labile diabetes—a condition characterized by extremely variable glucose control associated with unpredictable responses to insulin. Patients with labile diabetes and hypoglycemia are the most challenging to treat, given the unpredictability of their response to insulin. Insulininfusion pumps, carbohydrate counting, and frequent glucose monitoring might all help, as might the new continuous glucose monitors, which use a subcutaneous glucose sensor.8 Problems persist in a subset of these patients, despite intensive diabetes therapy, as is evident from the case presented. Quantifying the problems associated with hypoglycemia has been challenging. The CLARKE SCORE helps predict future problems with hypoglycemia, but is less quantitative than the HYPO score.9 The mean amplitude of glycemic excursion (MAGE) has been used to quantify glycemic lability, but only uses the glucose values over a 2-day period. The MAGE correlated with the LI (coefficient of correlation, r = 0.291; P = 0.004), but the LI was much more closely correlated with a clinical assessment of lability than with the MAGE (r = 0.868 and 0.328, respectively).1 A HYPO score of more than 1,047 (90th percentile) or a LI of more than 433 mmol/l2/h per week (90th percentile) indicates serious problems with hypoglycemia or glycemic lability, respectively. The patient described here presented to us with problems caused by both hypoglycemia and glycemic lability and she was, therefore, considered for an islet transplant. GLOSSARY HYPO SCORE A 4-week period of intensive glucose monitoring coupled with a year-long history of episodes of severe hypoglycemia that provides a score of the severity of hypoglycemia; also known as hypoglycemia score LABILITY INDEX (LI) This index provides a measure of glycemic lability and is based on the square of change in levels of glucose from one reading to the next, divided by the time interval and summed for a week CLARKE SCORE Predicts future problems with hypoglycemia NATURE CLINICAL PRACTICE ENDOCRINOLOGY & METABOLISM 351 ©2006 Nature Publishing Group CASE STUDY www.nature.com/clinicalpractice/endmet TREATMENT AND MANAGEMENT Islet transplantation provides endogenous insulin that corrects glycemic lability and is accompanied by a decrease in the number of episodes of hypoglycemia, although, typically, two transplants are required.10 Patients suitable for transplantation include those with problems with hypoglycemia or lability, despite optimization of diabetes therapy and no elevation of serum creatinine levels. Quantification of hypoglycemia is facilitated by the HYPO score and the glycemic instability by the LI. Either a HYPO score or LI over the 90th percentile or both over the 75th percentile warrants consideration of an islet transplant. The success of islet transplantation in terms of stabilizing problematic hypoglycemia is testimony to the dominance of regulated insulin secretion in glucoregulation. Glucose control was stable in the patient described after transplantation. The fasting glucose levels were disproportionately high, a common feature after islet transplantation, which might reflect some impairment in the regulation of endogenous glucose output by the intrahepatic islet source of insulin. The price for these benefits, however, is life-long immunosuppression and its attendant side effects—most commonly mouth ulcers, increased cholesterol levels, hypertension, gastrointestinal upset, and proteinuria,11 plus ovarian cysts and menorrhagia in premenopausal women.12 In addition, long-term insulin independence is rarely maintained, as was the case in the patient described, the probable explanation being the limited islet mass that engrafts.10,13,14 The patient described experienced many of the complications encountered after islet transplantation, including gastrointestinal upset, hypercholesterolemia, hypertension, and mouth ulcers. Interestingly, many of these abated when sirolimus was stopped. Of more importance was the patient’s need to restart insulin after 30 months and the recurrence of some problems with the sensing of hypoglycemia and lability. As reported, 90% of patients who undergo islet transplantation need to restart insulin therapy, although 80% have persistence of endogenous C-peptide.10 It is becoming apparent that the glucagon response to hypoglycemia is not normalized15,16 after intrahepatic islet transplantation. The role of the hepatic site in this lack of recovery might be important, because intraperitoneal islet transplants in dogs are associated with a 352 NATURE CLINICAL PRACTICE ENDOCRINOLOGY & METABOLISM ©2006 Nature Publishing Group normal glucagon response to hypoglycemia. It is possible that the autoregulation of glucose within the liver protects the transplanted islets from hypoglycemia and, hence, causes the blunted glucagon response. Also of note was the recurrence of occasional episodes of hypoglycemia once insulin was resumed, despite the use of lower doses of insulin compared with the pretransplantation dose and the continuing endogenous insulin release. This suggests that, in some patients, the impaired sympathoadrenal response is not fully restored to normal despite the patient being off insulin for years and presumably having avoided hypoglycemia during this interval. CONCLUSION Patients with recurrent, severe hypoglycemia and glycemic lability who are not responsive to intensive diabetes therapy (e.g. multiple daily insulin injections or use of continuous subcutaneous insulin infusion, frequent glucose monitoring, and careful dietary adherence) are eligible for an islet transplant, which can offer freedom from hypoglycemia as well as stable glucose values. The patient described exemplifies the advantages and disadvantages of an islet transplant. Posttransplantation, the patient experienced a marked relief from the problems of hypoglycemia, stable glucose values, and better glycemic control; however, she also experienced side effects from the immunosuppressive drugs, slight fasting hyperglycemia, and resumed taking small doses of insulin. The islets survive for many years, but the need for less toxic immunosuppression and enhanced function of the remaining islets is apparent. References 1 Ryan EA et al. (2004) Assessment of the severity of hypoglycemia and glycemic lability in type 1 diabetic subjects undergoing islet transplantation. Diabetes 53: 955–962 2 Pedersen-Bjergaard U et al. (2004) Severe hypoglycaemia in 1076 adult patients with type 1 diabetes: influence of risk markers and selection. Diabetes Metab Res Rev 20: 479–486 3 Cryer PE et al. (2003) Hypoglycemia in diabetes. Diabetes Care 26: 1902–1912 4 Gosmanov NR et al. (2005) Role of the decrement in intraislet insulin for the glucagon response to hypoglycemia in humans. Diabetes Care 28: 1124–1131 5 Cryer PE (2004) Diverse causes of hypoglycemiaassociated autonomic failure in diabetes. N Engl J Med 350: 2272–2279 6 Cryer PE (1992) Iatrogenic hypoglycemia as a cause of hypoglycemia-associated autonomic failure in IDDM. A vicious cycle. Diabetes 41: 255–260 RYAN AND SHAPIRO JUNE 2006 VOL 2 NO 6 CASE STUDY www.nature.com/clinicalpractice/endmet 7 Fanelli C et al. (1994) Long-term recovery from unawareness, deficient counterregulation and lack of cognitive dysfunction during hypoglycaemia, following institution of rational, intensive insulin therapy in IDDM. Diabetologia 37: 1265–1276 8 Bode B et al. (2004) Alarms based on real-time sensor glucose values alert patients to hypo- and hyperglycemia: the guardian continuous monitoring system. Diab Technol Therap 6: 105–113 9 Clarke WL et al. (1995) Reduced awareness of hypoglycemia in adults with IDDM. A prospective study of hypoglycemic frequency and associated symptoms. Diabetes Care 18: 517–522 10 Ryan EA et al. (2005) Five-year follow-up after clinical islet transplantation. Diabetes 54: 2060–2069 11 Senior PA et al. (2005) Proteinuria developing after clinical islet transplantation resolves with sirolimus withdrawal and increased tacrolimus dosing. Am J Transplant 5: 2318–2323 JUNE 2006 VOL 2 NO 6 RYAN AND SHAPIRO 12 Cure P et al. (2004) Alterations of the female reproductive system in recipients of islet grafts. Transplantation 78: 1576–1581 13 Hering BJ et al. (2005) Single-donor, marginal-dose islet transplantation in patients with type 1 diabetes. JAMA 293: 830–835 14 Froud T et al. (2005) Islet transplantation in type 1 diabetes mellitus using cultured islets and steroidfree immunosuppression: Miami experience. Am J Transplant 5: 2037–2046 15 Rickels MR et al. (2005) Islet cell hormonal responses to hypoglycemia after human islet cell transplantation for type 1 diabetes. Diabetes 54: 3205–3211 16 Paty BW et al. (2002) Intrahepatic islet transplantation in type 1 diabetic patients does not restore hypoglycemic hormonal counterregulation or symptom recognition after insulin independence. Diabetes 51: 3428–3434 Competing interests The authors declared they have no competing interests. NATURE CLINICAL PRACTICE ENDOCRINOLOGY & METABOLISM 353 ©2006 Nature Publishing Group