Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
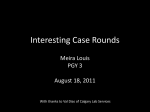
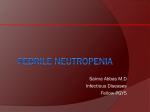
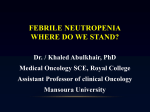
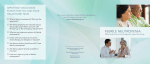
Outcomes of Febrile Children Presumed to be Immunocompetent Who Present with Leukopenia or Neutropenia to an Ambulatory Setting J. R. Serwint, MD1 M. M. Dias, MD3 H. Chang4 M. Sharkey, MD5 A. R. Walker, MD2 Summary: To determine significant medical outcomes in febrile children presenting to an ambulatory setting with neutropenia and/or leukopenia. Methods: Retrospective medical record review conducted on febrile patients who had a blood culture drawn, with white blood cell counts less than 5,000/mm3 and/or an absolute neutrophil count less than 1000/mm3. Ninety-one patients were identified; 5 with positive blood culture results, 13 with significant non-oncologic disease, and 3 patients with leukemia who had involvement of 2 or more cell lines. Conclusions: In the majority of patients, clinical judgment, physical findings, and review of all cell lines of the complete blood cell count identified those with significant disease. Clin Pediatr. 2005;44:593-600 Introduction P ediatricians use the total and the differential white blood cell (WBC) counts to aid in identifying children at increased risk of serious bacterial infections.1,2 WBC counts greater than 15,000/mm3, absolute neutrophil counts of greater than 10,000/mm3 and absolute band counts of greater than 1500/mm3 are associated with increased risk of bacterial infections, while WBC Department of Pediatrics, 1Division of General Pediatrics, 2Division of Emergency Medicine, Johns Hopkins Children’s Center, Baltimore, MD; 3CHOP Connection at Shore Memorial Hospital, Somers Point, NJ; 4Tender Care Pediatrics, Northfield NJ; 5University of Arkansas Area Health Education Center, Northwest Arkansas Pediatric Clinic, Fayettesville, AR. Presented in part at the Pediatric Academic Society meeting, San Francisco, CA, 1999. Reprint requests and correspondence to: Janet R. Serwint, MD, Division of General Pediatrics, Johns Hopkins Hospital, Park 389, 600 N. Wolfe St., Baltimore, MD 21287. © 2005 Westminster Publications, Inc., 708 Glen Cove Avenue, Glen Head, NY 11545, U.S.A. counts of 5000 to 15,000/mm 3 place a child at baseline risk.3 Few studies have examined the morbidity of febrile children presumed to be immunocompetent with leukopenia (WBC <5000/ mm3) or moderate to severe neutropenia (absolute neutrophil counts [ANC] <1000/mm3). Clinicians are often concerned that children with WBC counts less than 5000/mm3 or ANC less than 1000/mm3 may present because of marrow depletion from overwhelming sepsis, 1,2,4 while concern has been raised that patients with neutropenia may have difficulty fighting infections as has been the experience with patients with malignancies where guide- SEPTEMBER 2005 CLINICAL PEDIATRICS Downloaded from cpj.sagepub.com at PENNSYLVANIA STATE UNIV on September 21, 2016 593 Ser wint et al. lines suggest prompt initiation of empiric antibiotics.5 Other possible etiologies for leukopenia or neutropenia include bone marrow suppression from viral infections, medication side effects from antibiotics or anticonvulsants, or the inadvertent discovery of leukemia or cyclic neutropenia when a complete blood cell (CBC) count is obtained during a febrile illness. The ability to distinguish between these possibilities is essential to the clinician, who must make emergent decisions at the time of presentation based on the results of the WBC counts and the clinical appearance of the child. A febrile child with leukopenia or neutropenia may present a treatment challenge for a clinician in trying to decide whether to initiate antibiotics on an outpatient basis, hospitalize the patient, or pursue a further investigation for a hematologic abnormality or a malignancy. No studies, to our knowledge, have examined leukopenia and fever solely in febrile children who are presumed to be immunocompetent at the time of first contact to medical care. While Alario and colleagues examined neutropenia in well-appearing children, they included children from both inpatient and outpatient settings in addition to children who had received a complete blood cell count as part of a preoperative evaluation.6 Bowden and colleagues examined neutropenia in the pediatric population but included both hospitalized and ambulator y patients regardless of the cause for the visit.7 Eighty percent of patients in their study had no signs of infection. Bonadio and colleagues examined febrile children who had a CBC and blood culture performed as part of their evaluation, but their inclusion of both hospi- 594 talized and ambulatory patients biased the results toward a potentially more severely ill group.4 No one, to our knowledge, has studied febrile children with leukopenia or neutropenia from an ambulator y standpoint to obtain more accurate prevalence rates and determine the medical outcomes of these children. The aim of this study was to assist clinicians in their initial treatment decision for febrile children who present with leukopenia or neutropenia. The objectives were to: 1) determine the prevalence of positive blood culture results and hematologic conditions in febrile children presumed to be immunocompetent, found to be leukopenic or neutropenic on presentation for medical care; and 2) describe the medical outcomes for these children. Methods The study was a retrospective medical records review of patients who presented to a pediatric primar y care clinic or pediatric emergency department (ED) at a large, academic, urban hospital. Case identification took place using an Excel © database file of hospital laboratory results. Cases were identif ied by searching through the identification numbers of the pediatric primary care clinic or the pediatric emergency department from March 1, 1995 to January 1, 1998. Patients were included if they had 1) a temperature of 38°C or greater at the time of presentation or had a documented history of fever, 2) had a CBC count and a blood culture drawn during the visit, and 3) were found to have either leukopenia (defined as a WBC count <5000/mm3) or moderate to severe neutropenia, (de- fined as an ANC <1000/mm3), or both. The ANC was calculated by multiplying the total WBC by the percentage of segmented and band forms.1 Because this study was retrospective, all laboratory studies were done at the discretion of the treating physician. Other studies such as urine, cerebrospinal fluid, stool cultures, radiographs, etc. were performed when clinically indicated. All laboratory analyses were done at a single laboratory. Patients were excluded if chart review revealed a known disease entity to explain their neutropenia or leukopenia such as a malignancy (leukemia, lymphoma, solid tumors, brain tumors), receipt of immunosuppressive therapy, hematologic disease such as chronic or cyclic neutropenia or sickle cell disease, or if they were infected with human immunodeficiency virus (HIV). Patients were included if the chart review revealed that they were on anticonvulsants or antibiotics. The dependent variables, obtained by review of the chart and the electronic patient record, included age, gender, ethnicity, type of insurance, site where patient presented (clinic or pediatric emergency department), and whether the patient was taking antibiotics or anticonvulsants. Outcome variables included a positive blood culture result for a true pathogen, significant diagnoses, antibiotic administration after the evaluation of the patient, hospitalization, or death. Patients who were admitted to the hospital and/or seen in the outpatient settings were tracked for the next month via chart review at the parent institution to determine any additional diagnoses or outcomes. The study was approved by the Institutional Review Board at Johns Hopkins University School of Medicine. SEPTEMBER 2005 CLINICAL PEDIATRICS Downloaded from cpj.sagepub.com at PENNSYLVANIA STATE UNIV on September 21, 2016 Immunocompetent Children with Leukopenia or Neutropenia Data analysis was performed using the Statistical Program for Social Sciences (SPSS) version 10.0 (Chicago, IL). Chi-square analysis, Fisher’s exact test, and student t test were performed. Results Ninety-one febrile patients were identified during this period with leukopenia and/or neutropenia. This included 10 patients (11%) who were younger than 3 months of age, 55 (60%) 3 to 35 months of age, and 26 (29%) who were 36 months of age or older. The demographics of the patient population are presented in Table 1. The majority of patients had leukopenia while 13% exhibited both leukopenia and neutropenia (Figure 1). Figures 2 and 3 demonstrate the distribution of the degree of leukopenia and neutropenia in this study population. The medical outcomes of the patients included 5 patients (5.5%) with a positive blood culture result (Table 2), 6 (7%) with oncologic/hematologic disease (Table Table 1 DEMOGRAPHICS (n=91) Characteristic n (%) Male gender 55 (60%) African American 68 (75%) Medical assistance or self-pay 41 (45%) Site of visit Primary care clinic 32 (35%) Emergency department 59 (65%) Age < 3 mo 10 (11%) 3–35 mo 55 (60%) ≥36 mo 25 (29%) Antecedent medications associated with leukopenia/neutropenia Antibiotics 13 (14%) Anticonvulsants 3), one of whom had a positive blood culture result for Staphylococcus aureus, 12 (13%) with other significant diagnoses (Table 4), and 1 (1%) death while the re- 3 ( 3%) maining 68 patients (75%) experienced no significant morbidity. The one death occurred in a 6month-old female patient who presented to the ED with fever, Figure 1. Distribution of patients with leukopenia, neutropenia, or both. SEPTEMBER 2005 CLINICAL PEDIATRICS Downloaded from cpj.sagepub.com at PENNSYLVANIA STATE UNIV on September 21, 2016 595 Ser wint et al. Figure 2. Distribution of patients by total white blood cell count. Figure 3. Distribution of patients by absolute neutrophil count. 596 SEPTEMBER 2005 CLINICAL PEDIATRICS Downloaded from cpj.sagepub.com at PENNSYLVANIA STATE UNIV on September 21, 2016 Immunocompetent Children with Leukopenia or Neutropenia petechiae, and a toxic appearance. Purpura fulminans, septic shock, and disseminated intravascular coagulopathy developed rapidly. Her CBC parameters on admission included a WBC of 4700/mm3, ANC of 1683/mm3, hemoglobin of 8.0 g/dL, and platelet count of 67,000/mm 3. She was admitted to the pediatric intensive care unit and treated with antibiotics and aggressive supportive therapy, but died within 12 hours of admission. Her blood and urine culture results were negative and she had been too unstable to undergo a lumbar puncture. Of the 17 patients (19%) who under went lumbar puncture, only one had a positive culture result that grew a pathogen, in this case group B streptococcus. This patient is the same 1-month-old in- fant who was also found to have a positive blood culture result for the same organism. Thirty patients (33%) had a urine culture obtained and 5 patients (6%) had a stool culture obtained; all of these culture results were negative. Medical outcomes are presented by age in Figure 4. Children younger than 3 months of age were more likely to have been admitted and treated with antibiotics. When Table 2 PATIENTS WITH POSITIVE BLOOD CULTURE RESULTS (n=5) Age (mo) Pathogen WBC/mm3 ANC/mm3 Hgb (g/dL) Platelets Toxic Appearance Hospitalized Comments 1 Group B Streptococcus 1900 992 9.3 82,000 Yes Yes Confirmed with CSF culture results 9 Neisseria meningitidis 3300 2300 13.3 270,000 No No Admitted when aware + culture; no sequelae 88 Streptococcus pneumoniae 3000 Not done 11.6 157,000 Yes Yes Diagnosed with pneumonia 156 Staphylococcus aureus 25,000 0 0 36,000 Yes Yes Diagnosed with leukemia during admission 193 Escherichia coli 4100 3649 10.1 69,000 Yes Yes Septic at admission Table 3 PATIENTS FOUND TO HAVE ONCOLOGIC/HEMATOLOGIC DISEASE (n=6) Age (mo) Diagnosis WBC/mm3 ANC/mm3 Hgb (g/dL) Platelets 27 Leukemia 2400 24 5.3 309,000 39 Leukemia 2400 30 8.1 119,000 156 Leukemia 25,000 0 6.0 36,000 Presented with S. aureus bacteremia Comments 6 Chronic neutropenia 6000 726 11.5 359,000 Confirmed by hematology service 11 Chronic neutropenia 8100 405 10.5 391,000 Confirmed by hematology service 51 Chronic neutropenia 6700 268 12.8 512,000 Confirmed by hematology service SEPTEMBER 2005 CLINICAL PEDIATRICS Downloaded from cpj.sagepub.com at PENNSYLVANIA STATE UNIV on September 21, 2016 597 Ser wint et al. Table 4 OTHER SPECIFIC DIAGNOSES (n=12) Diagnosis Mean Age (mo) (Range) Mean WBC/mm3 (Range) Mean ANC/mm3 (Range) 7 Pneumonia 68 (10–202) 4930 (3700–8400) 1855 (777–3044) 1 Intussusception 7 3800 1700 1 Cellulitis 14 4106 600 1 Labial abscess 39 3500 35 1 Osteomyelitis 88 400 2488 1 Rocky Mountain spotted fever 106 4400 2790 No. of Patients Figure 4. Medical outcomes by age. considering medical outcomes by degrees of neutropenia and leukopenia, patients diagnosed with oncologic/hematologic disorders 5/6 (83%) were more likely to have an ANC less than 500, compared to those without 598 6/74 (9%), OR 61, (95% CI 5.3, 1662, p <0.001). In comparing patients with a WBC count of less than 3000/mm3, those 2/4 (33%) of patients with oncologic/hematologic disorders had this degree of leukopenia, compared to 4/85 (5%) of patients without these disorders. This approached statistical significance with OR 10, (95% CI 0.94, 105, p = 0.05. Neither the degree of neutropenia nor leukopenia was predictive in identifying those with bacteremia. SEPTEMBER 2005 CLINICAL PEDIATRICS Downloaded from cpj.sagepub.com at PENNSYLVANIA STATE UNIV on September 21, 2016 Immunocompetent Children with Leukopenia or Neutropenia Discussion This study examined the outcomes of febrile children thought to be immunocompetent who presented with leukopenia and/or neutropenia. No serious outcomes occurred in the majority of patients, presumably experiencing a transient leukopenia and/or neutropenia as a result of a viral infection. Boxer has commented that patients with neutropenia in conjunction with a malignancy are more likely to develop serious bacterial infections because their entire cellular immune system is compromised while those with transient neutropenia have an intact cellular immune system.1 The prevalence of bacteremia in this study, including all age groups, was 5.5%. However, only 1 patient younger than 3 months and 1 patient in the 3- to 36-month age groups had a positive blood culture result. Our results are similar to those of Bonadio and colleagues, who found that febrile infants younger than 8 weeks of age with neutropenia were not at higher risk of serious bacterial infections.4 In the 3- to 36-month age group, this would have led to a prevalence of 1/55 or 1.8%. This is comparable to present prevalence rates of bacteremia.8 The one positive blood culture result in this age group was due to Neisseria meningitidis, an organism that is regularly difficult to diagnose and this child had not received antibiotics at presentation. Twenty-five percent to 50% of children who presented with meningococcal disesase reported in retrospective series have been evaluated as outpatients in the 2 to 3 days before diagnosis,9-12 and these children do not commonly have leukocytosis.9,11,13 In a study by Fleischer, 3 of the 43 patients in the 2 series of meningo- coccal bacteremia had WBC counts less than 5000/mm 3, as was the case in our study.14 The higher rate of positive blood culture results in the patients older than 36 months may represent a bias arising from the fact that patients who appeared more ill in this age group would have been more likely to have had blood cultures obtained. Four of the five patients with bacteremia were hospitalized at the time of presentation because of a toxic appearance at admission as was the patient who died of purpura fulminans. As would be expected when looking at the distribution of leukopenia and neutropenia, the more severe either is, the less frequently either occurs. In looking at the helpfulness of these parameters, an ANC less than 500/mm3 was more predictive of oncologic/hematologic disease and a WBC count less than 3000/mm3 approached statistical significance as being more likely associated with oncologic/hematologic disease. Although these findings are important, the small sample size does not allow firm conclusions to be drawn. The utility of obtaining a differential WBC count is highlighted by the obser vation that leukopenia and neutropenia do not always track together. The patients diagnosed with leukemia were all significantly neutropenic, all with ANCs of 30 or less, and two thirds were leukopenic. The patients diagnosed with chronic neutropenia had ANCs between 268 and 726; none were leukopenic. All 3 of the patients diagnosed with leukemia had other evidence of bone marrow suppression with at least one other cell line affected. Our study results cor responded with those of other au- thors that the most common infections in patients with neutropenia include infections of the skin, mucous membranes, lungs, labia, gingivitis, and bacteremia with S. aureus and gram-negative organisms.1,15 Neither leukopenia nor neutropenia in and of itself was associated with sepsis in our study. All patients with bacteremia except one presented with toxicity and were hospitalized. The exception was the child with N. meningitidis bacteremia who suffered no significant morbidity after admission. Limitations Several limitations of this study must be addressed. The computerized data set used for the laborator y values may not have included all possible patients. The number of patients with initial neutropenia or chronic neutopenia may have been underestimated because not all patients in this sample had an initial ANC performed (n=11). There is also the possibility that the number of patients with chronic neutropenia may have been underestimated because only 58% had documentation of a repeat CBC and differential in the following month. Because medical follow-up was limited to our institution, the potential morbidity within the following month may have underestimated the potential longer term morbidity if patients had presented to another institution. We are not aware of any cases in which this occurred. Conclusions The prevalence of positive blood culture results in this study population was comparable to the SEPTEMBER 2005 CLINICAL PEDIATRICS Downloaded from cpj.sagepub.com at PENNSYLVANIA STATE UNIV on September 21, 2016 599 Ser wint et al. prevalence reported in studies of populations not selected for low WBC count. A number of patients with significant disease were recognized on clinical grounds of toxicity or physical findings. All patients eventually diagnosed with leukemia had involvement of at least one additional cell line besides their WBC count. Although our sample size was small, oncologic/hematologic disease was associated with more severe leukopenia and /or neutropenia, but infectious disease and bacteremia was not. Implications In the majority of cases of febrile patients with leukopenia and/or neutropenia, clinical judgment, physical findings, and review of all cell lines of the CBC will identify patients with significant disease. We recommend close follow-up with repeat CBC and differential in patients who do not have obvious significant disease at the time leukopenia and/or neutropenia is first documented. These recommendations, from this study of febrile children presenting to an ambulatory setting, are consonant with the recommendations from other authors.16,17 Suggested Approach to Neutropenia If a patient has an ANC less than 1000/mm3, a manual differential should be obtained to determine whether blasts or immature neutrophils are present. If the neutropenia occurs shortly after a presumed viral infection, a repeat CBC with differential 600 should be repeated 3 to 4 weeks later to allow assessment of recovery of the ANC. If recovery has not occurred, further evaluation is required. If a patient is noted to have leukopenia and/or neutropenia and signs of a serious infection, toxicity, gingivitis, or a skin infection, then a more aggressive workup may be warranted. REFERENCES 1. Boxer LA, Blackwood RA. Leukocyte disorders: quantitative and qualitative disorders of the neutrophil, part 1. Pediatr Rev. 1996;17(1):19-28. 2. Roskos RR, Boxer LA. Clinical disorders of neutropenia. Pediatr Rev. 1991; 12(7):208-212. 3. Baraff LJ, Bass JW, Fleischer GR, et al. Practice guidelines for the management of infants and children 0 to 36 months of age with fever without source. Pediatrics. 1993;92(1):1-12. 4. Bonadio WA, Stremski E, Shallow K. Clinical characteristics of children with fever and transient neutropenia who experience serious bacterial infections. Pediatr Emerg Care. 1989; 5(3):163-165. 5. Petrilli AS, Melaragno R, Barros KVT, et al. Fever and neutropenia in children with cancer: a therapeutic approach related to the underlying disease. Pediatr Infect Dis J. 1993; 12:916-921. 6. Alario AJ, O’Shea JS. Risk of infectious complications in well-appearing children with transient neutropenia. AJDC. 1989;143:973-976. 7. Bowden R, Hays T, Hathaway WE. Neutropenia in the pediatric population and its association with infection. Pediatr Res. 1984;18:236A. 8. Kuppermann N. Occult bacteremia in young febrile children. Pediatr Clin North Am. 1999;46(6):1073-1109. 9. Kupperman N, Malley R, Inkelis SH, et al. Clinical and hematologic features do not reliably identify children with unsuspected meningococcal diseases. Pediatrics. 1999;103:1-6. 10. Dagnew H, Reising S, Christie C. Occult meningococcal disease in children, 1983–1995: Subtle presentation and outcome with and without antibiotics. Presented at the 36th Interscience Conference on Antimicrobial Agents and Chemotherapy, 274A, 1996. 11. Dashefsky B, Teele DW, Klein JO. Unsuspected meningococcemia. J Pediatr. 1983;102:69-72. 12. Sullivan TO, LaScolea LJ JR. Neisseria meningitides bacteremia in children: quantitation of bacteremia and spontaneous clinical recovery without antibiotic therapy. Pediatrics. 1987;80:6367. 13. McCarthy PL, Grundy G, Spiesel SZ, Dolan TF. Bacteremia in children. An outpatient clinical review. Pediatrics. 1976;57:861-869. 14. Fleischer CR, Rosenberg N, Vinci R, et al. Intramuscular versus oral antibiotic therapy for the prevention of meningitis and other bacterial sequelae in young febrile children at risk for occult bacteremia. J Pediatr. 1994; 124:504-512. 15. Jonsson OG, Buchanan GR. Chronic neutropenia during childhood: a 13 year experience in a single institution. AJDC. 1991;145:232-235. 16. Alario AJ. Management of the febrile, other wise healthy child with neutropenia. Pediatr Infect Dis J. 1994; 13(2):169-170. 17. Bonadio WA, Smith DS, Mathews S, Rock AL. Clinical significance of newly documented neutropenia in febrile young infants evaluated for sepsis. Pediatr Infect Dis J. 1991;10 (5):407. SEPTEMBER 2005 CLINICAL PEDIATRICS Downloaded from cpj.sagepub.com at PENNSYLVANIA STATE UNIV on September 21, 2016