Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
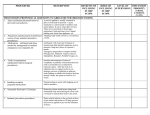
Professional Relations Dept. 601 S.W. Second Avenue Portland, OR 97204-3156 503-243-3965 (fax) www.odscompanies.com Survey of Charges–Oral Surgery This survey represents the most frequently billed procedure codes. DIAGNOSTIC D7280 $_________ CLINIC ORAL EVALUATIONS D0140 $_________ D0150 $_________ D0484 $_________ D0485 $_________ Limited oral evaluation Comprehensive oral evaluation Consultation on slides prepared elsewhere Consultation, including preparation of slides from biopsy material supplied by referring source RADIOGRAPHS D0210 $_________ D0330 $_________ $_________ $_________ $_________ D7285 $_________ D7286 $_________ D7310 $_________ D7311 $_________ D7320 $_________ Intraoral-complete series Panoramic film Additional codes _____ _____ _____ D7283 $_________ ______________________________ ______________________________ ______________________________ D7321 $_________ D7471 $_________ D7510 $_________ D7511 $_________ ORAL SURGERY D7953 $_________ EXTRACTIONS (INCLUDES LOCAL ANESTHESIA, SUTURING, IF NEEDED, AND ROUTINE POSTOPERATIVE CARE D7960 $_________ D7111 $_________ D7140 $_________ Coronal remnants-deciduous tooth Extraction, erupted tooth or exposed root (elevation and/or forceps removal) SURGICAL EXTRACTIONS (INCLUDES LOCAL ANESTHESIA, SUTURING IF NEEDED, AND ROUTINE POSTOPERATIVE CARE) D7210 $_________ D7220 $_________ D7230 $_________ D7240 $_________ D7250 $_________ Surgical removal of erupted tooth requiring elevation of mucoperiosteal flap and removal of bone and/or section of tooth Removal of impacted tooth-soft tissue Removal of impacted tooth-partially bony Removal of impacted tooth-completely bony Surgical removal of residual tooth roots (cutting procedures) OTHER SURGICAL PROCEDURES D7260 $_________ D7270 $_________ (1/13/05) Oroantral fistula closure Tooth reimplantation and/or stabilization of accidentally evulsed or displaced tooth and/or alveolus D7963 $_________ D7970 $_________ Surgical exposure of impacted or unerupted tooth for orthodontic reasons (including orthodontic attachments) Placement of device to facilitate eruption of impacted tooth Biopsy of oral tissue-hard (bone) Biopsy of oral tissue-soft (all others) Alveoloplasty in conjunction with extractions -per quadrant Alveoloplasty in conjunction with extractions - one to three teeth or tooth spaces Alveoloplasty not in conjunction with extractions-per quadrant Alveoloplasty not in conjunction with extractions -one to three teeth or tooth spaces Removal of exostosis-per site Incision and drainage of abscess-intraoral soft tissue Incision and drainage of abcess-intraoral soft tissue Bone replacement graft for ridge preservation-per site Frenulectomy (frenectomy or frenotomy)-separate procedure Frenuloplasty Excision of pericoronal gingiva Additional codes _____ _____ _____ $_________ $_________ $_________ ______________________________ ______________________________ ______________________________ ADJUNCTIVE GENERAL SERVICES D9110 $_________ D9220 $_________ D9241 $_________ Palliative (emergency) treatment of dental pain-minor procedure General anesthesia-first 30 minutes Intravenous sedation/analgesia-first 30 minutes Additional codes _____ _____ _____ $_________ $_________ $_________ ______________________________ ______________________________ ______________________________ *** If you practice at more than one office, you must submit fee filings for each location.*** Please print or type Name ________________________________________ Office Address ________________________________ TIN #________________________________________ License Number ____________________________ City ________________ Zip ______________ Telephone ________________________________ Fax # I certify that these are the fees I intend to charge my patients. I agree these fees and any future fees will not be used on treatment forms until I have received notification from ODS of acceptance of all fees listed on this form. Signature_________________________________ Date_____________ Specialty________________________