Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Special needs dentistry wikipedia , lookup
Forensic dentistry wikipedia , lookup
Water fluoridation in the United States wikipedia , lookup
Water fluoridation wikipedia , lookup
Fluoride therapy wikipedia , lookup
Scaling and root planing wikipedia , lookup
Focal infection theory wikipedia , lookup
Endodontic therapy wikipedia , lookup
Periodontal disease wikipedia , lookup
Crown (dentistry) wikipedia , lookup
Remineralisation of teeth wikipedia , lookup
Impacted wisdom teeth wikipedia , lookup
Dental emergency wikipedia , lookup
Tooth whitening wikipedia , lookup
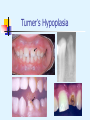
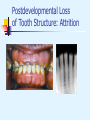
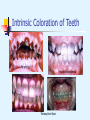
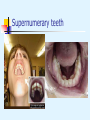
Abnormalities of the Teeth Environmental Effects on Tooth Structure Development Environmental Effects on Tooth Structure Development Visible environmental enamel defects can be classified into one of three patterns: Enamel hypoplasia – pits, grooves, or larger areas of missing enamel Diffuse opacities of enamel – variations in translucency or normal thickness; increased white opacity with no clear boundary with adjacent normal enamel Demarcated opacities of enamel show areas of decreased translucence, increased opacity, and a sharp boundary with adjacent enamel; normal thickness Environmental Effects on Tooth Structure Development Common pattern occurs as result of systemic influences (such as exanthematous fevers) which occur during the first two years of life; horizontal rows of pits or diminished enamel on anterior teeth and first molars; enamel loss is bilateral Similar pattern in cuspids, bicuspids, and second molars when the inciting event occurs at age 4-5 Enamel Hypoplasia associated with exanthematous fevers Turner’s Hypoplasia (1) Secondary to periapical inflammatory disease of the overlying deciduous tooth Enamel defects vary from focal areas of white, yellow or brown to extensive hypoplasia involving the entire crown. Most frequently affects permanent bicuspids Traumatic injury to deciduous teeth also causes Turner’s teeth (45% of children sustain injuries to primary teeth) Turner’s Hypoplasia (2) Trauma can displace the already formed hard tooth substance in relationship to the remaining soft tissue for root formation causing dilaceration (a bend in the tooth root) Severe trauma early in tooth development can cause disorganization of the bud resembling a complex odontoma. Severe trauma later on can lead to partial or total arrest of root formation. Turner’s Hypoplasia Turner’s Hypoplasia Hypoplasia Caused by Antineoplastic Therapy Degree and severity related to age, form of therapy (chemotherapy/radiotherapy) and dose Defects include hypodontia, microdontia, radicular hypoplasia, enamel hypoplasia and discolorations Radiotherapy effects more severe than chemotherapy alone but sometimes used together Dose of radiation as low as 0.72 Gy can cause mild defects in enamel/dentin Mandibular hypoplasia due to direct radiation, alveolar deficiency or pituitary effects. Hypoplasia Caused by Antineoplastic Therapy Dental Fluorosis Critical period is age 2-3, if fluoride levels greater than 1 part per million are ingested Fluoride comes from several sources besides water: adult-strength fluoride toothpastes, fluoride supplements, infant foods, soft drinks, and fruit juices Severity is dose dependent (higher intakes during critical periods associated with more severe fluorosis) Dental Fluorosis Dental fluorosis Syphilitic Hypoplasia Mulberry molars – constricted occlusal tables with disorganized surface anatomy resembling surface of a mulberry Anterior teeth called Hutchinson’s incisors, have crowns shaped like straight-edge screwdrivers; incisal taper & notch Treatment - Most are cosmetic problems; treatment includes acid-etched composite resin restorations, labial veneers, and full crowns Hutchinson’s triad Syphilitic Hypoplasia Moon’s (mulberry) molars Hutchinson’s incisors Postdevelopmental Loss of Tooth Structure: Attrition Loss of tooth structure caused by tooth-to-tooth contact during occlusion and mastication. Pathologic when it affects appearance and function. Process can be accelerated by poor quality or absent enamel, premature edge-to-edge occlusion, intraoral abrasives, erosion, and grinding habits. Attrition Can occur in deciduous and permanent dentitions Most frequently, incisal and occlusal surfaces involved Large flat wear facets found in relationship corresponding to pattern of occlusion Interproximal contact points also affected Over time, interproximal loss can result in shortening of arch length Postdevelopmental Loss of Tooth Structure: Attrition Postdevelopmental Loss of Tooth Structure: Abrasion Pathologic loss of tooth structure secondary to the action of external agent Most common source is tooth brushing with abrasive toothpaste and horizontal strokes. Also pencils, toothpicks, pipe stems, bobby pins, chewing tobacco, biting thread, inappropriate use of dental floss Abrasion Variety of patterns, depending on the cause Toothbrush abrasion presents as horizontal cervical notches on buccal surface of exposed radicular cementum and dentin; degree of loss greatest on prominent teeth Thread-biting, pipe stem, bobby pins etc., produce rounded or V-shaped notches in incisal edges of anterior teeth Dental floss, toothpicks result in loss of interproximal radicular cementum and dentin Abrasion Abrasion Abrasion from partial clasp Abrasion from improper flossing Postdevelopmental Loss of Tooth Structure: Erosion Loss of tooth structure by chemical reaction, not that associated with bacteria (caries) Secondary to presence of acid or chelating agent Source can be dietary (e.g., vinegar, lemons), internal (gastric secretions – perimolysis), or external (e.g., acids, industrial, atmosphere) “If it is not abrasion or attrition, it must be erosion” Erosion Commonly affects facial surface of maxillary anteriors and appears as shallow spoon-shaped depressions in cervical portion of the crown Posterior teeth exhibit loss of occlusal surface, where dentin is destroyed more rapidly than enamel, resulting in concave depression of dentin surrounded by elevated rim of enamel Erosion limited to facial surfaces of maxillary anterior dentition is usually associated with dietary acid. Erosion Tooth loss confined to incisal portions of anterior dentition of both arches indicates environmental source. Erosion on palatal surfaces of maxillary anterior teeth and occlusal surfaces of posterior teeth of both dentitions probably caused by regurgitation of gastric secretions. Erosion Fizzy Drinks Are Major Cause of Teen Tooth Erosion Thu Mar 11, 7:06 PM ET LONDON (Reuters) - Fizzy drinks are the major cause of tooth erosion in British teenagers but many parents are not aware of the problem, researchers said on Friday. The sodas and pop drunk by up to 92 percent of UK 14-year-olds wear away the enamel protective coating on teeth. Dental erosion weakens teeth and can cause thinning or chipping of the tooth edges. "This research identifies fizzy drink as by far the biggest factor in causing dental erosion among teenagers," said Dr Peter Rock, of Birmingham University. "Drinking fizzy drinks only once a day was found to significantly increase a child's chances of suffering dental erosion," he added. Drinking four or more glasses of fizzy drinks a day raises a 12-year-old's chances of suffering from tooth erosion by 252 percent. Heavy consumption in 14-year-olds increased the risk to 513 percent, according to research published in The British Dental Journal. Unlike tooth decay, which results from high levels of sugar, erosion is caused by acidic substances in the drinks. Even diet versions are harmful. Drinking milk and water, instead, reduces the risk. "Erosion is a growing problem among British teenagers, yet many parents don't understand the difference between decay and erosion," said Professor Liz Kay of the British Dental Association. "Parents need to understand...it is the acidity of certain products that cause erosion," she added in a statement. Erosion Postdevelopmental Loss of Tooth Structure: Abfraction Loss of tooth structure resulting from repeated tooth (enamel & dentin) flexure produced by occlusal stresses Disruption of chemical bonds at cervical fulcrum leads to cracked enamel that can be vulnerable to abrasion and erosion Abfraction Wedge-shaped defects limited to cervical area Deep, narrow, V-shaped Sometimes single tooth or subgingival More common in mandibular dentition and among those with bruxism Abfraction Treatment of Postdevelopmental Loss of Tooth Structure Early diagnosis and intervention to restrict severity of tooth loss Patient education Mouth guards Limit (redirect) tooth brushing & flossing Replacement of lost posterior teeth and avoidance of edge-to-edge occlusion Composite resins, veneers, onlays, full crowns Internal & External Resorption Internal resorption is caused by cells located in dental pulp. Rare, usually follows injury to pulpal tissues. External resorption is caused by cells in the periodontal ligament. Most patients are likely to have root resorption on one or more teeth. Internal Resorption Internal resorption presents as a uniform, well-circumscribed symmetrical radiolucent enlargement of pulp chamber. When it affects the coronal pulp, crown can display pink discoloration (pink tooth of Mummery) External resorption External resorption presents with a “moth-eaten” loss of root structure in which radiolucency is less well-defined and demonstrates variations in density. Most cases of external resorption involve apical or mid-portions of root Internal & External Resorption Cervical pattern of external resorption is often rapid (invasive resorption) Multiple idiopathic root resorption – involves several teeth, underlying cause not obvious Treatment involves the removal of all soft tissue from sites of dental destruction. For external resorption, determine if an accelerating factor is present, and eliminate it. Internal & External Resorption External Resorption Internal resorption → → Internal resorption External resorption-embedded tooth Environmental Discoloration of Teeth Environmental Discoloration of Teeth: Extrinsic Arise from surface accumulation of exogenous pigment Bacterial stains – occur most frequently in children Excessive use of tobacco, tea, coffee Foods that contain abundant chlorophyll Restorative materials, especially amalgam Medications Stannous fluoride and chlorhexidine Extrinsic stains can be removed by polishing with fine pumice, (sometimes with added 3% hydrogen peroxide); recurrence is likely unless the associated cause is altered Environmental Discoloration of Teeth: Extrinsic Amalgam stain Tobacco stain Environmental Discoloration of Teeth: Intrinsic Secondary to endogenous factors that discolor underlying dentin Congenital erythropoietic porphyria (Günther’s disease) is an AR disorder of metabolism that results in increased synthesis and excretion of porphyrins Hyperbilirubinemia due to jaundice, erythroblastosis fetalis (hemolytic anemia of newborns secondary to blood incompatibility, usually Rh factor), biliary atresia (sclerosing process of the biliary tree), and chlorodontia (green discoloration). Environmental Discoloration of Teeth: Intrinsic Localized red blood cell destruction (pink discoloration arising from hemoglobin breakdown within necrotic pulp tissue when blood has accumulated in the head) Lepromatous leprosy (pink discoloration secondary to infection-related necrosis and the rupture of numerous small blood vessels within the pulp Medications (tetracycline) Intrinsic stains are difficult to treat. Possible treatments include full crowns, external bleaching of vital teeth, internal bleaching of nonvital teeth, bonded restorations, composite build-ups, and laminate veneer crowns. Intrinsic Coloration of Teeth Porphyria Hyperbilirubinemia Tetracycline Stain Localized Disturbances in Eruption Localized Disturbances in Eruption Eruption – the continuous process of movement of a tooth from developmental location to functional location Impacted – teeth that cease to erupt due to physical obstruction Embedded – teeth that cease to erupt due to lack of eruptive force Ankylosis – teeth that cease to erupt due to anatomic fusion of tooth with alveolar bone Localized Disturbances in Eruption Primary impaction of deciduous teeth is extremely rare. Most commonly involves second molars often due to ankylosis. Primary impaction of permanent teeth most frequently affects third molars. Lack of eruption is most often related to crowding and insufficient maxillofacial development. Impacted teeth are frequently diverted or angulated, eventually losing their potential to erupt; mesioangular, distoangular, vertical, horizontal and inverted Localized Disturbances in Eruption Treatment includes long-term observation, orthodontic-assisted eruption, transplantation, or surgical removal Risks associated with both intervention and nonintervention Surgical removal of impacted teeth is the procedure most frequently performed by OMFS Localized Disturbances in Eruption Ankylosis – cessation of eruption after emergence Usually develops between ages 7-18; peak 8-9; prevalence est. 1.3-8.9% Fails to respond to orthodontic therapy Failure to treat can result in tilting, carious destruction, and periodontal disease When successor tooth present, best treated with extraction and space maintenance Localized Disturbances in Eruption Primary tooth impaction Mesioangular impaction Ankylosis Developmental Alterations of the Teeth Developmental Alterations in the Number of Teeth Anodontia – total lack of tooth development. Rare; most cases occur in hereditary hypohidrotic ectodermal dysplasia Hypodontia – lack of development of one or more teeth. Uncommon in deciduous teeth, usually involves mandibular incisors. More common in permanent teeth, third molars most affected. More frequent in females than males Oligodontia – lack of development of six or more teeth Developmental Alterations in the Number of Teeth Hyperdontia – development of increased number of teeth. Additional teeth are supernumerary. Prevalence 1-3%. More common in males and usually develops by age 20. Maxilla is most common site (90%) for single tooth hyperdontia, especially incisor region (mesiodens) Most single supernumerary teeth are unilateral. Nearly 75% of supernumerary teeth in anterior maxilla fail to erupt Non-syndromic multiple supernumerary teeth occur mostly in mandible. Hypodontia (oligodontia) Example of pedigree Hypodontia in Ectodermal Dysplasia Developmental Alterations in the Number of Teeth Mesiodens – supernumerary tooth in maxillary anterior incisor region Distomolar/Distodens – accessory fourth molar Paramolar – posterior supernumerary tooth situated lingually or buccally to a molar tooth Dental transposition – normal teeth erupted in an inappropriate pattern Natal teeth – teeth present in newborns; teeth arising during the first 30 days of life; (85% mandibular incisor region) Hyperdontia (supernumeray teeth) Mesiodens Cleidocranial dysplasia Supernumeray premolar Transposition (canine-first premolar) Treatment of Developmental Alterations in the Number of Teeth Hypodontia – often no treatment required for individual missing teeth; prosthetic replacement for multiple missing teeth. Hyperdontia – early removal of accessory tooth; delayed in therapy can delay eruption of adjacent teeth or cause displacement. Natal teeth – may be removed if they are loose; if stable, they should be retained; Riga-Fede disease (ulceration of ventral tongue associated with breastfeeding) can often be treated without removal of the teeth. Natal teeth (Riga-Fede syndrome) Supernumerary teeth Mesiodens Mesiodens Supernumerary premolar Supernumerary teeth Supernumerary teeth Supernumerary teeth in cleidocranial dysplasia syndrome Developmental Alterations in the Size of Teeth Developmental Alterations in the Size of Teeth (1) Microdontia – small teeth. Can also be related to tooth size relative to jaw size. More common in females. Isolated microdontia within otherwise normal dentition is not uncommon (peg-shaped lateral 0.8-8.4%). Diffuse microdontia occurs in some hereditary disorders and sometimes associated with hypodontia. Increased in Down’s, pituitary dwarfism & a few other syndromes. Macrodontia – larger than average teeth. More common in males. Typically only a few teeth are abnormally large. Diffuse macrodontia may occur in pituitary gigantism. It can be associated with hyperdontia. Microdontia “peg-shaped” laterals “paramolar” Developmental Alterations in the Size of Teeth (2) Macrognathia – normal sized teeth widely spaced in larger than normal jaw. Treatment – not necessary except for esthetic reasons Developmental Alterations in the Shape of Teeth Developmental Alterations in the Shape of Teeth Double teeth – two separate teeth exhibiting union by dentin and sometimes pulps (fusion). May result from fusion of two tooth buds, or partial splitting of one into two. Concrescence – union of two teeth by cementum without confluence of dentin. Gemination – single enlarged tooth or joined (double) tooth in which tooth count is normal when this tooth is counted as one. Fusion – single enlarged tooth or joined (double) tooth in which the tooth count is short one when this tooth is counted as one. Concrescence Gemination / Fusion → Fusion Gemination Dilaceration Abnormal angulation or bend in root (or commonly the crown) During tooth development, it is thought to arise following displacement injury or less frequently secondary to the presence of an adjacent cyst or tumor Treatment - minor dilaceration in permanent teeth requires no therapy; grossly deformed teeth should be removed; extraction of deciduous teeth when eruption is delayed. Dilaceration Supernumerary Roots Increased number of roots No treatment necessary, but detection of extra root critical for endodontic therapy or exodontia