Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
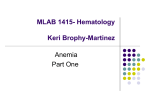
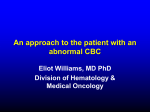
Case Challenge A 16-Year-Old Female with Anemia and a Dropping Platelet Count Ugoeze Otome, MD; and Lisa Giordano, MD A 16-year-old African-American female was referred for anemia and a dropping platelet count. Ferrous sulfate 325 mg orally three times per day had been initiated 3 days earlier. She gave a history of menorrhagia, headache, fatigue, and shortness of breath, intermittently, for 3 months. Her medical history was significant for anemia 2 years earlier, for which she was placed on oral iron but she was non-compliant. She denied any recent illness. Her gynecology/ obstetric history was notable for heavy menstruation since menarche at 14. Her usual menstrual pattern consisted of menses every 20 days, lasting 7 days with approximately five heavily soaked pads per day and cramping on the first day. She also had two episodes of light bleeding lasting about 2 days in between her last two menstrual periods. She denied other systemic bleeding symptoms. Medications at presentation included acetaminophen or Ugoeze Otome, MD, is a general pediatrician, Potomac Valley Family Medicine, Moorefield, WV. Lisa Giordano, MD, is Section Head of Pediatric Oncology, Division of Pediatric Hematology/ Oncology, John H. Stroger Jr. Hospital of Cook County. Address correspondence to Lisa Giordano MD, Division of Pediatric Hematology/Oncology, John H. Stroger Jr. Hospital of Cook County, 1900 West Polk Street, 11th Floor Pediatrics, Chicago, IL 60612; email: [email protected]. Disclosure: The authors have no relevant financial relationships to disclose. doi: 10.3928/00904481-20140825-05 354 ibuprofen for occasional headaches. There was no history of bleeding disorder or malignancy in the family. The patient’s mother also was diagnosed with anemia and was being treated with iron tablets. On examination, she was well appearing without distress. She had a temperature 98.8°F, heart rate of 131, respiratory rate of 24, blood pressure of 120/55 lying down and 101/61 sitting, with a body mass index of 27 kg/m2. Examination was significant for pallor, a flow murmur, and active heavy menstrual bleeding. There was no jaundice, lymphadenopathy, or organomegaly. Stigmata of polycystic ovarian syndrome, such as hirsutism and acne, were absent and there were no other abnormal findings. Prior to initiation of oral iron 3 days before presentation, hemoglobin was 5.0 g/ dL, mean corpuscular volume (MCV) was 63.9 fL, platelet count was 71 x 103/mm3, and white blood cell (WBC) count was 3.7 x 103/mm3 with a normal differential. Serum ferritin level was 2.4 ng/mL. Admission lab results included a negative urine pregnancy test, hemoglobin of 5.3 g/dL, MCV of 63.6 fL, red cell distribution width of 33.5%, platelet count of 27 x 103/mm3, WBC of 5.4 x 103/mm3 with a normal differential, and a reticulocyte count of 2.3% (see Table 1). Blood Figure 1. The patient’s peripheral blood smear after blood transfusion. type was O positive with a negative direct and indirect antiglobulin (Coombs) test. Serum creatinine was 0.6 mg/dL, total bilirubin 0.4 mg/dL, and lactate dehydrogenase 157 IU/L. Antinuclear antibody was negative and von Willebrand profile was normal. Hemoglobin electrophoresis revealed only low hemoglobin A2 level. Vitamin B12 and folic acid levels were normal. Analysis of the peripheral blood smear post-transfusion revealed two red blood cell populations with hypochromic microcytic erythrocytes, no schistocytes or blasts, and reduced platelets (Figure 1). Bone marrow studies revealed hypercellular trilineage hematopoiesis without increased blasts or stainable iron (Figure 2). For diagnosis, see page 355 Editor’s note: Each month, this department features a discussion of an unusual diagnosis. A description and images are presented, followed by the diagnosis and an explanation of how the diagnosis was determined. As always, your comments are welcome via email at [email protected]. Copyright © SLACK Incorporated Case Challenge Diagnosis: Thrombocytopenia Due to Severe Iron-Deficiency Anemia The patient received two units of leuko-reduced packed red blood cells upon admission (day 4 of oral iron therapy), which resulted in an increase in the hemoglobin to 7.5 g/dL. The platelet count increased to 33 x 103/mm3 then to 36 x 103/mm3 on the same day after transfusion of red cells (Table 1). Platelet transfusions were not administered at any time. The patient was evaluated by the gynecology service for menorrhagia. A pelvic ultrasound showed a thickened endometrial echotexture. A clinical diagnosis of dysfunctional uterine bleeding was made as the etiology for her menorrhagia, and therapy was initiated with oral contraceptives with one active tablet daily and instructions not to take the placebo tablets to prevent further bleeding. The patient was continued on ferrous sulfate and oral contraceptive therapy. She was discharged home and was followed closely in the outpatient hematology clinic. Ultimately, severe iron-deficiency anemia (IDA) secondary to dysfunctional uterine bleeding was confirmed, iron therapy was continued, and the patient’s hemoglobin and platelet count normalized (Table 2). DISCUSSION Thrombocytopenia is a rare complication of severe IDA. Our patient’s case was especially unusual because the platelet count continued to drop during the first few days of iron therapy. This observation raised the possibility of an alternative diagnosis, and a bone marrow examination and further investigations were performed. The differential diagnosis of anemia and thrombocytopenia in this patient at presentation included leukemia, which was ruled out by bone PEDIATRIC ANNALS • Vol. 43, No. 9, 2014 B A Figure 2. (A) The patient’s bone marrow iron stain, which revealed no stainable iron. (B) A control bone marrow iron stain (note the bluish discoloration). TABLE 1. Hematologic Parameters Prior to and During Admission Day 1 Pretreatment Day 1 on treatment Day 3 on treatment Day 4* on treatment Day 4† on treatment Hgb (g/dL) 5 5.5 5.3 5.9 7.5 MCV (fL) 63.9 64 63.6 67.7 70.4 RDW (%) 26.5 26.2 33.5 37.5 37.1 Platelets (x 10 /mm ) 71 43 27 33 36 WBC (x 103/mm3) 3.7 4.3 5.4 8.6 8.4 Reticulocyte count (%) 0.2 ND 2.3 ND ND 3 3 *After first red blood cell transfusion. †After second red blood cell transfusion and discharge day. Hgb = hemoglobin; MCV = mean corpuscular volume; ND = not done; RDW = red cell distribution width; WBC = white blood cell. marrow exam); autoimmune hemolytic anemia and immune thrombocytopenic purpura (ie, Evan’s syndrome), which was eliminated by the negative direct antiglobulin (Coombs) test and lack of evidence of hemolysis; and systemic lupus erythematosus, which was ruled out by the negative antinuclear antibody result. Hemoglobinopathy was ruled out by hemoglobin electrophoresis. The low hemoglobin A2 was consistent with IDA. Aplastic anemia was eliminated by the hypercellular bone marrow, and hemolytic uremic syndrome/thrombotic thrombocytopenic purpura was ruled out with a normal serum creatinine and lactate dehydrogenase, and a lack of schistocytes on the peripheral smear. An important potential etiology of menor- rhagia (von Willebrand disease) was eventually ruled out by a normal von Willebrand profile. The mechanism of thrombocytopenia associated with severe IDA is unknown. Suggested mechanisms in the literature include the existence of one or more irondependent cellular processes critical to the late stages of thrombopoiesis that can be altered during severe iron depletion.1-4 Also discussed is the stem cell competition/stem cell steal phenomenon based on evidence in animals that megakaryocytic and erythroid cell lineages share a common progenitor cell.2 Therefore, in IDA, an increase in erythroid precursors may result in a decreased number of megakaryocytes. However, this hypothesis was dismissed by Perlman et al.2 as they noted 355 Case Challenge TABLE 2. Hematologic Parameters During the Course of Ferrous Sulfate Therapy Day 1 Pretreatment Day 1 on Treatment Day 3 on Treatment Day 4* on Treatment Day 4† on Treatment Day 11 on Day 23 on Day 44 on Day 74 on Treatment Treatment Treatment Treatment Hgb (g/dL) 5 5.5 5.3 5.9 7.5 9.5 11.1 12.4 13 MCV (fL) 63.9 64 63.6 67.7 70.4 75 76.9 82 82.7 RDW (%) 26.5 26.2 33.5 37.5 37.1 39.7 33 26.1 15.5 Platelets (x 103/mm3) 71 43 27 33 36 696 393 183 181 3 WBC (x 10 /mm 3.7 4.3 5.4 8.6 8.4 9.6 5.7 5.4 5.1 Reticulocyte count (%) 0.2 ND 2.3 ND ND 6.1 1.5 0.5 0.7 3) *After first red blood cell transfusion. †After second red blood cell transfusion and discharge day. Hgb = hemoglobin; MCV = mean corpuscular volume; ND = not done; RDW = red cell distribution width; WBC = white blood cell. erythroid hyperplasia in two of three patients with IDA and an increase in megakaryocytes in all three patients with IDA who had a bone marrow examination. Our patient showed both erythroid hyperplasia and increased megakaryocytes on her bone marrow examination as well. Deficiencies of vitamin B12 or folic acid superimposed on severe IDA may cause thrombocytopenia; however, our patient had normal vitamin B12 and folic acid levels. Given the level of fortification of most food products in the United States, it is highly uncommon to see these vitamin deficiencies unless the patient is on a very restrictive diet. Another possibility is the effect of erythropoietin (Epo), which has been shown to be initially increased secondary to hypoxic stimuli in the setting of 356 severe anemia. Reports on the effect of Epo on thrombopoiesis5-7 document that an increased level of Epo in moderate IDA can stimulate megakaryopoiesis, whereas high levels of Epo may be associated with thrombocytopenia in severe IDA. Although Epo therapy often results in an increased platelet count initially, higher Epo doses have been shown to be associated with thrombocytopenia in humans and rats with chronic renal failure.5 Further study is necessary to elucidate the mechanism of thrombocytopenia in severe IDA. REFERENCES 1.Gross S, Keefer V, Newman AJ. The platelets in iron deficiency anemia. I. The response to oral and parenteral iron. Pediatrics. 1964;34:315-322. 2. Perlman MK, Schwab JG, Nachman JB, Ru- bin CM. Thrombocytopenia in children with severe iron deficiency anemia. J Pediatr Hematol Oncol. 2002;24:380-384. 3.Karpatkin S, Garg SK, Freedman ML. Role of iron as a regulator of thrombopoiesis. Am J Med. 1974;57(4):521-525. 4.Gupta MK, Joseph G. Severe thrombocytopenia associated with iron deficiency. Hosp Physician. 2001;54:49-51. http://www.turnerwhite.com/pdf/hp_aug01_iron.pdf. Accessed August 10, 2014. 5.Kadikoylu G, Yavasoglu I, Bolaman Z, Senturk T. Platelet parameters in women with iron deficiency anemia. J Natl Med Assoc. 2006;98(3):398-402. 6.Loo M, Beguin Y. The effect of recombinant human erythropoietin on platelet counts is strongly modulated by the adequacy of iron supply. Blood. 1999;93(10):3286-3293. 7. Beguin Y. Erythropoietin and platelet production. Haematologica. 1999;84:541-547. Copyright © SLACK Incorporated