Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
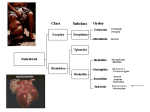
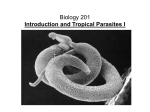
24.1 CHAPTER 24 Infections of the lymphatic system Wayne Melrose and John M. Goldsmid 24.1 INTRODUCTION The lymphatic system can be involved in a wide range of infectious conditions, viral, bacterial, mycotic and parasitic. Mostly this involvement is transient, the lymphatic system serving as part of the route utilized by micro-organisms in their spread throughout the body1. As such, enlargement of the lymph nodes may often reflect the spread of an infection from a local entry point1. However, in many infections the effect on the lymphatics may be both consistent and clinically marked. The lymphadenopathy may be local or generalized and lymphadenopathy is or can be a significant feature of acute HIV infection, primary Herpes simplex, some rickettsial infections, tularaemia, plague, cat-scratch fever due to Bartonella henselae, primary syphilis, lymphogranuloma venereum, chancroid, leptospirosis, brucellosis, relapsing fever, African trypanosomiasis (e.g. Winterbottom’s Sign), Chagas’ disease, and leishmaniasis2. Charters 3 also lists schistosomiasis (during the Katayama phase), paragonimiasis, onchocerciasis, trichinosis, leprosy, and sporotrichosis as causes of lymphadenopathy. However, the most significant and noteworthy involvement of the lymphatic system is seen in the Glandular Fever Syndrome and in Lymphatic filariasis. It is these two conditions, which will be dealt with in detail. 24.2 GLANDULAR FEVER SYNDROME The Glandular Fever Syndrome (GFS) has been overviewed by Mills and Goldsmid4 and is a condition characterised by fever, the presence of atypical lymphocytes in the peripheral blood, sore throat (often with exudate), splenomegaly, lymphadenopathy (local or generalised), liver dysfunction, malaise and sometimes a rash1,4,5. The infectious components of GFS comprise the Epstein Barr Virus (EBV) which specifically causes the condition of Infectious Mononucleosis, Cytomegalovirus (CMV), and the protozoan Toxoplasma gondii. Acute HIV may also present in this way. Of these causative organisms, EBV is the one most commonly associated with GFS – although in the tropics, infectious mononucleosis is not often seen and EBV is better known for it’s association with Burkitt’s lymphoma in Africa and Papua New Guinea and nasopharyngeal carcinoma in China and SE Asia. EBV infection can also be associated uncommon late tumours and with lymphoma in the immunologically compromised. It is believed that clinical Infectious Mononucleosis is rarely seen in the tropics due to infection occurring (mostly subclinically) at a very young age5. The effects of CMV and INFECTIONS OF THE LYMPHATIC SYSTEM 24.2 T. gondii on the foetus can be disastrous if a previously unexposed woman acquires the infection while pregnant. Of these organisms, EBV is transmitted by salivary exchange and kissing; CMV by intimate contact and crowding of young children which facilitates transmission and by sexual contact in adolescents and young adults; HIV sexually and T. gondii from eating vegetables or drinking water contaminated with the oocysts passed by cats or, more commonly, from the ingestion of intermediate hosts of the protozoan (mutton, pork, chicken and less commonly beef as well as a host of non-domesticated animals that might make up part of the diet in regional situations - see Chapter 4). Diagnosis of the GFS depends on the aetiological agent. Mostly, diagnosis is confirmed by antibody serology. Thus EBV infection is confirmed by specific antibody tests; heterophile antibody tests such as the Monospot Test, or by PCR. Treatment of IM and CMV is mostly supportive with bed rest, although Burkitt’s lymphomas and nasopharyngeal carcinomas respond well to standard antineoplastic drugs4. Aids can be treated as described in Chapter 9. Severe and clinically apparent T. gondii can be treated with sulphadiazine and pyrimethamine or spiramycin6-8 Clindamycin has also been found to be effective but should be reserved for cases of severe toxoplasmosis8. The dosages recommended are: 1) Pyremethamine: Adult: 25-100 mg/d orally for 3-6 weeks (Child: 1-2mg/kg/d orally up to 25mg for 3-6 weeks) + Sulphadiazine: Adult: 1 – 1.5g orally (or iv) qid for 3-6 weeks (Child: 50mg/kg orally up to adult dose.qid for 3-6 weeks) Folate supplements are usually added with this regimen. 2) Spiramycin (For pregnant women if needed or for patients sensitive to sulphas): Adult: 3-4g/d 3) Clindamycin: 600mg orally qid for 3-6 weeks. (Sheorey, Walker and Biggs (2000) in Clinical Parasitology, Melbourne University Press, also mention the use of albendazole as an alternative treatment for toxoplasmosis)) In ocular toxoplasmosis, corticosteroids should also be used. 24.3 FILARIAL INFECTIONS INVOLVING THE LYMPHATIC SYSTEM Filarial parasites (filaroids) are long hair-like tissue-dwelling nematodes. All except the Guinea worm Dracunculus medinensis (which uses a copepod) employ insects as intermediate hosts. They all have a similar life cycle that includes an obligatory maturation stage in a blood-sucking insect or a copepod, and a reproductive stage in the INFECTIONS OF THE LYMPHATIC SYSTEM 24.3 tissues or blood of a definitive host 9. A representative life cycle, Wuchereria bancrofti, is shown in Figure 24.1. Figure 24.1. Typical filaroid life cycle (CDC/DPDx, used with permission). (http://www.dpd.cdc.gov/dpdx) Adult male and female worms live in the lymphatics, skin, or other tissues. Microfilariae (which are specialised embryos not larvae) are produced by the female worm, circulate in the blood, (Figures 24.1, 24.2 and 24.3) or invade the skin, and are ingested by the vector where larval development, but not multiplication, occurs. The infective L3 stage migrates to the proboscis of the vector and is transmitted to the new host during feeding. Unlike malaria, the infective stage is not directly injected into the skin of the new host. They are deposited onto the skin whilst the mosquito is feeding and find their own way through the skin, usually via the puncture made by the mosquito. In Wuchereria bancrofti, Brugia malayi, B. timori and the subcutaneous species from West Africa (Loa loa), the microfilariae are surrounded by a sheath which appears as a pale, balloon-like structure in stained preparations. In the other species, the microfilariae INFECTIONS OF THE LYMPHATIC SYSTEM 24.4 are unsheathed. Figure 24.2. Microfilaria of W. bancrofti in thick blood film stained with Giemsa stain and showing the nuclear column (X200). Figure 24.3. Microfilaria of W. bancrofti in thin blood film attained with Giemsa stain and showing the sheath (X200) INFECTIONS OF THE LYMPHATIC SYSTEM 24.5 There are nine species of filaroid parasites that commonly cause human disease and their characteristics are summarised in Table 24.1 Species Disease Vector W. bancrofti Lymphatic filariasis “ “ Loiasis Mansonellosis Mosquito Brugia malayi Brugia timori Loa loa Mansonella perstans Mansonella ozzardi ____________ Mansonella streptocerca Onchocerca volvulus Dracunculus medinensis (Guinea worm) “ ____________ “ Onchocerciasis Dracunculiasis “ “ Chrysops fly Midges Location of adults Lymphatic system “ “ Migratory Serous cavities Location of microfilariae Blood Midge or Simulid fly ____________ Midge Thoracic or peritoneal cavities_______ ____________ Subcutaneous Skin Simulid blackfly Copepod Subcutaneous nodules Subcutaneous tissues “ “ “ Blood and serous effusions Blood Skin None. 1st stage larvae are liberated into water Table 24.1. The filaroid parasites of humans 24.3.1 Lymphatic filariasis Lymphatic filariasis is a mosquito-borne parasitic disease that is caused by three species of tissue dwelling filaroids: Wuchereria bancrofti is responsible for 90% of cases and is found throughout the tropics and in some sub-tropical areas world-wide. Brugia malayi is confined to Southeast and Eastern Asia. Brugia timori is found only in Timor and its adjacent islands. All three species cause similar disease. B. malayi is also found in monkeys, cats and other small animals but it is not known how important this is in the epidemiology of human disease. Unlike malaria where the only vectors are Anopheline mosquitoes, lymphatic filariasis can be transmitted by various species of the genera Anopheles, Culex, Aedes, Ochlerotatus, and Mansonia. The biting-time of the mosquito correlates with the periodicity of the microfilariae. In most parts of the world, the vectors are nocturnal feeders and the microfilariae exhibit nocturnal periodicity, where they are present in the blood in the greatest number around midnight. In areas such as the Central Pacific where the mosquito feeds during the day, there is a diurnal periodicity where the highest number of microfilariae occurs at midday. In some areas of Southeast Asia, a sub- INFECTIONS OF THE LYMPHATIC SYSTEM 24.6 periodic pattern is found, where some microfilariae are found in the blood at all times but there is a nocturnal peak. Lymphatic filariasis has a long history which reaches back into antiquity. Despite this, it has been a disease, which up to recent times, has been poorly understood and largely ignored by health authorities who are struggling to control what were perceived to be more important vector-borne diseases such as malaria and dengue fever. In the last two decades or so there has been a flurry of filariasis research, which has provided new insights into the global burden of filariasis, the pathogenesis and extent of filarial disease, diagnosis, and control 10,11. Lymphatic filariasis is classified by the World Health Organisation (WHO) as the second leading cause of permanent and long-term disability after mental illness 12. In addition to the physical problems, there are severe social and psychological consequences, especially in those who suffer from disfiguring complications such as elephantiasis or hydrocele 12-14. Lymphatic filariasis also has a huge economic impact upon endemic communities. In addition to the direct costs incurred in medical or surgical treatment, there are enormous indirect costs resulting from reduced work capacity and labour loss due to the frequency and severity of acute attacks and the disability due to chronic manifestations of the disease 12 .The total global burden of lymphatic filariasis is not known and mapping of its endemicity and prevalence is ongoing. Around 83 countries are known to be endemic but distribution mapping is continuing and more endemic areas are being identified. The most recent estimate puts the global burden at about 120 million 15. The true figures are certainly higher for Bancroftian filariasis because most country surveys done in the past were based on the demonstration of microfilariae. More recent surveys using antigen detection have shown that surveys of microfilaraemia alone can under-estimate the prevalence by as much as 30% 16. The WHO estimates that of that 120 million, 44 million have overt clinical disease – lymphodema, elephantiasis, and hydrocele. Another 76 million have covert, pre-clinical damage to their lymphatic and renal systems. Millions also suffer from debilitating acute attacks of filarial fevers and lymphadenitis 12. Until quite recently it was generally accepted that three groups of people are found in filarial- endemic areas: Those who are exposed, but with no evidence of disease - so called "endemic normals”, those with “asymptomatic microfilaraemia”, and those with “chronic pathology” - lymphodema, elephantiasis, or hydrocele. In some areas, most notably in Asia, another manifestation of filariasis arises - Tropical pulmonary eosinophilia 17-20. The term "endemic normal" is used to describe those who, despite constant exposure to filariasis, do not appear to become infected. Whether some of these people are truly immune to filariasis is debatable 21. Many of these so called "endemic normals" have a cryptic infection because they have circulating filarial antigen that is identical to that found in people with microfilaraemia 22, and ultrasound examination can detect adult worms in the scrotum of some “endemic normal” males 23,24. Asymptomatic microfilaraemia” is the most common manifestation of filariasis and this situation may persist for decades without progression to overt clinical disease. Recent studies prove that “asymptomatic microfilaraemia” is not a benign phase. Approximately half of the men with “asymptomatic microfilaraemia” have nests of motile adult worms in their scrotal lymphatics (the "filarial dance sign") and lymphoscintigraphy shows that their lymphatics INFECTIONS OF THE LYMPHATIC SYSTEM 24.7 are markedly dilated with collateral channelling and increased lymph flow 24-26. Another very important complication is renal dysfunction caused by direct mechanical damage to renal blood vessels by microfilariae, or by immune complexes being laid down in the kidney and manifesting as proteinuria and haematuria27-28. Like many other parasites, filaroids induce a degree of immunosuppression in their hosts as a means of ensuring their survival. The reduction in immune responses is not limited to filarial antigens alone and extends to a range of other antigens including tetanus toxoid 29,30, Salmonella typhi 29, H and O antigens of TAB vaccine 31, and purified protein derivative (tuberculin) 32,33. These findings strongly suggest that filarial infection may have an impact upon the efficacy of vaccination and further research is urgently required. 24.3.2 “Chronic filarial pathology.” Overall, hydrocele is the most common form of chronic Bancroftian filariasis and in parts of Africa it predominates. Hydrocele is said to have affected up to 70% of males along the Tanzanian coast and 60% of males in coastal Kenya by the time they reach age 70 years 34,35. Hydrocele can reduce work capacity, impair sexual activity and enjoyment, and cause severe psycho-social problems in affected males 14,,36-38. The most feared complications of lymphatic filariasis are chronic lymphodema and elephantiasis 12-14. In some populations, despite a high prevalence of microfilaraemia and filarial antigenaemia, filariasis is a mostly a cryptic disease and the number of people with elephantiasis is relatively low. For instance, the prevalence of filarial antigenaemia in many parts of Papua New Guinea is around 80% yet elephantiasis occurs only in scattered foci and is nowhere common 10. The first manifestation of impending elephantiasis is transient lymphodema which resolves with limb elevation. This is followed by persisting lymphodema, then fibrous infiltration and thickening of the skin with fissure and ulcer formation. The changes grow steadily worse until the limb becomes grossly swollen and hideously deformed, and normal function is impossible. The evolution of filarial infection and progression to chronic lymphodema and elephantiasis is not completely understood and is a complex interaction between transmission intensity, host and parasite immunobiology, in-utero exposure to parasite antigens, secondary infections (see below), and most probably host and parasite genetics. The shift from “asymptomatic microfilaraemia” to elephantiasis is accompanied by profound changes in cellular and humoral immunity. In microfilaraemics, most of the antifilarial antibody is of the IgG4 isotype with smaller amounts of IgG1, IgG2, IgG3 and IgE. In elephantiasis the proportion of IgG4 decreases and IgG1, IgG2, IgG3 and IgE increase. There is also an “awakening” of the previously suppressed cellular immune reactions to filarial and other antigens, but it is not clear whether the changes in the antibody profile and cellular immunity contribute to the pathology, or are the result of the pathology. 10,11. What is not in dispute is the role that acute attacks caused by secondary bacterial and fungal infections have in promoting the progression to elephantiasis. Active steps to improve hygiene, treat skin lesions with topical antibacterial and antifungal agents, aggressive antibiotic therapy of systemic infections, together with exercise and limb elevation can reduce the acute attacks, slow or prevent progression 40-42. An excellent practical handbook on the diagnosis, staging, and treatment of filarial lymphodema has been produced and should be on the bookshelf of everyone who cares for patients with lymphatic filariasis43. INFECTIONS OF THE LYMPHATIC SYSTEM 24.8 24.3.4 Acute filarial disease Acute filarial attacks can occur in both amicrofilaraemics and microfilaraemics, and are common in people with chronic filarial pathology 44. They can be extremely painful and debilitating and many people are confined to their houses and are unable to take part in productive activity. In some cases filarial infection markers such as filarial antigen and antifilarial antibody are absent. A possible explanation in these cases is an inflammatory response against in-coming L3 larvae before the adult worm has become established, but as yet there is no experimental evidence to support this hypothesis 45. Two distinct syndromes cause acute attacks 44. The first is called acute dermatolymphangioadenitis (ADLA), where there is development of a plaque-like lesion of cutaneous or subcutaneous inflammation. This may be accompanied by ascending lymphangitis and regional adenitis and typical systemic manifestation of bacteraemic such as chills and fevers are usually present. There is often oedema of the affected limb. This may completely or partially regress after the acute attack subsides but as noted above, recurrent ADLA is an important cause of chronic lymphodema. The other syndrome is called acute filarial lymphangitis (AFL) and is believed to be the result of an immunological reaction to dead or dying adult worms that have either been killed by the immune system or chemotherapy. In contrast to ADLA, AFL presents as a distinct wellcircumscribed nodule or cord and there may be local lymphadenitis with lymphangitis spreading in a centrifugal pattern i.e away from the inflamed lymph node. Fever is not usually present. These lesions can be extremely painful, and if they are the result of chemotherapy, can seriously compromise future compliance. Fortunately such occurrences are rare. Both ADLA and AFL can occur in the same patient. 24.3.5 Tropical Pulmonary Eosinophilia (TPE) TPE is most common in Southeast Asia and is at the opposite end of the immunological spectrum from asymptomatic microfilaraemia because it is the result of a hypersensitivity response to filarial antigens. There is marked eosinophilia, extreme levels of serum IgE, and high titres of antifilarial IgG and IgE 11,12. Circulating microfilariae are not usually found but adult worms may be detected by ultrasound 46. Clinically TPE is characterised by nocturnal coughing and asthma. Pulmonary infiltration gives rise to a characteristic xray picture called "snow flake" lung. Signs and symptoms resolve quite quickly after treatment with antifilarial drugs. 24.3.6 Other manifestations of lymphatic filariasis Chyluria, the passing of milky-coloured urine, is caused by leakage of lymph into the urinary tract is seen from time to time and is exacerbated by a high-fat diet and exercise. Filariasis can present with rheumatic features and mono-arthritis of a knee or ankle joint that resolves after antifilarial treatment is common in filarial-endemic areas, especially in children. Lymphatic filariasis has also been associated wide spectrum of other clinical signs and symptoms by various investigators. In some of these the connection is INFECTIONS OF THE LYMPHATIC SYSTEM 24.9 somewhat tenuous and a direct causal relationship between filarial infection and the other diseases have not been established 46-48. 24.3.7 Lymphatic filariasis in expatriates and travellers Because of its relatively ineffective transmission, lymphatic filarasis is seldom seen in in casual travellers or other people with short-term exposure to the parasite. Those who remain for longer periods in areas where transmission is intense are certainly at risk. A large number of cases occurred among American servicemen serving in the Central Pacific during World War 2 and other cases have occurred other military personnel, expatriate workers, Peace Corps volunteers, missionaries, and travellers 49-52. The clinical picture is that of acute filarial disease and microfilaraemia is extremely rare. The patient can present with a range of signs and symptoms such as malaise, transient fevers, lymphangitis, lymphadenopathy, skin rashes, and interestingly, episodic “black moods” or even clinical depression. Chronic pathology does not develop unless the person remains in the endemic area for many years. 24.3.8 Diagnosis of lymphatic filariasis Currently, four methods for diagnosis are currently in use: detection of microfilariae, detection of filarial antigen (only available for W. bancrofti), detection of specific antibodies and ultrasonic detection of adult worms. For microfilariae detection, blood is collected between 22:00 hours and midnight in areas where there is nocturnal periodicity and between 11:00 hours and midday where there is diurnal periodicity. It must be remembered that in lymphatic filariasis, the prepatent period - i.e. the time between infection and the appearance of the diagnostic stages of the parasite (the microfilariae), may be up to 12 months and is thus shorter than the incubation period (the time between infection and the appearance of clinical symptoms). For a parasitological diagnosis of lymphatic filariasis, the simplest method of detection is to take capillary blood from a finger-prick and make a thick film as for malaria diagnosis. Dry the film thoroughly, stain with Giemsa stain, and examine microscopically. A very useful variation is the “three line method” where, instead of the blood being spread over wide area, three lines of blood, each of 20µl are drawn on to the slide using a calibrated capillary tube. The microfilariae per 60µl of blood are counted and the number of microfilariae per ml of blood calculated. Thick film methods are relatively insensitive and will not detect low numbers of microfilariae, and in situations where that is important, venous blood should be obtained and a Knott’s concentration test done 53. This entails adding 1 ml of blood to 9 ml of 1% formaldehyde in water. The mixture is centrifuged and the deposit examined for microfilariae. A recent modification of the method allows for easier visualisation and counting of the microfilariae 54. Another widely used concentration method is the membrane filter technique whereby 1ml of blood that has been diluted in water is passed through a cellulose filter and the microfilariae are trapped on the cellulose. The filter is then removed from its holder, stained and examined microscopically 55. Other useful methods for the recovery of microfilariae from the blood include the microhaematocrit INFECTIONS OF THE LYMPHATIC SYSTEM 24.10 concentration technique 56 and the use of a cytocentrifuge if one is available 57. Staining blood films with Acridine Orange and examination under a UV microscope is another useful survey technique58. It is also worth noting that microfilariae of W. bancrofti can sometimes be found in the urines of patients presenting with chyluria. There are morphological differences between microfilariae of the three species and they can be distinguished by referring to the tables present in any book of human parasitology. Filarial antigen tests have revolutionised the diagnosis of Bancroftian filariasis since their introduction in the 1980’s and are now regarded as the “gold standard”. They are very sensitive and specific, and because they are not dependent upon the presence of microfilariae, blood can be taken at any time, and both microfilaraemic and amicrofilaraemic cases will be detected 11,59,60. Filarial antigen tests are available in both rapid card test and ELISA formats. The BINAX Filariasis NOW® rapid card test (also known as the ICT test) uses capillary blood and results are available almost immediately. This test is now the one of choice for community surveys and rapid assessment of filarial endemicity 61,62 but there needs to be careful adherence to reading times in order to get accurate results 63. The TropBio ELISA test (also known as the Og4C3 test) utilises serum and is very convenient for laboratory-based studies. It is slightly more sensitive than the rapid card test and provides a quantitative result 59,64,65. Antifilarial IgG4 antibody is produced in abundance during filarial infections and unlike broad-spectrum IgG antibody, shows little cross reaction with non-filaroid helminths 10,11. These antibodies are not species specific, and will not distinguish between aborted, cleared or patent infections, but a negative antibody test strongly suggests that filarial infection is extremely unlikely. A recently introduced antibody test called Brugia RAPID is showing great promise as a rapid screening test for Brugian filariasis where an antigen test is not available 66,67. PCR, and a number of other techniques are being evaluated for diagnosis but are not yet available for routine use 10,11. The use of ultrasound to detect living adult worms has been discussed earlier. In many patients with advanced elephantiasis all tests for lymphatic filariasis will be negative because they no longer have any living adult worms and reliance must be placed upon their clinical history and physical examination. The diagnosis of expatriate cases can be particularly difficult as they very seldom become microfilaraemic and there is little information on the value of filarial antigen tests in this setting. Filarial antibodies should be present but they make take some time to appear. If the patient has symptoms of acute lymphatic filariasis and tests are negative it may be worth considering still treating the patient and observing if the symptoms disappear. 24.3.9. Control and treatment of lymphatic filariasis In 1997, the World Assembly passed a resolution calling upon the elimination of lymphatic filariasis as a public health problem by 2020, and in 2000, a global elimination program was launched. The cornerstone of this program is the interruption of parasite transmission using annual, single-dose, community-wide mass drug administration (MDA)68. Currently, three drugs are used against lymphatic filariasis: diethylcarbamazine (DEC), ivermectin and albendazole. All three are very effective at clearing microfilariae and DEC and albendazole also have some effects on adult worms. Efficacy is enhanced when a combination of drugs is used. In areas where onchocerciasis and lymphatic INFECTIONS OF THE LYMPHATIC SYSTEM 24.11 filariasis are not co-endemic, DEC at 6mg/kg plus 400mg of albendazole is the combination of choice. In areas where lymphatic filariasis is co-endemic with onchocerciasis or loiasis, a combination of 400mg of albendazole and 400ug/kg body weight of ivermectin is used because DEC can cause severe reactions in patients with Onchocerca volvulus or Loa loa. 69-76. The safety and effectiveness of MDA has been proven to be effective in both Bancroftian and Brugian filariasis and elimination programs are underway in a number of countries 77-82. A community compliance level of at least 80% is required for the strategy to be effective and at least 5 annual rounds of treatment are required. An added advantage of using albendazole and ivermectin is their activity against soil-transmitted helminths 83. Although single-dose therapy has been shown to be efficacious in control programs, it is not yet recommended for the treatment of single patients who are generally given a dose of DEC at 6mg/kg every day for 12 consecutive days 84. Mild general side-reactions are common after anti-filarial treatment. Their severity tends to be proportional to the microfilarial density and they are more common and more severe in Brugian filariasis than in Bancroftian filariasis. Headache, body ache, malaise, fever, nausea, urticaria are the symptoms most commonly seen, and if they are of concern, the patient should be given analgesics. Local reactions tend to occur over, or near to, the site of adult worms and consist of lymphadenitis, funiculitis, epididymitis, orchitis, lymphangitis and transient lymphodema. Occasionally there may be painful nodule formation and even abscesses. Adverse reactions seldom last for more than three days. Severe adverse reactions that require hospitalisation are rare 81,84. The use of DEC-medicated salt is another control strategy that has been successfully used in several settings, most notably in China 10. Another promising chemotherapeutic strategy is the use of antibiotics to target the endosymbiont Wolbachia bacteria that live within some filaroids and are essential to the healthy growth and development of the parasite. The results obtained to date are very promising. Tetracycline, doxycyline and Rifamycin have been shown to inhibit the motility viability and release of microfilariae and impede their development 85,86. Control programs are very important, but those who have already developed chronic pathology should not be over looked. As mentioned earlier a lot can be done to alleviate the suffering caused by chronic lymphodema and elephantiasis and communities should be encouraged to institute active home-care programs. Hydrocele can be managed by surgery but re-occurrence can be a problem 87. The treatment for chyluria is rest and diet rich in protein but low in fat. Surgical intervention to disconnect the route between the leaking lymphatic vessel and the bladder has been tried in intractable cases 88. No proven prophylactic drugs are available for lymphatic filariasis although DEC is active against early stages of the parasite and is potentially effective. There is also a strong possibility that doxycycline, which is used for malaria prophylaxis, may also be effective against filarial worms by killing endosymbiont Wolbachia and research is urgently needed. 24.4 REFERENCES 1. Mims, C. et al . Medical Microbiology. 2nd Edition. London; Mosby. 1993 INFECTIONS OF THE LYMPHATIC SYSTEM 24.12 2. Wilson, M.E and Pearson, R.D. Practice: Approach to the patient. In: Essentials of Tropical Infectious Diseases. Guerrant, RL., Walker, DH and Weller, PF (Eds). N.Y. Churchill Livingstone. 2001. 3. Charters, A.D. Human Parasitology. Perth. Imperial Printing Co., 1983. 4. Mills, A.E. and Goldsmid, J.M. Intestinal protozoa. In: Tropical Pathology. 2nd edit., Doerr, W. and Siefert, G. (Eds). Berlin; Springer Verlag. pp 477-556. 1995. 5. Hudnall, S.D. Human herpesvirus infections. In: Essentials of Tropical Infectious Diseases. Guerrant, RL, Walker, DH and Weller, PF (Eds). N.Y. Churchill Livingstone. 2001. 6. Chin, J (Ed.) Control of Communicable Diseases Manual. Washington; APHA. 2000. 7. Bartlett, J.G. Pocket Book of Infectious Disease Therapy. Philadelphia. Lippincott, Williams and Wilkins. 2002. 8. Spicer, W.J. (Chairman). 2004. Therapeutic Guidelines: Antibiotic. Version 12. Melbourne; Therapeutic Guidelines Inc. 2004. 9. Roberts LS, Janovy J. Nematodes: Filaroidea, the filarial worms. In: Schmidt GD, Roberts LS. Foundations of Parasitology 5th. Edition, Boston. WCB Publishers. 1996. 10. Melrose W. Lymphatic Filariasis: A review 1862-2002. Warwick. Warwick Educational Publishing. http://www.wepi.org 11. Melrose WD. Lymphatic filariasis – new insights into an old disease. 2002; 32: 947960. 12. World Health Organisation. Lymphatic filariasis: reasons for hope. Geneva. WHO. 1997. 13. Bandyopadhyay L. Lymphatic filariasis and the women of India. Soc Sci Med 1996; 42: 1401-1410. 14. Dreyer G, Noroes J, Addiss D. The silent burden of sexual disability associated with lymphatic filariasis. Acta Trop 1997; 63: 57-60. 15. Michael E, Bundy DAP, Grenfell BT. Re-assessing the global prevalence and distribution of lymphatic filariasis. Parasitol 1996; 112: 409-428. 16. Turner PF, Copeman D, Gerisi D, Speare R. A comparison of the Og4C3 antigen capture ELISA, the Knott test, and IgG4 test and clinical signs in the diagnosis of Bancroftian filariasis. Trop Med Parasitol 1993; 44: 45-48. 17. Dasgupta A. Cursory overview of lymphatic filariasis. Ind J Pathol Microbiol 1984; 27: 273-280. 18. Ottesen EA. Filariasis now. Am J Trop Med Hyg 1989; 41: S9-S17. 19. Ottesen EA. Infection and disease in lymphatic filariasis: an immunologic perspective. Parasitol. 1992; 104: S71-S79. 20. Ottesen EA. Filarial infections. Infect Dis Clin Nth Amer 1993; 7: 619-633. 21. Kazura JW, Nutman TB, Greene BM. Filariasis. In: Immunology and Molecular Biology of Parasitic infections, 3rd edition. Warren KS. (Ed.) Boston; Blackwell Scientific Publications, Chapter 18. 1993. 22. Weil GJ, Ramzy RM, Chandrashekar R, Gad AM, Lourie RC, Faris R. Parasite antigenaemia without microfilaraemia in Bancroftian filariasis. Am J Trop Med Hyg 1996; 55: 333-337. 23. Dreyer G, Santos A, Noroes J, Rocha A, Addiss D. Amicrofilaraemic carriers of Wuchereria bancrofti. Trans R Soc Trop Med Hyg 1996; 90: 288-289. INFECTIONS OF THE LYMPHATIC SYSTEM 24.13 24. Amaral F, Dreyer G, Figueredo-Silva J, Noroes J, Cavalcanti A, Samico SC, Santos A, Coutinho A. Live adult worms detected by ultrasonography in human Bancroftian filariasis. Am J Trop Med Hyg 1994; 50: 753-757. 25. Noroes J, Addiss D, Santos A, Medeiros Z, Coutinho A, .Dreyer G. Ultrasonic evidence of abnormal lymphatic vessels in young men with adult Wuchereria bancrofti infection in the scrotal area. J Urol. 1996; 156: 409-412. 26. Ottesen EA. The human filariases: new understandings, new therapeutic strategies. Curr Opin Inf Dis 1994; 7: 550-558. 27. Langhammer J, Birk HW, Zahner H. Renal disease in lymphatic filariasis:evidence for tubular and glomerular disorders at various stages of infection. Trop Med Int Health 1997; 2: 875-884. 28. Dreyer G, Ottesen EA, Galdino E, Andrade L, Rocha A, Medeiros Z, Moura I, Casimiro I, Beliz F, Coutinho A. Renal abnormalities in microfilaraemic patients with Bancroftian filariasis. Am J Trop Med Hyg 1992; 46: 745-751. 29. Grove DI. Immuno-suppression in Bancroftian filariasis. Trans R Soc Trop Med Hyg 1979; 73: 23-26. 30. Nookala S, Srinivasan S, Kaliraj P, Narsyanan, RB, Nutman TB. Impairment of tetanus-specific cellular and humoral responses following tetanus vaccination in human lymphatic filariasis. Inf Immunity 2004; 72: 2598-2604. 31. Srivastava SK, Sabena RG, Bhutto B, Tandon A, Scrivastava BC, Sabena KC. Antibody response to TAB vaccine human filariasis - a preliminary communication. Ind J Med Res. 1981; 74: 524-526. 32. Malhotra I, Ouma J, Wamachi A, Kioko J, Mungai P, Omollo A, Elson L, Koech D, Kazura JW, King CL. In-utero exposure to helminth and mycobacterial antigens generates cytokine responses similar to that observed in adults. J Clin Invest 1997; 99: 1759-1766. 33. Malhotra I, Mungai P, Wamachi A, Kioko J, Ouma J, Kazura JW, King CL. Helminth and Calmette-Guerin-induced immunity in children sensitised in utero to filariasis and schistosomiasis. J Immunol 1999; 162: 6843-6848. 34. Wegesa P, McMahon JE, Abaru DE, Hamilton PJS, Marshall TF de C, Vauhan JP. Tanzania filariasis project: survey methodology and clinical manifestations of Bancroftian filariasis. Acta Trop 1979; 36: 369-377. 35. Estambale BBA, Simonsen PE, Knight R, Bwayo JJ. Bancroftian filariasis in Kwale district of Kenya 1. Clinical & parasitological survey in an endemic community. Ann Trop Med Parasitol 1994; 88: 145-151. 36. Mwobobia IK, Muniu EM, Kombe Y, Wamae CN. Hydrocelectomy: a proxy for hydrocele prevalence in coastal Kenya. Ann Trop Med Parasitol 2000; 94: 479-484. 37. Ahorlu CK, Dunyo SK, Asamoah G, Simonsen PE. Consequences of hydrocele and the benefits of hydrocelectomy: a qualitative study in lymphatic filariasis endemic communities on the coast of Ghana. Acta Trop 1999; 73: 251-261. 38. Shenoy RK. Management of disability in lymphatic filariasis – an update. J Comm Dis 2002; 34: 1-14. 39. Kazura JW, Spark R, Forsyth K, Brown G, Heywood P, Alpers M. Parasitologic and clinical features of Bancroftian filariasis in the Sepik Province of Papua New Guinea. Am J Trop Med Hyg 1984; 33: 1119-1123. INFECTIONS OF THE LYMPHATIC SYSTEM 24.14 40. Shenoy R, Kumaraswami V, Suma T, Rajan K, Radhakuttyamma G. A double blind, placebo-controlled study of the efficacy of oral penicillin, Diethylcarbamazine, or local treatment of the affected limb in preventing acute adenolymphangitis in lymphodema caused by Brugian filariasis. Ann Trop Med Parasitol 1999; 93: 367377. 41. Dreyer G, Noroes J, Figuerdo-Silva J. New insights into the natural history and pathology of bancroftian filariasis: implications for clinical management and filariasis control programmes. Trans R Soc Trop Med Hyg 2000; 94: 594-59. 42. Dreyer G, Noroes J, Figuerdo-Silva J, Piessens W. Pathogenesis of lymphatic disease in bancroftian filariasis: a clinical perspective. Parasitol Today 2000; 16: 544-548. 43. Dreyer G, Addiss D, Dreyer P, Noroes J. Basic Lymphodema Management: treatment and management of problems associated with lymphatic filariasis. Hollis Publishing, ISBN 1-884186-17-3. 44. Dreyer G, Medeiros Z, Nett M, Leal N, de Castro L, Piessens W. Acute attacks in the extremities of persons living in an area endemic for Bancroftian filariasis: differentiation of two syndromes. Trans R Soc Trop Med Hyg. 1999; 93: 413-417. 45. Addiss D, Eberhard M, Lammie P. "Filarial" adenolymphadenitis without filarial infection. Lancet 1994; 343: 597. 46. Dreyer G, Dreyer P, Piessens W. Extralymphatic disease due to Bancroftian filariasis. Braz J Med Biol Res 1999; 32: 1467-1472. 47. Adebajo AO. Rheumatic manifestations of tropical diseases. Curr Opin Rheumatol 1996; 8: 85-89. 48. Chaturvedi P, Harinath BC, Reddy MVR, Advani B, Gawdi A, Alikhan A, Rama Rao BV. Filarial antibody detection in suspected occult filariasis in children in an endemic area. J Trop Paediat 1995; 41: 243-245. 49. Wartman WB. Filariasis in American armed forces in World War 2. Medicine 1947; 26: 394. 50. McQuay R. Parasitological studies in a group of furloughed missionaries. Am J Trop Med Hyg . 1967; 16: 161-166. 51. Melrose W, Usurup, J, Pisters P, Turner P. Development of anti-filarial antibodies in a group of expatriate mine-site workers with varying exposure to the disease. Trans R Soc Trop Med Hyg 2000; 94: 706-707. 52. Leggat PA, Melrose W, Durrheim DN. Could it be Lymphatic Filariasis? J Travel Med. 2004; 11: 56-60. 53. Knott J. The periodicity of the microfilaria of Wuchereria bancrofti. Preliminary report of some injection experiments. Trans R Soc Trop Med Hyg 1935; 29: 59-64. 54. Melrose W, Turner P, Pisters, P, Turner B. An improved Knott’s concentration test for the detection of microfilariae. Trans R Soc Trop Med Hyg 2000; 94: 176. 55. Nathan MB, Lambourne A, Monteil S. Evaluation of a membrane (Nucleopore) filtration method using capillary blood for the detection of microfilariae. Ann Trop Med Parasitol 1982; 76: 339-345. 56. Goldsmid, J.M. The microhaematocrit centrifuge technique for the laboratory diagnosis of filarial infections. S.Afr. Med.J. 1972; 46: 171-174. 57. Goldsmid, J.M. and Rogers, S. The cytocentrifuge for the isolation of parasites from the blood. C. Afr. J. Med. 1975; 21: 160-161. INFECTIONS OF THE LYMPHATIC SYSTEM 24.15 58. Goldsmid, J.M., Rogers, S., Parsons, G.S. and Chambers, P.G. The use of Acridine Orange O in the laboratory diagnosis of human filariasis. C. Afr. J. Med. 1976; 22: 46. 59. Simonsen PE, Dunyo SK. Comparative evaluation of three new tools for diagnosis of bancroftian filariasis based on detection of specific antigens. Trans R Soc Trop Med Hyg 1999; 93: 278-282. 60. Melrose WD, Durrheim DN, Burgess GW. Update on immunological tests for lymphatic filariasis. Trend Parasitol 2004; 20: 255-257. 61. Weil GJ, Lammie PJ, Weiss N. The ICT filariasis test: a rapid-format antigen test for diagnosis of Bancroftian filariasis. Parasitol Today 1997; 13: 40-404. 62. Phantana S, Sensathein S, Songtrus J, Klagrathoke S, Phongnin. ICT filariasis test: a new screening test for bancroftian filariasis. Southeast Asian J Trop Med Pub Hlth 1999; 30: 47-51. 63. Simonsen PE, Magesa SM. Observations on flae positive reactions in the rapid NOW filariasis test. Trop Med Int Health 2004; 9: 1200-1202. 64. More SJ, Copeman DB. A highly specific and sensitive monoclonal antibody-based ELISA for the detection of circulating antigen in Bancroftian filariasis. Trop Med Parasitol 1990; 41: 403-406. 65. Chanteau S, Moulia-Pelat JP, Glaziou NL. Og4C3 circulating antigen: a marker of infection and adult worm burden in Wuchereria bancrofti filariasis. J Inf Dis 1994; 170: 247-250. 66. Rahmah N, Khairul Anuar A, Tengu Ariff, Zurainee MN, Noor A’shikin A, Fadzillah A, Maimunah A, Ashraful Haq J. Use of antifilarial IgG4 ELISA to detect Brugia malayi infection in an endemic area of Malaysia. Trop Med Int Health 1998; 3: 184-188. 67. Noordin R, Shenoy RK, Rahman RA. Comparison of two IgG4 assays formats for detection of Brugian filariasis. Southeast Asian J Trop Med Pub Health 2003; 34: 768-770. 68. Molyneux DH, Zagaria N. Lymphatic filariasis elimination: progress in global programme development. Ann Trop Med Parasitol 2002; 96: S15-40 69. Eberhard ML, Dickinson CM, Hightower AW, Lammie MJ. Bancroftian filariasis: long term effects of treatment with diethylcarbamizine in a Haitian population. Am J Trop Med Hyg 1991; 45: 728-733. 70. Addiss DG, Eberhard ML, Lammie PL. Comparative efficiency of clearing-dose and single high-dose ivermectin and diethylcarbamazine against Wuchereria bancrofti microfilaraemia. Am J Trop Med Hyg 1993; 48: 178-185. 71. Kazura J, Greenberg J, Perry R, Weil G, Day K, Alpers M. Comparison of singledose diethylcarbamazine and ivermectin for the treatment of Bancroftian filariasis in Papua New Guinea. Am J Trop Med Hyg 1993; 49: 804-811. 72. Ottesen EA, Ismail MM, Horton J. The role of albendazole in programmes to eliminate lymphatic filariasis. Parasitol Today 1999; 15: 382-386. 73. Addiss DG, Beach MJ, Streit TG, Lutwick S, LeConte FH, Lafontant JG, Hightower AW, Lammie PJ. Randomised placebo-controlled comparison of ivermectin and albendazole alone and in combination for Wuchereria bancrofti microfilaraemia in Haitian children. Lancet 1997; 350: 480-484. INFECTIONS OF THE LYMPHATIC SYSTEM 24.16 74. Ismail MM, Jayakody RL, Weil GJ, Nirmalan N, Jayasinghe KSA, Abeyewickrema W, Rezvi Sheriff MH, Rajaratnam HN, Amarasekera N, de Silva DCL, Michalski ML, Dissanaike AS. Efficacy of single dose combinations of albendazole, ivermectin and diethylcarbamazine for the treatment of Bancroftian filariasis. Trans R Soc Trop Med Hyg 1998; 92: 94-97. 75. World Health Organization. Training module on lymphatic filariasis for drug distributors in non-onchocerciasis co-endemic countries. Geneva; WHO, 2000. 76. World Health Organization The programme to eliminate lymphatic filariasis. Essential elements for medical personnel in onchocerciasis co-endemic countries. Geneva; WHO, 2000. 77. Hussein O, El Setouhy M, Ahmed E, Kandil A, Ramzy R, Helmy H, Weil G. Duplex dopler sonographic assessment of the effects of diethylcarbamazine and albendazole therapy on adult filarial worms and adjacent host tissues in Bancroftian filariasis. Am J Trop Med Hyg 2004; 71: 471-477. 78. Ismail MM, Jayakody RL, Weil GJ, Nirmalan N, Jayasinghe KSA, Abeyewickrema W, Rezvi Sheriff MH, Rajaratnam HN, Amarasekera N, de Silva DCL, Michalski ML, Dissanaike AS. Efficacy of single dose combinations of albendazole, ivermectin and diethylcarbamazine for the treatment of Bancroftian filariasis. Trans R Soc Trop Med Hyg 1998; 92: 94-97. 79. Pani SP, Subramanyam Reddy, Das LK, Vanamail P, Hoti SL, Ramesh J, Das PK. Tolerability and efficacy of single doses of albendazole, diethylcarbamazine (DEC) or co-adminstration of albendazole with DEC in the clearance of Wuchereria bancrofti in asymptomatic microfilaraemic volunteers in Pondicherry, South India: a hospital-based study. Filaria J. 2002; 1: 1-10. 80. El Setouchy M, Ramzy MR, Ahmed ES, Kandil AM, Hussain O, Farid H, Helmy H, Weil G. A randomised clinical trial comparing single and multi-dose combination therapy with diethylcarbamazime and albendazole for treatment of Bancroftian filariasis. Am J Trop Med Hyg 2004; 70: 191-196. 81. Supali T, Ismid I, Ruckert P, Fischer P. Treatment of Brugia timori and Wuchereria bancrofti infections in Indonesia using DEC or combination of DEC and albendazole: adverse reactions and short-term effects on microfilariae. Trop Med Int Hlth 2002; 7: 894-901. 82. Fischer P, Djurdi, Ismid I, Ruckert P, Bradley M, Supali T. Long-lasting reduction of Brugia timori microfilariae following a single dose of diethylcarbamazine combined with albendazole. Trans R Soc Trop Med Hyg 2003; 97: 466-448. 83. Mani TR, Rajendran R, Sunish IP, Munirathinam A, Araunachalam N, Satyanarayana K, Dash AP. Effectiveness of two annual, single-dose mass drug administrations of diethylcarbamazine alone or in combination with albendazole on soil-transmitted Helminths in filariasis elimination program. Trop Med Int Hlth 2004; 9: 1030-1035. 84. World Health Organisation. Control of lymphatic Filariasis: a manual for health personnel.Geneva: World Health Organisation, 1987. 85. Hoerauf A, Volkmann L, Hamelmann C, Adjei O, Autenrieth I, Fleischer B, Buttner DW. Endosymbiotic bacteria in worms as targets for a novel chemotherapy for filariasis. Lancet 2000; 355: 211-213. INFECTIONS OF THE LYMPHATIC SYSTEM 24.17 86. Hise AG, Gillette-Ferguson I, Perlman E. The role of endosymbiotic Wolbachia bacteria in filarial disease. Cell Microbiol 2004; 6: 97-104. 87. Albbrecht W, Holti W, Aharinejed S. Lord’s procedure – the best operation for hydrocele? Br J Urol 1991; 68: 187-189. 88. Karanjavala DK. Technique of clearance (or disconnection) of dilated lymphatics in the renal hilum and lower ureter and bladder in cases of chyluria or haemochyluria. Br J Urol 1979; 51: 440-442. □□□ Correspondence: Dr Wayne Melrose, DrPH, MPH&TM, BApplSc, ThDip, FACTM, FAIMS, MNZIMLS Acting Director, WHO Collaborating Centre for Control of Lymphatic Filariasis, Senior Lecturer, Anton Breinl Centre for Public Health and Tropical Medicine, James Cook University, 4811 Townsville, Queensland, Australia [email protected] Professor John M. Goldsmid, BSc (Hons), MSc, PhD, FRCPath, CBiol, FIBiol, FAIBiol FASM, Hon. FACTM, Hon. FRCPA Emeritus Professor of Medical Microbiology Discipline of Pathology University of Tasmania, 7000 Hobart, Tasmania, Australia [email protected] *** © Copyright 2005. All rights reserved, The Australasian College of Tropical Medicine Primer of Tropical Medicine Enquiries to: [email protected] *** INFECTIONS OF THE LYMPHATIC SYSTEM