Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
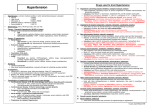
Paediatric Clinical Guideline Renal: 2.2 Hypertension Short Title: Hypertension Full Title: Guideline for the management of hypertension in children and young people Date of production/Last revision: May 2008 Explicit definition of patient group to which it applies: This guideline applies to all children and young people under the age of 19 years. Name of contact author Dr Simon Rhodes, Paediatric SpR Dr Damian Wood, Consultant Paediatrician Ext: 64041 Revision Date May 2011 This guideline has been registered with the Trust. However, clinical guidelines are 'guidelines' only. The interpretation and application of clinical guidelines will remain the responsibility of the individual clinician. If in doubt contact a senior colleague or expert. Caution is advised when using guidelines after the review date. Hypertension Definition(s) (See Appendix 1 for reference tables/data) Normal BP systolic and/or diastolic < 91st centile for age and sex Borderline 91st – 98th centile Hypertension ≥ 98th centile on at least 3 separate readings Severe Hypertension Symptomatic or >10mmHg above 98th centile 1 Simon Rhodes Page 1 March 2008 Paediatric Clinical Guideline Renal: 2.2 Hypertension Causes Newborn to 1 year o Renal artery thrombosis o Renal artery stenosis (RAS) o Renal vein thrombosis o Congenital abnormalities – dysplasia / hypoplasia / ARPKD o Aortic coarctation o Neuroblastoma o Raised Intracranial Pressure o Wilm’s tumour o Bronchopulmonary dysplasia o Patent ductus arteriosus o Intraventricular haemorrhage o Drugs - corticosteroids 1 to 5 years o RAS o Middle aortic syndrome o Glomerulonephritis o Renal vein thrombosis o Phaeochromocytoma o Neuroblastoma o Cystic kidney disease o Corticosteroids o Monogenic hypertension (Liddle’s syndrome) o Wilm’s tumour 5 to 10 years o Reflux nephropathy o Glomerulonephritis o Cystic renal disease o RAS o Middle aortic syndrome o Endocrine tumours o Wilm’s tumour o Other parenchymal renal disease – nephronopthisis o Essential hypertension o Obesity 10 to 20 years o Essential HT o Reflux nephropathy o Glomerulonephritis o RAS o Endocrine tumours o Monogenic HT o Pregnancy o Drugs: oral contraceptive, corticosteroids, alcohol, ecstasy, amphetamines o Obesity NB. Aetiologies may overlap at different ages. Renal failure should always be considered at any age. Raised intracranial pressure and pain should always be thought of and excluded. Presentation Simon Rhodes Page 2 March 2008 Paediatric Clinical Guideline Renal: 2.2 Hypertension The vast majority of children with Hypertension are asymptomatic. Infants vomiting / failure to thrive (rarely) irritability congestive cardiac failure / respiratory distress Older children headache / nausea / vomiting visual symptoms tiredness / irritability Bell’s palsy / hemiplegia epistaxis growth failure altered conscious level / fitting Hypertensive crisis is a medical emergency and can present at any age with: Encephalopathy Seizures Congestive cardiac failure NB For the unconscious or fitting child refer to guideline “Management of a child with decreased conscious level” (see page 7, table 13 for hypertension). See Appendix 2 Around two thirds of severe or symptomatic hypertension in childhood is likely to be renal in origin. Hypertension is linked to obesity with ~30% higher blood pressure with BMI centile >95%. Evaluation Full History to include specifically; o o o o o o Polyuria / dysuria / enuresis - renal disease Palpitations / flushing – phaeochromocytoma failure to thrive / lethargy / visual disturbances / headache / nausea or vomiting prescribed drugs: oral contraceptives, ADHD medications, steroids illicit drug use: ecstasy, amphetamines, cocaine pregnancy Family history o essential hypertension o familial hypertension. o sudden death o renal failure o MI or stroke Simon Rhodes Page 3 March 2008 Paediatric Clinical Guideline Renal: 2.2 Hypertension Examination o Height / weight / OFC / body mass index o radio-femoral delay or arm-leg BP discrepancy (i.e. leg < arm) – aortic coarctation or Takayasu’s disease o café-au-lait spots, axillary freckling – NF type1 o abdominal bruit - renovascular disease o short stature, anaemia, deafness, renal osteodystrophy – chronic renal failure o ambiguous genitalia - adrenogenital syndromes o urinalysis: proteinuria +/- haematuria o examine fundi and CVS for end-organ damage Investigation The 2 main purposes of investigation of hypertension are to define cause and assess presence and severity of end-organ damage. All children o Urinalysis for protein / blood / infection o Urine culture and microscopy (if indicated) o FBC anaemia consistent with chronic disease o Paediatric Renal Profile – i.e. U&E, Creatinine, Calcium, Phosphate, Albumin, PTH, Alkaline Phosphatase o Renal Ultrasound o Fasting Lipids and Glucose (to review co-morbidity i.e. teenagers, chronic kidney disease, diabetes mellitus, family history or signs of abnormal lipid metabolism o Thyroid function tests o Urinary catecholamine’s Consider: pregnancy test, urinary steroid profile, toxicology screen, renin and aldosterone. End-organ damage o Echocardiogram +/- ECG o Retinal examination -ophthalmology review should be considered in children with longstanding / severe hypertension Children with evidence of renal disease and hypertension should be referred to Paediatric Nephrology for further investigations and management Further tests to consider at this point include: renin / aldosterone and renovascular imaging NB. Try to obtain blood and urine samples before starting antihypertensive therapy BUT do not delay necessary treatment. Simon Rhodes Page 4 March 2008 Paediatric Clinical Guideline Renal: 2.2 Hypertension Management The goal of treatment is to reduce BP to below the 98th percentile o <91st if co-morbidity present e.g. Diabetes, LVH, chronic kidney disease o In some groups of children it may be beneficial to aim for blood pressure to be lower i.e. <50% because of their long-term cardiovascular disease risk For some children where hypertension is ‘borderline’ and there is no obvious abnormality or cause (following baseline investigations and examination) simple lifestyle measures are appropriate along with regular (at least 6 monthly) blood pressure monitoring. o Such measures include: regular exercise, management of obesity, reducing dietary salt intake, attention to use of alcohol/illicit drugs and prescribed drugs. The choice of drug should be discussed with the child’s Consultant, and varies depending on the cause of hypertension in the individual patient. Aim to keep the regime as simple as possible o E.g. use of long-acting once-daily preparations, when the blood pressure is stabilised o It may be best to start off with short-acting preparations (e.g. Nifedipine) until stability achieved and total daily dose calculated NB. Children with Renal Failure may have hypertension secondary to retention of sodium and water and generally need restriction of fluids and sodium intake together with diuretics as a first line Management of these children should be discussed with the relevant Paediatric Nephrology Consultant Management of hypertensive encephalopathy This is a specialised area and is to be covered in a separate guideline (Acute severe hypertension / Hypertensive encephalopathy). These children should be managed in an appropriate ICU / HDU setting, with care led by PICU Consultant. The important basic steps of management of hypertensive encephalopathy are: A,B,C,D approach Seizure control A controlled slow reduction in blood pressure to avoid CNS ischemia Simon Rhodes Page 5 March 2008 Paediatric Clinical Guideline Renal: 2.2 Hypertension Appendix One Measurement of Blood Pressure in children Standards All Children should have their BP measured as part of their clinical assessment. Palpation of the brachial pulse to identify systolic blood pressure followed by auscultation (using stethoscope and aneroid sphygmomanometer) is the ‘gold standard’ and should be used to verify / exclude abnormal blood pressure readings measured on oscillometry (Dinamap). Oscillometry can be unreliable in severe hypertension. Use of an appropriately sized cuff is very important - bladder length should cover 80100% of the circumference of the arm. A cuff that is too small will overestimate the blood pressure. Ideally the measurement should be taken after the child has been at rest for 3 to 5 minutes, using the right arm, which should be supported at heart level (false low readings in coarctation of the aorta when left arm used). At least two measurements should be taken and the average used. Systolic BP is determined by the onset of the ‘tapping’ Korotkoff sounds (K1), and diastolic by the disappearance of all sounds (K5). (If sounds are heard to 0 mmHg, diastolic pressure should be recorded as K4 – “muffled” sounds). Hypertension should be confirmed on repeated visits (except in the presence of severe or symptomatic hypertension) over a period of weeks. Severe / symptomatic hypertension requires urgent action (i.e. discussion with Consultant on-call). Doppler can be used to detect systolic blood pressure in young infants. Ambulatory blood pressure monitoring may be available via the Paediatric Renal Unit as some children may demonstrate “white-coat” hypertension. ABP is only suitable for children of 6 years and over. Simon Rhodes Page 6 March 2008 Paediatric Clinical Guideline Renal: 2.2 Hypertension Appendix Two Reference data / tables for hypertension 1) Reference (90th Centiles for age and sex) for children 0-4 years BOYS GIRLS Age Systolic Diastolic Systolic Diastolic 0 87 68 76 68 3 mth 106 63 104 64 6 mth 105 66 106 66 9 mth 105 68 106 67 1 yr 105 69 105 67 2 yrs 106 68 105 69 3 yrs 107 68 106 69 4 yrs 108 69 107 69 Simon Rhodes Page 7 March 2008 Paediatric Clinical Guideline Renal: 2.2 Hypertension 2) Systolic BP for children aged 4-17 years (GB data) Simon Rhodes Page 8 March 2008 Paediatric Clinical Guideline Renal: 2.2 Hypertension Simon Rhodes Page 9 March 2008 Paediatric Clinical Guideline Renal: 2.2 Hypertension 3) Diastolic BP for children aged 4-17 years (GB data) Simon Rhodes Page 10 March 2008 Paediatric Clinical Guideline Renal: 2.2 Hypertension Appendix Three Algorithm summarizing management of Hypertensive children Simon Rhodes Page 11 March 2008 Paediatric Clinical Guideline Renal: 2.2 Hypertension References 1. Blood pressure centiles for Great Britain. Children aged 4-17 years – oscillometric data; ADC 2007;92:298-303. 2. Paediatrics 1996;98:649-658 3. Paediatric Clinics of North America 1999;46:235 Simon Rhodes Page 12 March 2008 Paediatric Clinical Guideline Renal: 2.2 Hypertension 4. Forfar and Arneil Fifth edition p 972-973 5. Blood pressure centiles for Great Britain; Jackson LV, Thalange NKS, Cole TJ.ADC 2007;92:298-303. 6. NICE guidelines – No. 34, Hypertension (adult guideline). Simon Rhodes Page 13 March 2008