Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Cardiac contractility modulation wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Coronary artery disease wikipedia , lookup
Jatene procedure wikipedia , lookup
Myocardial infarction wikipedia , lookup
Cardiothoracic surgery wikipedia , lookup
Electrocardiography wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
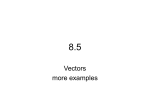
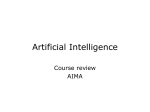
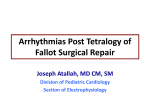
(Acta Anaesth. Belg., 2014, 65, 1-8) Junctional Ectopic Tachycardia after Congenital Heart Surgery E. Cools and C. Missant Abstract : Purpose : In this literature review, we try to give anesthesiologists a better understanding about Junctional Ectopic Tachycardia (JET), a narrow complex tachycardia that frequently occurs during and after surgery for congenital heart disease. Source : Information was found in the databases of Pubmed, Science Direct, Medline and the Cochrane Library, by using the mesh terms “Tachycardia, Ectopic Junctional”, combined with “Diagnosis”, “Etiology”, “Physiopathology”, “Complications” and “Therapy”. The publication date of the articles ranged from 1990 to 2012. Principal Findings : Risk factors for the development JET are surgery near the AV node, a duration of cardiopulmonary bypass longer than 90 minutes, young age, the use of inotropic drugs and hypomagnesaemia. The diagnosis of Junctional Ectopic Tachycardia can be made on a 12-lead ECG, demonstrating a narrowcomplex tachycardia with inverted P-waves and VA dissociation. Adenosine administration and an atrial electrocardiogram can help to confirm the diagnosis. If JET has a minimal impact on the hemodynamic status of the patient, risk factors should be avoided and the adrenergic tonus should be reduced. Hemodynamic unstable JET can be treated by amiodarone, hypothermia and pacing. Extracorporeal membrane oxygenation (ECMO) and radiofrequency or cryoablation are treatment options for life-threatening and resistant JET. Conclusion : JET is the most frequent arrhythmia during and after congenital cardiac surgery. The ECG is the only available method to diagnose JET, demonstrating inverted P-waves and VA-dissociation. Amiodarone seems to be the most effective treatment option, because it can restore sinus rhythm and reduces the JET rate. Keys words : Junctional Ectopic Tachycardia ; Con genital Cardiac Surgery ; Tachycardia. important cause of morbidity and mortality related to congenital heart surgery. The tachycardia and the loss of atrial-ventricular synchrony can lead to severe hemodynamic instability (2). JET arises near the AV node (junctional), where an ectopic focus starts to fire automatically with a frequency of 170 to 260 beats per minute (tachycardia). The impulses can be conducted to the atria and ventricle at the same time (ventriculo-atrial association) or more impulses can be conducted to the ventricle than to the atria (ventriculo-atrial dissociation) (3). Frequently, another supraventricular tachyarrhythmia precedes JET. With an incidence reported ranging from 2 to 11.2%, JET is the most frequent arrhythmia after congenital cardiac surgery (4) and mortality rates have been reported to vary from 3 to 13.5% (5, 6). In the majority of cases, JET occurred immediately after surgery or during the first post- operative day (5). In very rare occasions, JET can occur as late as 50 days after surgery (7). The diagnosis of JET can be difficult. Some medications which are used to treat tachyarrhythmia that have a strong resemblance with JET, can cause an aggravation of the arrhythmia and should be avoided (8). The exact cause of JET is not known, but several associations and predictors of JET have been studied and identified. Early attention to these factors makes it possible to avoid them when possible and to create preventive strategies. While there are many ways to successfully treat JET, there is no consensus about the best treatment options. Many anti- arrhythmic drugs have been used, but some of them have important side- ffects and should be avoided. JET is a self- imiting arrhythmia. In Introduction Junctional Ectopic Tachycardia (JET) or Hisbundle tachycardia is a narrow complex tachycardia that can present as a primary idiopathic arrhythmia during infancy (so called congenital JET), but most often occurs in the postoperative period after congenital cardiac surgery (1). JET is an Evelien Cools, MD ; Carlo Missant,MD, PhD. Department of Anesthesiology, University Hospitals Leuven and the Department of Cardiovascular Sciences, KU Leuven, Belgium Correspondence address : Prof Dr Carlo Missant, Department of Anesthesiology, University Hospitals Leuven, Herestraat 49, 3000 Leuven, Belgium. Tel : +32 16 34 42 70. Fax : +32 16 34 42 45. E-mail : [email protected] © Acta Anæsthesiologica Belgica, 2014, 65, n° 1 Cools et al.indd 1 31/03/14 09:25 2 e. cools and c. missant most instances it will resolve spontaneously, within 2 or 3 days (9). It is, however, difficult to predict when the resolution of the arrhythmia will occur. Pathophysiology The exact cause of JET is still not completely understood. Surgery near the AV node or the proximal conduction system (such as VSD closure or RV outflow tract repairs) seems to be an important factor in the pathogenesis and increases the risk of JET (8). During surgery, direct manipulation of the heart can result in myocardial injury and increase the electrical excitability (10). Indeed, autopsy reports have mentioned hemorrhagic tracts that invaded the tissue near the AV node (11). The surgeon can reduce the incidence of JET by trying to minimise the traction and manipulation of the heart (8). However, this can be difficult to achieve and furthermore, JET has also been reported in operations which don’t take place in the area of the AV node (7). Risk factors One can distinguish pre-, per- and postoperative risk factors for the development of JET. The age of the patient and surgery near the AV-node, are preoperative risk factors. The younger the patient (or the lower the weight of the patient), the greater the risk of developing JET with associated hemodynamic compromise. Manipulation and traction during surgery are relatively greater in a small heart (8, 12). Moreover, the myocardium of the young child has an increased non-contractile tissue mass (13) and a sarcoplasmatic reticulum with a reduced storage capacity for calcium (14). In addition, the first hours after surgery, systolic and diastolic function of the heart is impaired due to postoperative myocardial oedema. Hence, the cardiac output (which is determined by heart rate and stroke volume) is more dependent on the heart rate in these circumstances. During tachycardia, the ventricle has not enough time to fill in, which will have a negative impact on the cardiac output. There is some evidence that JET is more frequently observed in children who have experienced an episode of heart failure before the actual surgery (5). Cardio- pulmonary bypass (CPB) and aortic cross clamping, commonly used during congenital heart surgery, result in decreased myocardial perfusion, which possibly can cause myocardial damage although cardioprotective strategies are being applied in clinical practice. Per-operatively, the aortic cross clamp time is the best predictor of JET (4, 5). It has been reported that a total duration of CPB longer than 90 minutes, is associated with an elevated risk to the development of JET and other heart rhythm disorders (3, 8). Surgeries with a higher grade of complexity, e.g. redo surgery, need more manipulation of the heart, have a longer CPB-time and therefore lead to a higher incidence of JET (3, 15). To have an idea about the extent of myocardial injury due to trauma and ischemia, creatinine kinase (CK-MB), troponin-I and -T can be measured after CPB. Elevated levels of these markers have been reported to be associated with an increased risk of JET (6, 16). Positive inotropic drugs, hyperthermia, anae mia and electrolyte imbalances are all associated with JET in the per- and postoperative setting. During weaning from, and sometimes after, CPB, inotropes such as dobutamine and epinephrine can be necessary to increase the contractility of the heart. An important side-effect of these medications however is their positive chronotropic and arrhythmogenic effect. This effect is even more pronounced in the immature myocardium of the young child and during heart failure, thereby diminishing the cardiac output and increasing myocardial oxygen consumption (5). In addition to positive inotropic drugs, hyper thermia and anaemia can also increase the heart rate and have been shown to be associated with an increased incidence of JET (1, 7). While acute electrolyte imbalances definitely increase the incidence of arrhythmias, hypo magnesaemia seems to be the most essential in the pathogenesis of JET (15). Hypomagnesaemia causes an intracellular potassium deficiency and an augmented intracellular calcium concentration, leading to an increase in myocardial excitability (17). In addition, magnesium attenuates the degree of myocardial necrosis and plays a cardioprotective role in ischemia-reperfusion injury by decreasing the catecholamine release from the adrenal medulla and adrenergic nerve endings (14). Many factors can cause hypomagnesaemia during surgery, e.g. hemodilution, blood loss and transfusions, large amounts of intravenous fluids, increased urinary loss, catecholamine-induced lipolysis and ischemia (14, 17). Consequently, magnesium and the other electrolytes should be measured and corrected repetitively during surgery. © Acta Anæsthesiologica Belgica, 2014, 65, n° 1 Cools et al.indd 2 31/03/14 09:25 junctional ectopic tachycardia3 Fig. 1. — Diagnosis of Junctional Ectopic Tachycardia based on the electrocardiogram. Since JET arises near the AV-node, it’s a small-complex tachycardia with a ventricular rate ranging from 170 to 260 bpm. Because of the retrograde activation of the atrium, the P-wave is negative (18). Reproduced with permission from RnCeus.com Fig. 2. — The difficult differential diagnosis with other supraventricular tachycardia. On this ECG, you can see a smallcomplex tachycardia with a heart rate of 260 beats per minute. P-waves aren’t visible. This narrow-complex tachycardia can be Junctional Ectopic Tachycardia or another supraventricular tachycardia. Afterwards, it proved to be Junctional Ectopic Tachycardia. If the focus of the junctional rhythm lies low nodal or in the proximal His bundle, the P-wave will coincide with the T-wave on the ECG (19). Reproduced with permission from Bash S., M.D. Diagnosis The 12-lead electrocardiogram (ECG) is the only and therefore most important tool to diagnose JET. Since JET arises near the AV node, it is a small-complex tachycardia (Fig. 1) (18). Because of the retrograde atrial activation, the P-wave will typically be inverted. The timing of the P-wave depends on the specific location of the ectopic focus. If the ectopic focus arises at the top of the AV-node, the P-wave takes place prior to the QRS-complex. In case of an ectopic focus that lies in the centre of the AV node, the P-wave will disappear into the QRS-complex. If the focus lies low nodal or in the proximal His-bundle, the P-wave will coincide with the ST-segment or the T-wave (Fig. 2) (3, 19). Depending on the electrical conduction pattern, 2 types of JET occur in clinical practice. There can be ventricular-atrial association (VA-association), where every ectopic beat will be conducted to the ventricle and atrium : ventricular and atrial rate are thus equal (1:1). This is more frequently seen in the younger patients. Most of the time, however, VA-dissociation occurs and more impulses will be conducted to the ventricle than the atria and the atrial frequency will therefore be lower than that of the ventricle (Fig. 3) (1, 10). Frequently, other supraventricular tachycardias or a transient AV block precede JET. In contrast to other supraventricular tachycardias where the heart rate suddenly increases (e.g. from 120 to 200 beats per minute), the heart rate gradually increases over time in JET. For this reason, JET is said to have a “warm-up pattern” (1). Hence, the ECG-pattern in JET isn’t uniform at all. Moreover, a bundle branch block can also coincide with JET, leading to a broadcomplex tachycardia (Fig. 4A) (1, 20). Therefore, the differential diagnosis with other arrhythmias can be difficult. Fig. 3. — The effect of adenosine on Junctional Ectopic Tachycardia. During the first 4 ventricular complexes, there is VA-association : every QRS-complex is followed by an inverted P-wave. After the 4th and 5th ventricular complex, the P-wave disappears. This can be normal in Junctional Ectopic Tachycardia, or can be caused by adenosine. VA-association occurs more frequently in younger patients (1, 10). A strategy that is frequently used to discriminate JET from other forms of tachycardia is the use of adenosine. Adenosine blocks the conduction through the AV node and suppresses the automaticity of the atrial and Purkinje tissue (21). By blocking the AV node, an atrial tachycardia can be unmasked and a paroxysmal supraventricular tachycardia, in which the AV node is a component of the re-entry circuit, can be terminated. Adenosine can suppress JET for a very short time, but does not terminate it (22). In JET with VA-association, adenosine blocks retrograde atrial conduction and VA-dissociation appears (Fig. 3) (1, 10, 20). The recommended dose of adenosine in the diagnosis of JET is 0.1-0.4 mg/kg intravenously, with a maximum dose of 6 mg. Because of the short half-life of 20 seconds, adenosine will be preferably administered via a central venous catheter (21). Side effects of adenosine are sinus bradycardia, flushing, dyspnea and nausea. Adenosine should be used with caution in patients with asthma, sinus node dysfunction and orthotopic cardiac transplantation (23). © Acta Anæsthesiologica Belgica, 2014, 65, n° 1 Cools et al.indd 3 31/03/14 09:25 4 e. cools and c. missant An important difference between JET and paroxysmal supraventricular tachycardia is the response to electrical cardio-version. While PSVT is sensitive to cardio-version, JET doesn’t react (22). When the diagnosis of JET remains unclear, the temporary epicardial pacing wires, which are placed during surgery, can be used to create an atrial electrocardiogram (ACG). An ACG can unmask the P-waves that disappear in the QRS-complex or T-wave (Fig. 4) (1, 20) and, in addition, demonstrate VA-dissociation (24). An atrial ECG can be taken by placing one atrial pacing wire underneath the gel pad of a precordial chest lead, such as precordial lead V1. In this way, the ACG and ECG can be recorded simultaneously and the P-waves will be augmented on the ECG (20, 25). Treatment JET is a self-limiting arrhythmia. However, no one can predict when exactly the arrhythmia will resolve. Hence, the loss of VA-synchrony and tachycardia can cause a severe hemodynamic instability needing urgent medical treatment. The pivotal step in the management of JET consists of correction and avoidance of all possible risk factors associated with JET and which are mentioned above. First, increased adrenergic tone should be avoided whenever possible as it will accelerate the JET rate. Therefore, routine critical care (anxiolysis and continued postoperative sedation) is the cornerstone measure in the prevention of JET (1). Similarly, positive inotropic drugs can have arrhythmic side effects. Although it can be difficult to avoid these drugs during surgery for congenital heart disease, they should be used at a dosage as low as possible. Milrinone, a positive inotropic drug with phosphodiesterase inhibitor activity can also be arrhythmogenic, but has the advantage to have relatively less effect on the heart rate in comparison to dobutamine and epinephrine because it acts independently of the β-adrenergic receptor. Therefore, milrinone should be the positive inotropic drug of choice, despite the side effect of severe hypotension (7, 26). Vagolytic drugs, e.g. pancuronium, mepiridine and barbiturates, should also be used with caution, as they can increase the JET rate. Other causes of tachycardia, e.g. hypovolemia, fever and anaemia, should be avoided or immediately corrected (26). During every congenital cardiac surgery, the haemodynamic status of the patient should be adequately monitored using invasive arterial blood pressure, assessment of serum lactate levels, urine output and (whenever possible) transoesophageal echocardiography and mixed venous oxygen (24). While only hypomagnesaemia saturation proved to be a risk factor of JET, all acute electrolyte and pH disturbances should immediately be treated, because they can lead to other forms of arrhythmias (4). Amiodarone, a type III anti-arrhythmic agent with both alpha- and beta receptor blocking properties, prolongs the action potential and refrac tory period of every ventricular contraction (24). It has the highest efficacy rate for the treatment of JET and is therefore the first-line treatment option to restore sinus rhythm and slow the heart rate (1, 8, 27). Amiodarone should be administered whenever JET leads to hemodynamic instability. Possible dosing regimens include the intravenous administration of one or two loading boluses of 5 mg/kg with a maximum bolus dose of 15 mg/ kg/day. If necessary, these loading boluses can be followed by a continuous infusion of 10-20 µg/ kg/min, diluted in dextrose 5% (1, 28, 29). The use of amiodarone in hemodynamic stable JET is controversial, due to the associated side effects such as hypotension, bradycardia, AV block and torsade de pointes (Table 1) (1, 27, 30). The hypotension can be treated by volume boluses (1) or calcium gluconate 10% (24). Amiodarone seems to be effective in the treatment of JET in 80-90% of the cases (24, 29, 31). A lower body temperature and a large difference between the arterial and venous oxygen saturation, which is related to a low cardiac output, are predictors of failure of amiodarone therapy. In these particular patients, amiodarone could be combined with hypothermia to have a more adequate first line approach (see below) (8). Once the sinus rhythm has been restored, the amiodarone infusion can then gradually be weaned. Because of the prolonged half-life of amiodarone after prolonged infusion or during hemodynamic instability, one should monitor for late sinus bradycardia (24). Other anti-arrhythmic drugs have only been tested in small series. The beta-blockers esmolol and sotalol have both successfully been used in the treatment of JET, mainly by reducing the JET rate (1, 5, 24), but have the disadvantage to have a negative inotropic effect (1). Propanolol only has a minimal effect when administered during an episode of JET, but it has been reported that the preoperative use of propanolol seems to reduce the incidence of JET (1, 28). Recently, the alpha-2 adrenergic © Acta Anæsthesiologica Belgica, 2014, 65, n° 1 Cools et al.indd 4 31/03/14 09:25 junctional ectopic tachycardia5 Table 1 Treatment options for Junctional Ectopic Tachycardia. The most relevant side- effects are mentioned. JET : Junctional Ectopic Tachycardia, SR : Sinus Rhythm, TdP : Torsade de Pointes, IV : intravenous, ECMO : extracorporeal membrane oxygenation (1, 8, 19, 22, 24, 27, 32) Treatment Effect Side- effects Amiodarone Restoration of SR, reduces JET- rate Hypotension, bradycardia, AV block, TdP Beta- blockers Reduces JET- rate Negative inotrope Dexmedetomidine Restoration of SR, reduces JET- rate Hypotension, bradycardia, nausea, dry mouth Hypothermia Decreases automaticity of ectopic focus, reduces JET rate and metabolic oxygen requirements Metabolic acidosis, peripheral vasoconstriction, cardiac arrhythmias, coagulation abnormalities and impaired immunity Pacing Establish AV synchrony ECMO Extracorporeal heart support Thrombosis, bleeding, infections and exposure to additional blood products Ablation Destroys the ectopic focus Complete AV block agonist dexmedetomidine has drawn quite some attention. Dexmedetomidine seems to be effective to restore sinus rhythm during JET by its depressive effect on the AV node. Advantages compared with amiodarone are that dexmedetomidine’s side effects are less pronounced. Dexmedetomidine has a faster onset of action, prevents shivering during hypothermia and has sedative, analgesic and anxio lytic properties (33). In a very recent paper, Le Riger and co-workers have successfully used dex medetomidine to control JET in an infant after tetralogy of Fallot repair (32). Unfortunately, the number of studies about the use of dexmedetomidine in JET are limited, but its promising effects clearly makes it an interesting drug for the treatment of JET in the future (33). Importantly, certain drugs that are used in the treatment of supraventricular tachycardia, can aggravate JET. Supraventricular tachycardia can be treated with vagal manoeuvers, adenosine, beta-blockers, amiodarone and calcium channel blockers. In JET, calcium channel blockers should be avoided because of the negative inotropic effect that can induce atrial fibrillation (1, 17, 34). While digoxine was used years ago to treat JET, it has no place anymore in the treatment of JET, because of the increase in JET rate and the myocardial cell excitability (6, 24). Another difference between JET and PSVT is the response to electrical cardioversion. While PSVT can be converted to normal sinus rhythm by electrical cardioversion, JET is resistant (22). If amiodarone therapy fails, another treatment option might be the induction of hypothermia to 32-34°C as it will decrease the automaticity of ectopic pacemaker cells (1, 6, 22). A decreased core temperature cannot restore sinus rhythm, but it can significantly slow the ventricular rate, thereby ameliorating diastolic filling and hemodynamic stability. In addition, hypothermia reduces the metabolic oxygen requirements and the myocardial work (24). Hypothermia can be induced by cooling blankets, ice packs or by the administration of cooled infusion solutions (19). Only a few studies examined the best way of cooling during JET but it has been reported that cooling with intravenous cold saline has the advantage to have less side-effects, to generate a more homogenous cooling and to have a better temperature control (35). It is important that, during hypothermia, the patient must be sedated, paralyzed and mechanically ventilated to prevent shivering (1, 8). Hypothermia has a range of sideeffects such as metabolic acidosis, peripheral vasoconstriction, cardiac arrhythmias and impaired (19, 24). Therefore, coagulation and immunity antibiotic prophylaxis should be administered (1). The duration of cooling varies among the studies : most of the time, cooling during 1-3 days resolves JET, but there are case reports where cooling was necessary for one week (1). Procainamide, a type I anti- arrhythmic, has a higher efficiency in the treatment of JET when combined with hypothermia (28). A bolus of 515 mg/kg, if necessary followed by a continuous infusion of 20-120 µg/kg/min seems to be effective in controlling JET. Adverse effects of procainamide are bradycardia, hypotension and proarrhythmic effects (24). Procainamide combined with hypo thermia could resolve JET in 50-80% of the cases (31, 35). If the haemodynamics do not improve after amiodarone-therapy or hypothermia, cardiac pacing should be initiated in an effort to establish atrioventricular synchrony (24). Some authors start pacing © Acta Anæsthesiologica Belgica, 2014, 65, n° 1 Cools et al.indd 5 31/03/14 09:25 6 e. cools and c. missant Fig. 5 — Flowchart of the management of JET. JET : Junctional Ectopic Tachycardia, CPB : Cardiopulmonary Bypass, CK- MB : Creatinine- Kinase, Bpm : beats per minute, VA : Ventriculo- Atrial, ACG : Atrial electrocardiogram, ECMO : Extracorporeal Membrane Oxygenation. before inducing hypothermia (1). The pacing rate should be 5 to 10 beats per minute higher than the actual JET rate. Pacing can be performed by using the temporary pacing wires placed during surgery, by external pads or by trans-oesophageal pacing. Atrial (AAI), synchronous (DDI) and paired ventricular pacing (in which two stimuli are delivered to the ventricle in close succession to slow the heart rate (36) can all be tried to achieve atrioventricularsynchrony (1, 24). Pacing should however be stopped frequently to evaluate the underlying heart rate, cardiac output and rhythm. Flecainide, a type Ic anti-arrhythmic drug, decreases the automaticity of the ectopic focus and improves the outcome of JET when combined with atrial pacing. The used dose of flecainide in JET is a bolus of 2 mg/kg followed by a continuous infusion of 0.40 mg/kg per hour. Flecainide has a fast onset of action, but it’s myocardial depressive effect should be closely monitored (1, 28, 31). If the JET remains resistant to all of the above mentioned treatment options or the haemodynamic imbalance creates a serious life-threatening situa tion, the circulation of the child can be supported by extracorporeal membrane oxygenation (ECMO). The deleterious side-effects of ECMO should be outweighed by the life-saving nature of this treatment strategy (30). Besides ECMO, radiofrequency or cryoablation might be the ultimate treatment for JET (24). An important complication of ablation is the creation of a complete AV block, which needs pacemaker implantation. Complete AV block has less frequently been reported after radiofrequency ablation. ECMO is a more attractive technique for the treatment of severe hemodynamic unstable JET (30). An overview of all possible treatment options for JET with the associated side effects is given in Table 1. Figure 5 provides a flowchart of the management of JET in the perioperative phase. Conclusion JET is the most frequent arrhythmia during and after congenital cardiac surgery. Therefore, it is important for everybody involved in the operative care of congenital heart surgery peri patients to recognise and treat JET early. The ECG is the only available method to diagnose JET. Adenosine and an atrial electrocardiogram can help to confirm the diagnosis. Risk factors are surgery near the AV node, duration of CPB longer than 90 minutes, a young age, heart failure before surgery, electrolyte disturbances (especially hypomagnesaemia), hyperthermia and anaemia. If JET occurs, the hemodynamic impact should be examined thoroughly. Many treatment options have © Acta Anæsthesiologica Belgica, 2014, 65, n° 1 Cools et al.indd 6 31/03/14 09:25 junctional ectopic tachycardia7 been studied. Of these, amiodarone seems to be the most effective because it can restore sinus rhythm and reduces the JET rate. Hypothermia and pacing are second-line treatment options. Extracorporeal membrane oxygenation or ablation are necessary if the hemodynamic status of the patient is really compromised. Acknowledgements This review was funded with instutional grants only. References 1.Haas N., Plumptom K., Justo R., Jalali H., Pohlner P., Post operative junctional ectopic tachycardia (JET), Z. Kardiol., 93, 371-380, 2004. 2.Roger B., Mee B., Surgical substrates of postoperative junctional ectopic tachycardia in congenital heart defects, J. Thorac. Cardiovasc. Surg., 123, 615-616, 2002. 3.Malmivuo J, Plonsey R., Cardiac Rhythm Diagnosis. In : Malmivuo J, Plonsey R. Bioelectomagnetism. Oxford Press, New York, 323-326, 1995. 4.Kamel Y., Sewielam M., Arrhythmias as Early Postoperative Complications of Cardiac Surgery in Children at Cairo University, J. Med. Sci., 9, 126-132, 2009. 5.Andreasen J., Johnsen S,. Ravn H., Junctional ectopic tachycardia after surgery for congenital heart disease in children, Intensive Care Med., 34, 895-902, 2008. 6.Batra A., Chun D., Johnson T., et al., A Prospective Analysis of the Incidence and Risk Factors Associated with Junctional Ectopic Tachycardia Following Surgery for Con genital Heart Disease, Pediatr. Cardiol., 27 : 51-55, 2006. 7.Hoffman T., Bush D., Wernovsky G., Postoperative Junctional Ectopic Tachycardia in Children : Incidence, Risk Factors, and Treatment, Ann. Thorac. Surg., 74, 1607-1611, 2002. 8.Kovacikova L., Hakacova N., Dobos D., Skrak P., Zahorec M., Amiodarone as a First-Line Therapy for Post operative Junctional Ectopic Tachycardia, Ann. Thorac. Surg., 88, 616-623, 2009. 9.Walsh E., Facc J., Saul P., et al., Evalutaion of a Staged Treatment Procotol for Rapid Automatic Junctional Tachycardia After Operation for Congenital Heart Disease, JACC, 29, 1046-1053, 1997. 10.Perry J., Junctional Ectopic Tachycardia : Epidemiology, Pathophysiology, Primary Prevention, Immediate Evalua tion and Management, Long-Term Management, and Experimental and Theoretical Developments, Cardiac Electrop hysiology Review, 76-78, 1997. 11.Till J. A., Ho S. Y., Rowland E. Histopathological findings in three children with His bundle tachycardia occurring subsequent to cardiac surgery. Eur. Heart J., 13(5), 709712, 1992. 12.Wildes N., Mallett S., Peachey T., Di Salvo C., Walesby R. Correction of Ionized Plasma Magnesium During Cardio pulmonary Bypass Reduces the Risk of Postoperative Cardiac Arrhythmia. Anesth. Analg., 95 : 828-834, 2002. 13.Brett C., Pediatrics. In : Stoelting R, Miller R. Basics of Anesthesia, 5th Edition. Churchill and Livingstone, Philadelphia, 504-517, 2007. 14. Manrique A., Arroyo M., Lin Y., et al., Magnesium supple mentation during cardiopulmonary bypass to prevent junc tional ectopic tachycardia after pediatric cardiac surgery : A randomized controlled study. J. Thorac. Cardiovasc. Surg., 139, 162-169, 2010. 15.Mildh L., Hiipala A., Rautiainen P., Pettilä V., Sairanan H., Hzpponrn J. M., Junctional ectopic tachycardia after surgery for congenital heart disease : incidence, risk factors and outcome. Eur. J. Cardiothorac. Surg., 7676, 1-6, 2010. 16.Pfammatter J. P., Wagner B., Berdat P., et al., Procedural factors associated with early postoperative arrhythmias after repair of congenital heart defects. J. Thorac. Cardiovasc.Surg., 123, 258-262, 2002. 17. Delaney J., Moltedo J., Dziura J., Kopf G., Snyder C., Early postoperative arrhythmias after pediatric cardiac surgery. J. Thorac. Cardiovasc. Surg., 131, 1296-301, 2006. 18.Bauer P., RnCeus, Interactive website, http ://www.rnceus. com/ekg/junctach.gif 19.Bash S., Shah J., Albers W., Geiss D. Hypothermia for the Treatment of Postsurgical Greatly Accelerated Junctional Ectopic tachycardia, JACC, 5, 1095-1099, 1987. 20.Robida A., Early Arrhythmias in Children after Cardiac Surgery, Heart Views, 1(6), 223-228, 1999. 21.Bakshi F., Barzilay Z., Paret G., Hashomer T. Adenosine in the diagnosis and treatment of narrow complex tachycardia in the pediatric intensive care unit, Heart & Lung, 27, 4750, 1998 22.Bouzas-Mosquera A., Rueda-Nenez F., Mosquera-Perez I. Postoperative junctional ectopic tachycardia, Archives of Cardiovascular Disease, 102, 335-336, 2009. 23. Paul T., Pfammatter J. P., Adenosine : An Effective and Safe Antiarrhythmic Drug in Pediatrics. Pediatr. Cardiol., 18, 118-126, 1997. 24. Erickson S. J., Guidelines for the management of junctional ectopic tachycardia following cardiac surgery in children, Current Paedicatrics, 16, 275-278, 2006. 25.Batra A., Balaji S. Post operative temporary epicardial pacing : When, how and why ? Ann. Pediatr. Card., 1(2), 120-125, 2008. 26.Sheikh F., Uppal M., Farina M., Wilson J., Diagnosis and Management of Junctional Ectopic Tachycardia. J. Cardio thorac. Vasc. Anesth., 11 : 203-205, 1997. 27.Dodge-Khatami A., Miller I., Anderson R., Gil-Jaurena J., Goldman A., De Leval M., Impact of junctional ectopic tachycardia on postoperative morbidity following repair of congenital heart defects. Eur. J. of Car.-Thor. Surg., 255259, 2002. 28.Mahmoud A., El Tantawy A., Kouatli A., Baslaim G., Propranolol : a new indication for an old drug in preventing postoperative junctional ectopic tachycardia after surgical repair of tetralogy of Fallot, Interact. Cardiovasc. Thorac. Surg., 184-187, 2008. 29.Laird W, Snyder C, Kertesz N, Friedman R, Miller D, Fenrich A. Use of Intravenous Amiodarone for Postoperative Junctional Ectopic Tachycardia in Children. PediatrCardiol 2003 ; 24 : 133-137. 30.Tsoutsinos A., Papagiannis J., Chatzis A., Sarris G., Sur gi cal Cryoablation for Life-Threatening Postoperative Junctional Tachycardia, Ann. Thorax. Surg., 84, 286-288, 2007. 31.Bronzetti G., Formigari R., Giardini A. et al., Intravenous Flecainide for the Treatment of Junctional Ectopic Tachycardia After Surgery for Congenital Heart Disease, Ann. Thorac. Surg., 76, 148-151, 2003. 32.Leriger M., Naguib A., Gallantowicz M., Tobias J. D., Dexmedetomidine controls junctional ectopictachycardia during Tetralogy of Fallotrepair in an infant, Ann. Card. Anaesth., 15(3), 224-228, 2012. © Acta Anæsthesiologica Belgica, 2014, 65, n° 1 Cools et al.indd 7 31/03/14 09:25 8 e. cools and c. missant 33.Chrysostomou C., Beerman L., Shiderly D., Berry D., O Morell V., Munoz R.. Dexmedetomidine : A novel drug for the treatment of atrial and junctional tachyarrhythmias during the perioperative period for congenital cardiac surgery : a preliminary study, Anesth. Analg., 107 : 15141522, 2008. 34.Blomstrom-Lundqvist C., Scheinman M., Aliot E., et al., ACC/AHA/ESC guidelines for the management of patients with supraventricular arrhythmias, Eur. Heart. J., 24, 1857-1897, 2003. 35.Kelly B., Gajarski R., Ohye R., Charpie J., Intravenous Induction of Therapeutic Hypothermia in the Management of Junctional Ectopic Tachycardia : A Pilot Study, Pediatr. Cardiol., 31 : 11-17, 2010. 36.Kohli V., Young M., Perryman R., Wolff G., Paired Ven tricular Pacing : An Alternative Therapy for Postoperative Junctional Ectopic Tachycardia in Congenital Heart Disease, Pace, 22, 706-710, 1999. © Acta Anæsthesiologica Belgica, 2014, 65, n° 1 Cools et al.indd 8 31/03/14 09:25