Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Biochemistry wikipedia , lookup
Developmental biology wikipedia , lookup
Human embryogenesis wikipedia , lookup
Human genetic resistance to malaria wikipedia , lookup
Cell-penetrating peptide wikipedia , lookup
List of types of proteins wikipedia , lookup
Cell theory wikipedia , lookup
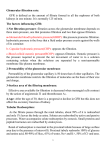
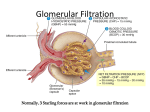
MOLECULAR PHYSIOLOGY Excretory system Punam Verma*, Vineet Mehrotra and Sunita Mittal *Associate Professor Department of Physiology SGRRIM&HS Patel Nagar Dehradun 3-Jul-2006 (23-May-2007) CONTENTS Introduction Functions of kidney Kidney structure Structure of nephron Types of nephron Renal blood flow Mechanism of urine formation Glomerular filtration Tubular transport process Hormonal regulation of tubular reabsorption and tubular secretion Renal handling of some common solutes and water Keywords Excretory system; Urine formation; Filtration; Reabsorption; Secretion Introduction Excretion literally, the word excretion means elimination of any matter from the body of an organism. Different organs and systems like digestive system, respiratory system, excretory system and skin are involved in the process of excretion. However, here the term excretion refers to elimination of principal products of metabolism except carbon dioxide i.e. removal of ammonia, urea, uric acid, creatinine, various pigments and inorganic salts. Thus in strict sense kidneys are excretory organs. Together with a pair of ureter and a urinary bladder kidneys constitute excretory system (Fig 1). Fig. 1: Urinary system Functions of kidney The kidneys do the major function of the urinary system. The other parts of the system are mainly passageways and storage areas. Functions of kidney are: 1. Homeostatic function: It maintains constancy of the interval environment of body by (a) Regulating blood ionic composition Kidneys regulate the blood levels of several ions like Na+, K+, Ca++, Cl- etc. (b) Regulating blood pH - It maintain blood pH by excreting variables amount of H+ into urine and conserving H CO3- in the blood. (c) Regulating blood volume - It adjust blood volume by conserving or eliminating water in urine. (d) Regulating blood pressure - It regulate blood pressure by secreting renin . (e) Maintain blood osmolarity - By separately regulating loss of water and loss of solutes in the urine. Kidneys maintain relatively constant blood osmolarity 300 milli osmoles/liters. 2. Endocrine function: It secretes: (a) Erythropoietin hormonewhich stimulates production of RBC from stem cell. (b) 25-Dihydroxycholecalciferol (active form of vitamin D),which helps to regulate calcium homeostasis. (c) Renin from Juxta-glomerular cells in response to low BP. It converts angiotensinogen into angiotensin I (Ag I) which in presence of angiotensin converting enzyme is converted into angiotensin II (AgII) which is a powerful vasoconstrictor and helps to maintain BP. 3. Regulating blood glucose level: Kidneys can also synthesize glucose from amino acid, glutamine etc. 2 4. Excreting waste and foreign substances: By forming urine kidneys help to excrete wastes. Kidney structure The kidneys are paired organs, each weighting 150 gm in adults. They are located retroperitonealy in the upper dorsal region of the abdominal cavity on either side of vertebral column. It is bean shaped organ approximately 10 cm long, 5 cm wide and 2.5 cm thick. Right kidney occupies slightly lower position due to pressure of liver on that side. The lateral border of each kidney is convex and its medial side is deeply concave. In the middle of the medial side there is depression leading to a hollow chamber called renal sinus through which blood vessels, nerves, lymphatic renal pelvis and ureter passes. Vertical section of kidney (Fig. 2) shows: 1. Outer cortex reddish in colour looks granular due to arrangements of nephrons. It forms shell-surrounding medulla. 2. Inner medulla is pale in colour. It contains 10 – 15 conical mass of tissues called pyramids whose bases are directed towards convex surface of the kidney. They terminate medially in the renal papillae. Papillae projects into calyces, such 10 – 15 minor calyces join to form two major calyces, which come out through pelvis of kidney to the widened end of the ureter. Fig. 2: Vertical section of kidney Structure of nephron The basic functional unit of the kidney is the nephron. There are about 1.2 million nephrons in each kidney, which drain into pelvis. Total length of nephrons is 45-65mm. Each nephron is formed by two parts (Fig. 3): 1. Renal corpuscle or malpighian corpuscle 2. Renal tubule 3 Fig. 3: Structure and histology of nephron Renal Corpuscle – It is a rounded structure comprising glomerulus, surrounded by glomerular capsule also called as Bowman’s capsule (Fig. 4). Fig. 4: Renal Corpuscle 4 Glomerulus – It is a tuft of anastmozing capillaries. Blood enters the glomerulus through afferent arterioles and leaves it through efferent arterioles. Capillaries are made up of single layer of endothelial cells. Bowman’s capsule – It is a cup shaped structure having two layers: i) Visceral layer, closely applied to the loops of capillaries from all sides and ii) Parietal layer form the outer layer having glomerulus and is continuous with epithelial lining of proximal tubule. A space between visceral layer and parietal layer is called as Bowman’s space (BS). Structure of glomerular membrane It is the membrane through which blood filters from capillaries into Bowman’s space and it is also called as filtration barrier. It is made up of three layers (Fig. 5): 1. Endothelial layer of capillaries 2. Basement membrane 3. Visceral layer of Bowman’s capsule/ layer of podocytes Fig. 5: Glomerular capillary membrane Endothelial layer of capillaries: The endothelium is fenestrated i.e. contains holes of about 70-90 nm and is freely permeable to water, small solutes such as sodium, urea and glucose and even very small proteins but not all since this layer express negatively charged glycoproteins (sialoproteins) on their surface, which retard the filtration of large anionic proteins. Basement membrane: This is a porous matrix (pore size <8nm) of extra cellular proteins including collagen, laminin, fibronectin and other negatively charged proteins. It is an important filtration barrier to plasma protein. Unlike other basement membrane it is very thick. Visceral layer: It has special type of cells called podocytes, which have finger like projections. These projections interdigitate to cover the basement membrane and are separated by gaps called filtration slits. Each filtration slit is bridged by a thin diaphragam, which contains pores with dimensions of 25 nm. Therefore, filtration slit retard the filtration 5 of some proteins and macromolecules that pass through endothelium and basement membrane. Renal tubule The tubular portion of nephrons is the continuation of Bowman’s capsule. It is made up of four parts: 1. Proximal convoluted tubule (15 mm) 2. Loop of Henle (14 - 26 mm) 3. Distal convoluted tubule (5 mm) 4. Collecting duct (20 mm) Proximal convoluted tubule (PCT) The initial coiled, portion is called as pars convoluta while distal portion is straight and is called as pars recta. The epithelial lihing is continuous with the parietal layer of Bowman’s capsule. The epithelial cells are metabolically active as they have large number of mitochondria in it. The apical surface has brush border due to presence of microvill in order to increase the absorptive surface area. These cells are united with each other, with tight junction, at their apex. Function: These cells take part in active reabsorption and secretion of some organic substances and ions. Glucose, amino acid, lactic acid, uric acid, ascorbic acid, phosphate, sulphate, potassium, calcium, sodium ions and water are reabsorbed while penicillin, histamine, creatinine and H+ are actively secreted. Loop of Henle (LH) It consists of i) Descending thin segment (DTS), ii) Ascending thin segment (ATS) and iii) Ascending thick limb (TAL). The fluid in the descending limb runs towards renal pelvis and in ascending limb run towards cortex. The DTS and ATS are made up of single layer of squamous epithelial cells which do not have brush border and have very few or no mitochondrias so these are metobolically inactive and only passive transport process can take place in these segments. The TAL has cuboidal epithelial cell layer with prominent brush border and has large number of mitochondrias. Therefore, TAL has functions similar to that of PCT. Function From descending limb water is reabsorped From ascending limb Na, K and Cl ions are reabsorbed Distal convoluted tubule (DCT) TAL is continuous with DCT. This tubule comes very close to its own glomerulus and establishes a close proximity to the afferent and efferent arteriole of the glomerulus. At this point the cells of the tubule get modified and closely crowned together and called as Macula densa cells. Function: DCT is an important site for active secretion of ions, acids etc. Na ions are actively reabsorbed and water is reabsorbed in presence of ADH and H ions are secreted actively 6 Collecting duct (CD) The collecting duct, strictly speaking is not a part of nephron because it is derived from the ureteric buds. Depending upon the region where it is present, is divisible into three parts: i) Cortical collecting duct (CCD) ii) Outer medullary collecting duct (OMCD). iii) Inner medullary collecting duct (IMCD) The last part of DCT and continuing collecting duct has two different types of cells: i) Principal cell (P-cell):- They are abundant in number, have moderately invaginated basolateral membrane and contains very few mitochondrias . They have receptor for ADH & aldosterone hormone so increase the permeability for water & Na+. ii) Intercalated cell (I- cell):- Few in number and have large number of mitochondrias. They play role in maintaining blood pH by secreting H+ in the urine. Several IMCDS join together before finally opening at the tip of Renal papilla. Types of nephron There are two types of nephrons cortical nephron and Juxta medullary nephron. The differences between these are listed in Table 1 and Fig. 6. Table 1: Difference between cortical and juxtamedullary nephron Cortical nephron Juxta medullary nephron Number of nephron Size and location of glomeruli 80 – 85% Small size glomerulus in renal cortex Loop of henle Short loop of henle may reach upto medulla In ascending limb ATS is absent Vascular supply is in the form of peritubular capillaries Mainly involved in the formation of urine 15%. Large size, located at the junction of cortex and medulla. Long loop of henle goes deep into the medulla Both ATS and TAL are present in ascending limb It is in the form of vasa recta. Vascular supply Function Involved in the concentration of urine Juxta glomerular apparatus (JGA) It is a combination of specialized tubular and vascular cells located at the vascular pole where the afferent and efferent arterioles enter and leave the glomerulus (Fig. 7). It is composed of three types of cells: a) Juxta glomerular cells – These are specialized myoepithelial cells located in the media of afferent arterioles. They have well developed golgi apparatus, endoplasmic reticulum, mitochondria and ribosomes. They synthesize store and release an enzyme called renin. These cells act as baroreceptor as they respond to change in blood 7 pressure and also monitor vascular volume. They are richly innervated with sympathetic fibers. Fig. 6: Cortical and juxtamedullary nephron Fig. 7: Juxtaglomerular apparatus 8 b) Macula densa cells –These cells refer to the specialized renal tubular epithelial cells near the vascular pole. These cells have prominent nuclei and golgi complex. They act as chemo receptors and are stimulated by decreased NaCl load in DCT, thereby cause increase renin release. c) Mesangial cells or Lacis cells - These are supporting cells of JGA and found between capillary loops. They are contractile in nature and play role in glomerular filtration by increasing or decreasing the surface area of filtration membrane (Table 2). Table-2 Agents causing contraction and relaxation of mesangial cell Contraction Angitensin II ADH Endothelins Histamine Norepinephrin PGF2 Platelet activating factor GFR Relaxation GFR Atrial natriuretric peptide (ANP) c-AMP Doapmine PGE2 Renal blood flow Renal blood vessels To perform its function, kidneys are abundantly supplied with blood vessels. Although they constitute less than 0.5% of the total body mass but they receive 20-25% of the resting cardiac output via the renal artery. Renal artery enter the kidney at the pelvis and then branch into several segmental arteries, which enter the parenchyma and pass through the renal columns between the renal pyramids as the interlobar arteries which at the base of renal pyramid arches between the cortex and medulla as arcuate artery. Division of arcuate arteries give rise to series of interlobular arteries, which enter the renal cortex and branches called as afferent arteriole. It is short, thick walled and each divded into multiple capillary branches to form, glomerulus. The glomerular capillaries, exhibit higher pressure of about 45 mm Hg than that in other capillary bed, join to form efferent arteriole whose diameter is smaller to afferent arteriole but possess a thinner wall. They have relatively high resistance. These breakup to from peritubular capillary plexus in cortical nephrons and surrounds all the convoluted tubule in the cortex. The juxtamedullary nephrons form peritubular capillary plexus and also sub divides into bands of straight vessels called Vasa Recta (VR) which run parallel to the convoluted tubules into the medulla. Both these join to form stellate vein which drains into inter lobular vein, actuate vein, inter lobar vein and finally into renal vein which leave the kidney at renal pelvis (Fig. 8). Characteristics of RBF 1) Amount and rate of blood flow i. The rate of blood flow in this region of the body is quite high in comparison to blood flow in other region. Renal blood flow (RBF) is 1.2 – 1.3 lit / min (400 ml /100gm/ min) or 1700–1800 L / day. 9 Renal plasma flow (RPF) is 650 ml / min or 900 L / day Coronary blood blow - 60 – 80 ml / 100 gm / min Brain blood flow - 55 ml / 100 gm / min Skin blood flow - 3 – 4 ml / 100 gm / min ii. Higher blood flow in kidney is related to its excretory function rather than its metabolic requirement. iii. Afferent arteriole, efferent arterioles and intralobular artery are the major resistance vessels in kidney and they determine renal vascular resistance. iv. Renal oxygen consumption is very high (6 ml / 100 gm / min) as compared to that in heart (8 ml / 100 gm / min). Fig. 8: Blood supply of kidney: A - Blood vessels in cortex; B - V/S showing major arteries and vein 2) Intra renal distribution of RBF - Of the total RBF, 90 % blood perfuses cortex and only 10 % perfuses renal medulla Blood flow in cortex 5 ml / gm/ min in outer medulla 2.5 ml / gm/ min in inner medulla 0.6 ml / gm/ min 10 Low blood flow to medulla plays an important role in concentration of urine and is because of high vascular resistance in vasa recta which may be due to: i) long length of vasa recta (40 mm); ii) increase viscosity of blood near the hair pin band of loop of Henle; iii) small number of these vessels; iv) low hydrostatic pressure head because the diameter of efferent arterioles arising from JM nephron is small. Regulation of Renal Blood Flow Same regulatory mechanisms affect both RBF and GFR therefore this section will be discussed with regulation of GFR. Mechanism of urine formation Three process are involved in the formation of urine (Fig. 9): 1) Glomerular filtration - It is the function of renal corpuscle of nephrons 2) Tubular Reabsorption 3) Tubular Secretion Reabsorption and secretion are the function of tubular part of nephron. Both these process are together are called tubular transport process. Fig. 9: Mechanism of urine formation Glomerular filtration Glomerular filtration is defined as the ultra filtration of plasma from the glomerular capillaries into the Bowman’s capsule. It is the first step in the urine formation. To understand this process this section is divided into following sub headings: i) Characteristics of filtration membrane. ii) Composition of glomerular filtrate. iii) Dynamics of glomerular filtration. iv) Glomerular filtration rate (GFR) v) Filtrations fraction. vi) Factors affecting glomerular filtration. 11 vii) viii) Regulation of glomerular filtration. Measurement of glomerular filtration. i) Characteristics of filtration membrane: As discussed previously, filtration membrane consists of three layers: capillary endothelium, glomerular basement membrane and visceral layer. The characteristic features of the membrane are: 1) It is highly permeable to water and to water soluble substances due to its porous nature 2) This membrane also exhibits high degree of selective permeability which depends upona) Pore size – Pore size of endothelial layer is 70 –90nm , of basement membrane is 8nm and of visceral layer is 25 nm. Therefore, 1. Molecules less than 4 nm in size can freely pass. 2. Molecules with diameter more than 8nm are not filtered at all. 3. Filtration of molecules having diameter between 4nm –8nm is inversely proportional to their diameter. b) Electrical charge – This membrane is negatively charged due to presence of glycoproteins rich in silica acid. Therefore the negatively charged molecules are less permeable than neutral and positive charged molecules. This is the reason that albumin, although has 7nm molecular diameter, is not filtered. ii) Composition of glomerular filtrate: It is similar to plasma composition except that it is devoid of cells and proteins. The composition may alter in some diseases due to alteration in permeability of membrane. For example in glomerular disease the negative charge of membrane is lost and protein filters across membrane and appears in the urine (Proteinuria / albuminuria ) in significant amount. iii) Glomerular filtration rate (GFR): The total quantity of filtrate formed in all the nephrons of both kidney in the given unit time is called as glomerular filtration rate (GFR). The normal value of GFR in an average man is 125ml/mn or 180 L/day. It is directly proportional to the surface area but in women it is 10% lower than in man. After age of 30 year, GER declines with age. iv) Dynamics of glomerular filtration: The forces that determine the filtration of plasma are similar to the forces, which determine the absorption of fluid in interstitial space through capillaries. GFR is the product of filtration coefficient and net filtration pressure. GFR = Kf x Net filtration pressure. Where Kf is filtration coefficient, which depends upon the glomerular capillary membrane permeability and the surface area of filtration membrane and is equal to 12.5. Net filtration pressure is the difference of the forces that favours the filtration and the forces that opposes the filtration. Basically four forces (Starling forces) act at the filtration membrane (Fig. 10) 1. Hydrostatic pressure in glomerulus (PG) = 45 mm Hg. 2. Hydrostatic pressure in Bowman’s space (PB) = 10 mm Hg. 3. Oncotic pressure in glomerular capillaries (πG) = 25 mmHg 4. Oncotic pressure in Bowman’s space (πB), which is taken as 0 as it does not contain proteins. PG and πB favors filtration while Pb and πG opposes the filtration Net filtration pressure = (PG + πB) – (PB + πG) 12 So, GFR = = = = Kf x [(PG + πB) – (PB + πG)] 12.5 x (45 + 0 – 25 – 10) 12.5 x 10 125 ml / min Fig. 10: Dynamics of glomerular filtration 13 v) Filtration fraction (FF): It is the fraction of plasma that flows through kidneys get filters at glomerulus into Bowman’s space. GFR 125 FF = = = 0.16 – 0.22 RPF 620 – 700 = 16 % – 22 % Therfore, filtration fraction is 16 % – 22 % of RPF i.e., only 16 % – 22 % of plasma, that flows through kidneys, filters at glomerulus. vi) Factors affecting Glomerular Filtration Rate 1. GFR decreases with advancing age due to decrease in renal plasma flow, cardiac output and renal tissue mass. 2. GFR changes with RBF in linearity. 3. Hydrostatic pressure in glomerulus – If PG increases GFR also increases. PG increases in afferent arteriolar dilatation and efferent arteriolar constriction PG decreases with decreased arterial pressure, afferent arteriole constriction and efferent arteriole dilatation. 4. Oncotic pressure in Glomerulus (πG) - Increase in πG results in decrease in GFR Increase in πG is seen in hyperproteinmemia e.g. dehydration. Decrease in πG is seen in hypoproteinemia e.g. severe anaemia and nephrotic syndrome 5. Hydrostatic pressure in Bowman’s space (PB) - With increase in PB, GFR decreases e.g.obstruction to urine flow i.e. in ureteric calculus. 6. Membrane permeability – permeability of glomerular membrane increases in its infection as in glomerular nephritis and decreases when it becomes thick as in diabetes mellitus. 7. Surface area of filtration membrane – Greater the surface area more will be the GFR while small surface area reduces GFR. vii) Regulation of GFR: Since the same regulatory mechanism affects both GER and RBF so regulation of RBF is also discussed with regulation of GER Before discussing various regulatory mechanisms, it is essential to understand the relationship between changes in afferent arteriole and efferent arteriole with RBF and GFR (Fig.11). 1. Constriction of afferent arteriole decreases both RBF and GFR without charges in filtration fraction. 2. Dilatation of the afferent arteriole increases both RBF and GFR without charges in filtration fraction. 3. Constriction of efferent arteriole decreases the RBF but increases GFR so also filtration fraction. 4. Dilatation of efferent arteriole increases RBF and Decreases GFR and filtration fraction. The mechanisms that regulates RBF and GFR are: • Autoregulation, • Hormonal regulation, and • Nervous regulation. 14 Fig. 11: Relation of afferent and efferent arteriole diameter with RBF and GFR 1. Autoregulation of GFR and RBF The renal blood flow (RBF) and thus the glomerular filtration rate (GFR) remain constant over a wide range of renal arterial pressures, 80-200mm Hg (Fig 12). This occurs due to an intrarenal mechanism known as autoregulation. Fig. 12: Autoregulation of RBF and GFR 15 Mechanism of autoregulation: Autoregulation has been observed to persist after renal denervation, in the isolated perfused kidney, in the transplanted kidney, after adrenal demedulation, and even in the absence of erythrocytes thus ruling out the role of all these factors. Two mechanisms are considered responsible for autoregulation of RBF and GFR: i) Myogenic mechanism: It is related to an intrinsic property of vascular smooth muscle, the tendency to contract when it is stretched. Thus, when renal arterial pressure is raised, the afferent arterioles are stretched and with the result they constrict. Increase in vascular resistance offsets the effect of increased arterial pressure and thereby maintains a constant RBF and GFR. ii) Tubuloglomerular feedback (TGF) mechanism: Tubulo-glomerular feedback (TGF) mechanism is based on the NaCl concentration of tubular fluid. It involves a feedback loop which operates as (Fig 13) Fig 13: Tubuloglomerular feedback mechanism 16 • • • • • Changes in the GFR cause change in NaCl concentration of fluid in the loop of Henle. Changes in the NaCl concentration are sensed by the macula densa cells and converted into a signal. The signal from the macula densa cells changes the vascular resistance in afferent arterioles. Increase in GFR causes increase concentration of NaCl load in DCT, which is sensed by macula densa cells and they produce afferent arteriolar constriction. This results in decrease of GFR and decrease load of NaCl in DCT. Conversely signals obtained due to decreased NaCl causes vasodilatation of afferent arterioles and so on. The effector mechanism responsible for vasoconstriction and vasodilatation is not exactly known. Perhaps, adenosine triphosphate (ATP), which selectively constricts the afferent arterioles and metabolites of arachidonic acid may contribute to TGF mechanism. Physiological significance: Autoregulation of GFR and RBF is an effective mechanism for uncoupling renal function from fluctuation in arterial pressure and maintain fluid and electrolytic balance. Special features of autoregulatory mechanisms • Autoregulation mechanisms do not work when the mean arterial blood pressure falls below 80 mm Hg or increases more than 200 mm Hg • Autoregulation is not a perfect mechanism. • Several hormones and other factors can change RBF and GFR in spite of autoregulatory mechanisms. 2. Hormonal regulation: Both GFR and RBF are also influenced by hormones as described in Table 3. Table 3: Hormones influencing RBF and GFR Decrease in GFR &RBF by Vasoconstrictors Increase in GFR & RBF by Vasodilators Nor epinephrine Prostaglandins (no effect on GFR) Nitric oxide Bradykinin Dopamine Histamine Angiotensin II Endothelin 3. Nervous regulation: Like most blood vessels of the body, kidneys are supplied by sympathetic fibers from T12 - L2 segments. At rest, sympathetic stimulation is moderately low, the afferent and efferent arterioles are dialated and renal autoregulation, of GFR prevails. With moderate sympathetic stimulation, both afferent and efferent arteriole constrict to the same degree, decreasing GFR and RBF only slightly. With greater sympathetic stimulation, as occurs during exercise and hemorrhage, 17 vasoconstrictuion of afferent arteriole predominate, as a result, blood flow into glomerular capilllaries is greatly decreased and GFR drops. vii. Measurement of GFR - GFR can be measured by renal clearance of inulin, urea and creatinine. Tubular transport process About 180 L of glomerular filtrate is formed per day and only 1.5 L is excreted in the form of urine i.e. 99% of filtered water and many useful substances are reabsorbed. The different segments of tubule like PCT, Loop of Henle, DCT and Collecting duct determines the composition and volume of urine by the process of selective reabsorption and selective secretion of water and solutes (Table 4). For understanding, tubular transport can be studied in the following subheadings: A. General consideration: 1. Transport pathways and mechanisms across cell membranes. 2. Selective reabsorption 3. Pattern of renal handling 4. Quantification of renal tubular transport. B. Transport across different segments of nephrons. C. Renal handling of some common solutes and water. Table 4: Substances filtered, reabsorbed, secreted nad excreted in the urine Substances Filtered Reabsorbed Secreted Excreted Percentage 2000 Na+ (mEq) + 720 K (mEq) 18000 Cl+- (mEq) 4900 HCO3 (mEq) ++ 540 Ca (mEq) 800 Glucose (mmol) 870 Urea(mmol) 12 Creatinine (mmol) 50 Uric acid (mmol) Total solute (mosmol) 54000 180 Water (L) 25850 620 17850 4900 530 800 435 1 49 53400 178.5 1 100 - 150 100 150 10 0 435 12 5 700 1.5 99.1 86.1 99.2 100 98.2 100 50 98 98.9 99.2 A. General Consideration 1. Transport pathways and mechanisms across Tubular cell membrane In renal tubule, substances can be transported by two pathways (Fig. 14): (i) Paracellular pathway: Transport between the cells through tight junctions.. (ii) Transcellular pathway: Transport across the cell. It is a two-step process. The substances can be transported by a) Active transport process and b) Passive transport process– Diffusion, facilitated diffusion and solvent drag. For reabsorption by 18 transcellular pathway, a substance first has to pass from tubular lumen into the tubular epithelial cell and then from cell into the lateral intercellular space. The opposite happens if the substance has to be secreted by transcellular pathway. The water moves across the cell passively while solutes moves both actively and passively. For these mechanisms various pumps, carriers and channels are present (Table 5). Fig. 14: Reabsorption pathway Table 5: Various transport mechanisms in a nephron Pumps Carrier Symporter 3Na+2K+ ATPase 3 H+- ATPase H+-K+ ATPase Ca++-ATPase Na+-Glucose Na+-Amino-acid 2Na+- HPO4Na+-3HCO3Na+-2Cl-K+ K+-Cl- Channel Antiporter Na+ - H+ Na+ - NH4+ Na+-Ca++ Cl- - HCO3- Na+ K+ ClCa++ 2. Selective reabsorption The tubular cell reabsorbs the substances present in glomerular filtrate according to the need of the body. So the tubular reabsorption is selective reabsorption, the various substances are classified into three categories: i) High threshold substance – The substances like glucose, amino acids and vitamins are completely reabsorbed and do not appear in the urine. These 19 ii) iii) substances can reappear in urine only when their concentration in plasma is very high or in renal disease when they are not re-absorbed. Low threshold substance – The substances such as urea, uric acid and phosphate are reabsorbed to little extent. These appear in urine even under normal conditions. Non-threshold substance – The metabolic end products like creatinine are not reabsorbed and are excreted in urine irrespective of their concentration in plasma. 3. Pattern of renal handling A substance may be handled in different ways while passing through nephrons (Fig. 15): i) By glomerular filtration only, e.g. Inulin ii) By glomerular filtration plus partial reabsorption, e.g. urea. iii) By glomerular filtration plus complete reabsorption, e. g. Glucose iv) By glomerular filtration plus partial secretion, e.g. PAH v) By glomerular filtration plus tubular reabsorption and secretion, e.g. K+. vi) By only secretion, e.g. organic compound bound to proteins. 4. Quantification of renal tubular transport i) Filtered load : Amount of substance entering the tubule through glomerular filtration per unit time. It is denoted as Fo. Fo = GFR x Px ii) Excretion rate :It is the amount of substance that appear in the urine per unit time. It is denoted as Eo. Eo = V x Ux V - Urine flow rate Ux - Concentration of substance in the urine iii) Reabsorpton rate : It is the rate at which a particular substance is reabsorbed. It is labeled as R. R = Fo - Eo iv) Secretion rate : It is the rate at which substance is secreted from peritubular capillaries into the tubule. It is denoted as S. S = Eo - Fo v) Tubular transport maximum: Like transport system elsewhere in the body, renal active transport system have a maximal rate or Transport maximum (Tm) at which they can transport particular solute. The rate of transport of any substance depends upon the rate at which this specific transport system operates. The transport system, in turn, depends upon the carrier substance or enzyme. So the maximum rate at which a substance is reabsorbed or secreted is called as tubular transport maximum or Tm for that solute. Thus the amount of a particular substance transported is proportionate to the concentration of that solute but after certain limit, when that carrier becomes saturated then no amount of solute is transported. This is called as (Tm) for that solute. Reabsorbed substances that have (Tm) are glucose, amino acids, uric acid, albumin etc. Secreted substances that have (Tm) are PAH, penicillin, certain diuretics, vitamins etc. 20 A C B D Fig. 15: Tubular transport in PCT – A. Sodium glucose transport, B. Bicarbonate reabsorption, C. Sodium hydrogen exchange, D. Passive reabsorption of Cl-, K+,Ca++, Mg++, Urea and water B. Transport across different segments of nephrons Reabsorption and secretion in the proximal convoluted tubule The largest amount of solute and water reabsorption occurs in PCT (Fig. 16). 21 Fig. 16: Tubular transport in LH Substances reabsorbed: Approximately 67% of the filtered water, Na+, Cl-, K+ and other solutes like Ca++, Mg++ and urea are reabsorbed from here. Glucose, amino acids and vitamins are 100% reabsorbed but reabsorption of HCO3– is 80-90%. Substances secreted: H+, PAH, drugs, creatinine etc are secreted in this segment. Various pumps and carriers: On apical surface – Na- glucose/ amino acid transporter (Symport) Na+- H+ exchange (Antiport) On basolateral surface: Na- K ATPase Mechanism i) Normally, filtered glucose, amino acids, lactic acid, water-soluble vitamins, and other nutrients are not lost in the urine. Rather, they are completely reabsorbed in the first half of the proximal convoluted tubule (PCT) by Na+ symporters located in the apical membrane. ii) Another secondary active transport process, the Na+ /H+ antiporters, carry filtered Na+ down its concentration gradient into a PCT cell in the exchange of H+ which is secreted into tubular fluid. PCT cells produce the H+ in the following way: Carbon dioxide (CO2) diffuses from peritubular blood or tubular fluid or is produced by metabolic reactions within the cells. As also occurs in red blood cells the enzyme carbonic anhydrase (CA) catalyzes the reaction of CO2 with water (H2O) to form carbonic acid (H2CO3), which then dissociates into H+ and HCO3- . The HCO3 diffuses in the blood while H+ is secreted into the fluid within the lumen of the proximal convoluted tubule and it reacts with filtered HCO3- to form H2CO3, which dissociates into CO2 and H2O. Carbon dioxide then diffuses into the tubule cells and joins with H2O to from H2O3. Thus, every H+ secreted into the tubular fluid of the proximal convoluted tubule causes reabsorption of a filtered HCO-3. iii) Besides achieving reabsorption of sodium ions, the Na+ symporters promote osmosis of water and passive reabsorption of other solutes. As water leaves the tubular fluid, the 22 concentration of the remaining filtered solutes increase. In the second half of the PCT, electrochemical gradients for Cl- , K+ , Ca2+ , Mg2+ , and urea promote their passive diffusion into peritubular capillaries via both paracellular and transcellular routes. Among these ions, Cl- is present in the highest concentration. Diffusion of negatively charged Cl- into interstitial fluid via the paracellular route makes interstitial fluid electrically more negative than the tubular fluid. This negativity promotes passive paracellular reabsorption of cations, such as K+, Ca2+, and Mg2+. iv) Each reabsorbed solute increases the osmolarity, first inside the tubule cell, then in interstitial fluid, and finally in the blood. Water thus moves rapidly from the tubular fluid, via both the paracellular and transcellular routes, into the peritubular capillaries and restores osmotic balance. In other words, reabsorption of the solutes creates osmosis. Cells lining that promote the reabsorption of water via osmosis. Cells lining the proximal convoluted tubule and the descending limb of the loop of Henle are especially permeable to water because they have many molecules of aquaporin–1. This integral protein in the plasma membrane is a water channel that greatly increases the rate of water movement across the apical and basolateral membranes. Transport process in the loop of Henle Because the proximal convoluted tubules reabsorb about 67% of the filtered water (about 80mL/min), fluid enters the next part of the nephrons, the loop of Henle, at a rate of 40 – 45 mL/min. The chemical composition of the tubular fluid now is quite different from that of glomerular filtrate because glucose, amino acids, and other nutrients are no longer present. However, the osmolarity of the tubular fluid is still close to the osmolarity of blood (~300mosmol/L) as reabsorption of water by osmosis keeps pace with reabsorption of solutes all along the proximal convoluted tubule. The LH reabsorbs about 20-30% of the filtered Na+, K+, Ca2+; 10 – 20% of the filtered HCO3; 35% of the filtered Cl-; and 15% of the filtered water (Fig. 17). Fig. 17: Tubular transport in late DCT and CD 23 Characterstics Pump: Na +2Cl – K+ symport is present on the apical membrane and Na +- K + ATPase on the basolateral surface. DTS: the membrane of it is highly permeable to water but moderately to solutes. Water is reabsorbed passively along with diffusion of Na+ from interstitial space into the tubular lumen. Therefore this limb is also called as concentrating segment. ATS: Passive reabsorption of Na+ and Cl- occurs in this region. TAL: It is impermeable to water but permeable to solutes. Half of the Na+ is reabsorbed actively through transcellular route and half of the Na+ is reabsorbed passively by paracellular pathway. Since there is no reabsorption of water and only solutes are reabsorbed therefore this limb is also called as diluting segment. Mechanism i) The apical membrane of cells in the thick ascending limb of the LH has Na+ - K+ - 2Clsymporters that simultaneously reclaim one Na+, one K+, and two Cl- from the fluid in the tubular lumen. Na+ that is actively transported into interstitial fluid at the base and sides of the cell diffuses into the vasa recta. Cl- moves through leakage channels in the basolateral membrane. Because many K+ leakage channels are present in the apical membrane, most K+ brought in by the symporters moves down its concentration gradient back into the tubular fluid. Thus, the main effect of the Na+ - K+ -2Cl- symporters is reabsorption of Na+ and Cl-. ii) The movement of positively charged K+ into the tubular fluid through the apical membrane channels leaves the interstitial fluid and blood with a negative charge relative to fluid in the ascending limb of the LH. This relative negativity promotes reabsorption of cations – Na+, K+, Ca2+ and Mg2+ - via the paracellular route. Since ions but not water molecules are reabsorbed from the TAL, the osmolarity of the tubular fluid progressively decreases as fluid flows towards the end of the ascending limb (~100 mosmol/L). Transport process in the distal convoluted tubule Filtered NaCl (7%) and water (8-17%) are reabsorbed while K+ and H+ are secreted in this segment. Characterstics Early DCT – Reabsorbs Na+, Cl-, and Ca++ but is impermeable to water like ALH. Pump: Na+ - Cl- symporter in apical membrane and Na+- K+ ATPase in the basolateral membrane. Fluid enters the distal convoluted tubules (DCT) at a rate of about 25mL/min because 80% of the filtered water has now been reabsorbed. As fluid flows along the DCT, reabsorption of Na+ and Cl- continues by means of Na+ -Cl- Symporters in the apical membranes. Sodium – potassium pumps and Cl- leakage channels in the basolateral membranes then permit reabsorption of Na+ and Cl- into the peritubular capillaries. The DCT also is the major site where parathyroid hormone (PTH) stimulates reabsorption of Ca+. 24 Transport process in the late DCT and collecting duct By the time fluids reach the end of the distal convoluted tubule, 90- 95% of the filtered solutes and water have returned to the blood stream. As described earlier late DCT and collecting duct have 2 types of cell: Principal cell - It causes reabsorption of (i) Na+ actively across basolateral surface with help of Na +K+ ATPase and passively across apical membrane, ii) Cl- passively through paracellular route, iii) water only in presence of ADH. iii) It causes secretion of K+ via Na +K + ATPase across basolateral membrane and which diffuses passively across apical membrane. Intercalated cell - It reabsorbs K+ by H+ - K+ ATPase in the apical membrane and secretes H+ by H+ ATPase. Note: Aldosterone hormone increases Na+ reabsorption and K+ excretion from principal cell while increases H+ secretion by intercalated cell by stimulating H+ ATPase. In contrast to earlier segments of the nephrons, Na+ passes through the apical membrane of principal cells via Na+ leakage channels rather than by means of symporters or antiporters. The concentration of Na+ in the cytosol remains low, as usual, because the sodiumpotassium pumps actively transport Na+ across the basolateral membranes. Then Na+ passively diffuses into the peritubular capillaries from the interstitial spaces around the tubule cells (Fig. 18). Normally, transcellular and paracellular reabsorption in the proximal convoluted tubule and loop of Henle return most of the filtered K+ blood stream. To adjust for varying dietary intake of potassium and to maintain a stable level of K+ into body fluids, principal cells, secrete a variable amount of K+ because the basolateral sodium-potassium pumps continually bring K+ into principal cells, the intracellular concentration of K+ remains high. K+ leakage channels are present in both the apical and basolateral membranes. Thus, some K+ diffuses down its concentration is very low. This secretion mechanism is the main source of K+ excreted in the urine. Hormonal regulation of tubular reabsorption and tubular secretion Four hormones affect the extent of Na+, Cl-, and water reabsorption as well as K+ secretion by the renal tubules. The most important hormonal regulators of electrolyte reabsorption and secretion are angiotensin II, ADH and alosterone. Atrial natriuretic peptide (ANP) plays a minor role in inhibiting both electrolyte and water reabsorption. Renin- Angiotensin-Aldosterone System When blood volume and blood pressure falls, the walls of the afferent arterioles are stretched less, and the juxtaglomerular cells secrete the enzyme renin into the blood. Sympathetic stimulation also directly stimulates release of renin from juxtaglomerular cells. Renin converts angiotensinogen into Ag I. Angiotensin converting enzyme (ACE) converts angiotensin Ag I to Ag II. Angiotensin II affects renal physiology in the following ways: 25 Fig. 18: Water reabsorption under the effect of AD i) It causes vasoconstriction of the afferent arterioles leading to decrease GFR. ii) It enhances reabsorption of Na+, Cl-, and water in the proximal convoluted tubule by stimulating the activity of Na+ /H+ antiporters. iii) It stimulates release of aldosterone hormone from adrenal cortex that in turn, stimulates the principal cells in the collecting ducts to reabsorb more Na+ and Cl- and secrete more K+. All these three mechanisms ultimately result in increase in blood volume. Antidiuretic hormone Antidiuretic hormone (ADH or Vasopressin) is released by the posterior pituitary. It regulates facultative water reabsorption by increasing the water permeability of principal cells in the last 26 part of the distal convoluted tubule and throughout the collecting duct. In the absence of ADH, the apical membranes of principal cells have a very low permeability to water. Within principal cells are tiny vesicles containing many copies of a water channel protein known as aquaporin –2. ADH stimulates insertion of the aquaporin-2 containing vesicles into the apical membranes via exocytosis. As a result, the water permeability of the principal cell’s apical membrane increases, and water molecules move more rapidly from the tubular fluid into the cells. Because the basolateral membranes are always relatively permeable to water, water molecules then move rapidly into the blood. The kidneys can produce as little as 400-500 mL of very concentrated urine each day when ADH concentration is maximal, for instance during severe dehydration. When ADH level declines, the aquaporin-2 channels are removed from the apical membrane via endocytosis. The kidneys produce a large volume of dilute urine when ADH level is low. A negative feedback system involving ADH regulates facultative water reabsorption (Fig. 18). When the osmolarity or osmotic pressure of plasma and interstitial fluid increase – that is, when water concentration decreases by as little as 1%, osmoreceptors in the hypothalamus detect the change. Their nerve impulses stimulate secretion of more ADH into the blood, and the principal cells become more permeable to water. As facultative water reabsorption increases, plasma osmolarity decreases to normal. A second powerful stimulus for ADH secretion is a decrease in blood volume, as occurs in hemorrhage or severe dehydration. In the pathological absence of ADH activity, a condition known as diabetes insipidus, person may excrete up to 20 liters of very dilute urine daily. Atrial natriuretic peptide A large increase in blood volume promotes release of atrial natriuretic peptide (ANP) from the heart. Although the importance of ANP in normal regulation of tubular function is unclear, it can inhibit reabsorption of Na+ and water in the proximal convoluted tubule and collecting duct. ANP also suppresses the secretion of aldosterone and ADH. These effects increase the excretion of Na+ in urine (natriuresis) and increase urine output (diuresis), which decreases blood volume and blood pressure. Transport of various substances across different segments of nephrons is summarized in table Renal handling of some common solutes and water 1. Renal handling of sodium and water Reabsorption of sodium Percentage reabsorption of the filtered sodium in different segments of the renal tubule is 67% from PCT, 20% from LH (mainly from TAL), 7% from DCT and 5% from CD. A mechanism of reabsorption is described in detail above in the subsection on transport across different segments of renal tubule. Sodium recycling The sodium, which is actively pumped out from the thick ascending limb (TAL) into the outer medullary interstitium, mostly enters the outer medullary descending thin segments (DTS). This results in recycling of Na+ in the long loops of the juxtamedullary nephrons. The recycling causes accumulation of Na+ in the interstitium of the renal medulla. 27 Reabsorption of water Water is absorbed passively by osmosis in response to a transtubular osmotic gradient. Rapid diffusion of water across the cell membrane occurs through water channels made up to proteins called Aquaporins. Different types of aquaporins are aquaporin-1, 2, 5 and 9. Mostly these are present in kidneys. Other sites are leucocytes, liver, lung and lacrimal gland. Renal handling of water by different segments of renal tubule is as follows: From PCT: Passive reabsorption (67 %). From Loop of Henle: Descending thin segment (DTS): Passive reabsorption (15 %) Ascending thin segment (ATS): Impermeable Thick ascending limb (TAL): Impermeable From Distal tubule and collecting duct: (8 to 17 %) Early DCT: Impermeable CCD: Reabsorption is ADH dependent OMCD: Reabsorption is ADH dependent IMCD: Reabsorption is ADH dependent Obligatory and facultative reabsorption of water Out of the total amount of water reabsorbed from the nephron, 80% of the reabsorption is compulsory i.e. about 80 % of the filtered water is always reabsorbed, irrespective of the body water balance. This reabsorption occurs by osmosis in response to a transtubular osmotic gradient and is called obligatory (must occur) reabsorption. About 67% of obligatory reabsorption occurs in the proximal tubules, and about 15-18% of obligatory reabsorption occurs in the descending thin segment of loop of Henle. The remaining 15-18% of the filtered water may or may not be absorbed depending upon the body water balance. It is called facultative (optional) reabsorption. Facultative reabsorption of water occurs from the late DCT and collecting tubule and is under the control of ADH. Regulation of NaCl and water absorption i) Hormonal regulation. Various hormones including angiotenisn II, aldosterone, ADH, ANP, urodilatin epinephrine and nor epinephrine (released from sympathetic nerves) and dopamine, regulates NaCl reabsorption (already discussed) ii) ADH is the only major hormone that directly regulates the amount of water excreted by kidney. iii) Role of starting forces. Although Na+ reabsorption is an active process, it is affected by the passive starling forces operating between the intercellular spaces and the peritubular capillaries in the proximal tubule. Glomerulotubular balance (GTB) – As GFR increases, the tubular reabsorption of solutes and water increases in PCT due to glomerulotubular balance (GTB). This mechanism in the proximal tubule maintains reabsorption at a constant fraction (2/3 or 67 % of the filtered Na+ and H2O). It is because of oncotic pressure in the peritubular capillaries. When GFR increases, more amount of plasma proteins accumulate in the glomerulus. Consequently, the oncotic pressure increases in the blood by the time it reaches to the efferent arteriole and peritubular capillaries. The elevated pressure in the capillaries increases reabsorption of sodium and water from PCT. 28 iv) Effects of ECF volume on proximal tubular reabsorption. a. ECF volume contraction increases reabsorption. b. ECF volume expansion decreases reabsorption. 2. Renal handling of glucose Glucose is freely filtered into glomerular filtrate. Filtration load (Fo) increase is direcly proportional to the plasma glucose concentration (PG). All filtered glucose is completely reabsorbed from PCT. The transport mechanism occurs in two steps (Fig. 15A): i) From lumen into cell via secondary active transport processes– Glucose binds with carrier protein, Sodium – Glucose transporter (SGLUT), located at the apical membrane. Transport of Na+ down its electrochemical gradient with the help of this carrier protein, into the cell liberates energy that is utilized to transport glucose into the cell against concentration gradient. ii) From cell into the intercellular space via facilitated diffusion - The carrier for this transport is called GLUT-2 and GLUT-1 Characteristic features of glucose reabsorption i) Glucose is reabsorbed by transport maximum process i.e. depend upon the number of Na+ glucose transporter. ii) The glucose reabsorbtion and excretion processes are function of the plasma glucose titration curve (Fig. 19): a) Increase in the PG result in progressive linear increase in the filtered load. b) At low PG glucose reabsorption is 100% i.e. no amount of glucose appears in urine. In this region, line of reabsorption is same as that of filtration. c) When PG increase above 180-200 mg the glucose reabsorption is incomplete and glucose appears in urine (Glycosuria). This PG at which glucose appears in urine is called as Renal Threshold for glucose, which is 200 mg % of arterial plasma and 180 mg% of venous plasma. d) Transport maximum Tm refers to the plasma concentration at which carrier proteins are fully saturated. As shown in figure, Tm for glucose is 375 mg/min i.e. after this PG level reabsorption rate become constant and is independent of PG. Thus, beyond TmG all the additional glucose is excreted in the urine. And now the urinary excretion rate increases in linearity with PG. Splay: It represents the excretion of glucose in urine before the TMG is fully achieved. It is between PG 180mg % and 350 mg% i.e. the predicted renal threshold for glucose is 300mg. However actual curve obtained is rounded rather than sharply angulated predicted curve. Normally their filtered load is 100mg/min. PG is 80mg %. So if glucose is filtered at therate of 375mg/min then PG will be 80 x 375/100 = 300 mg %. Therefore predicated renal threshold for glucose would be 300 mg %, however, the actual renal threshold is 200 mg % of arterial plasma or 180 mg % of venous plasma. The causes for the splay may be: i) Helerogenecity in glomerular size. ii) Variability in TMG of nephrons. 3. Renal handling of proteins, peptides and amino acids Like glucose, peptides and amino acids filter across glomerular membrane and are 100 % reabsorbed while proteins are not filtered. The small amount of protein that is present in the 29 urine usually comes from the tubular shedding. Normally up to 150 mg of proteins are excreted in urine in a day. Reabsorption of amino acids is via secondary active transport process and facilitates diffusion just like that of glucose. Fig. 19: Glucose titration curve 4. Renal handling of urea Urea is freely filtered into the glomerular filtrate. The amount of urea filtered by glomerular capillaries varies with protein intake. PCT reabsorbs 5% of filtered urea passively. DTS and ATS, CD, OMCD are totally impermeable to urea. IMCD is permeable to urea so reabsorbs large amount of urea in the effect of ADH. Urea recycling: Recycling of urea plays important role in concentration of medullary interistitium Following steps occur: i) Concentration of urea in collecting duct- As the nephrons beyond TAL till OMCD is impermeable to urea, therefore as water is reabsorbed from CD & OMCD, the urea gets more and more concentrated. ii) With the result massive and rapid reabsorption of urea occurs from IMCD into medullary interstitium. iii) From medullary interstitium, most of urea enters vasa recta and is carried upward towards renal cortex by ascending limb of vasa recta. iv) From the renal cortical interstitium, urea is secreted into the PCT of cortical nephrons. Some of the urea also enters the thin segment of the long loop of JM nephrons. In this way urea is again carried back to the IMCD from where it diffuses out again resulting in a constant recyling 5. Renal handing of uric acid Urate is freely filtered by the glomerular capillaries. Tubular transport is exclusively limited to PCT. Early PCT reabsorbs 95 % of filtered uric acid, mid PCT secrete moderate amount of uric acid equivalent to 50 % of the GF while late PCT reabsorbs moderate amount of uric acid, equivalent to 40 % of GF, called as post secretary reabsorption. 30 Mechanism – Two mechanisms are involved in the transport of uric acid: 1. Passive reabsorption through paracellular pathway. 2. Secondary active transport through transcellular pathways involves two steps – a) Across apical membrane it enters the cell by counter transport with intracellular ions like Cl-, H CO3- etc. The carrier protein is called urate transport protein. b) Across basolateral membrane, the urate moves out using another anion exchanger. Suggested Readings 1. 2. 3. Text Book of Medical Physiology by AC Guyton Fundamentals of Anatomy and Physiolgy by Martini Text Book of Physiology by AK Jain 31