Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
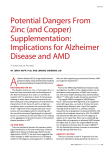
THERAPY REVIEW ■ Prevention and treatment of agerelated macular degeneration SARAH HORTON AND CATHERINE GULY Age-related macular degeneration (AMD) is a common cause of visual loss in older people and GPs play a critical role in identification and timely referral. This article discusses the features of AMD, preventing progression, treatment options, and the GP’s role in management. a Fovea Neurosensory retina Retinal pigment epithelium Bruch’s membrane b A ge-related macular degeneration (AMD) is a degenerative change of the central area of the retina (macula) in people aged 55 years and above and is the leading cause of irreversible sight loss in the developed world. The management of AMD has been transformed over the last decade with the introduction of anti-vascular endothelial growth factor (anti-VEGF) agents. Early treatment of neovascular or ‘wet’ AMD results in better visual outcomes and GPs play a critical role in the early identification and prompt referral of patients with this condition. This article will describe clinical aspects of AMD, prevention, current treatments and management of visual loss. What is AMD? AMD is a disease of metabolic dysfunction within the aging retina. Lipid and protein material accumulates beneath the retinal pigment epithelium (RPE) and within Bruch’s membrane (see Figure 1). Focal collections of lipid material are seen as ‘drusen’ on examination of the retina and morphological alteration of the RPE causes hyper- and hypopigmentation (see Figure 2). These changes form part prescriber.co.uk Figure 1. Optical coherence tomography (OCT) scans demonstrating the layers of the retina at the fovea in cross-section. The top image [a] shows healthy retina. In the lower image [b], the usually smooth profile of the retinal pigment epithelium and Bruch’s membrane is irregular due to drusen of ‘dry’ AMD. As AMD progresses, the breakdown of light-sensitive cells leads to one or more areas of well-demarcated depigmented (atrophic) RPE, described as ‘geographic atrophy’ (see Figure 3). In some patients, disordered local anatomy and biochemistr y leads to hypoxia and stimulation of new blood vessel growth through the release of angio genic growth factors (including VEGF). These abnormal blood vessels, known as a choroidal neovascular membrane, lie beneath and within the retina and can easily bleed and leak blood constituents. Prescriber January 2017 ❚ 37 ■ THERAPY REVIEW l Age-related macular degeneration Figure 2. Colour fundus photograph of a patient’s left eye: dry age-related macular degeneration with large drusen and hyperpigmentation of the retinal pigment epithelium at the macula Classification AREDS Category Clinical signs No AMD 1 None or a few small drusen (<63 microns) Early AMD 2 Any or all of the following: multiple small drusen, few intermediate drusen (63 to 124 microns in diameter), or retinal pigment epithelium abnormalities Intermediate AMD 3 Any or all of the following: extensive intermediate drusen, at least one large drusen (≥125 microns in diameter), or geographic atrophy not involving the centre of the fovea Advanced AMD 4 Geographic atrophy involving the fovea and/ or any of the features of neovascular AMD Table 1. The four-stage classification of (AMD) from the Age-Related Eye Disease Study (AREDS) Which patient groups are most susceptible? Nonmodifiable risk factors for AMD are age and genetics, while the most consistent modifiable risk factor is smoking.3,4 Patients of increasing age, current smokers and those with a family history of the condition are therefore most susceptible to the disease. There is inconsistent evidence for an association between AMD and long-sightedness, iris colour, dietary carotenoids (which make up macular pigment), alcohol intake, omega-3 and -6 fatty acid intake, obesity, hypertension, cardiovascular disease, diabetes, cataract surgery, sunlight exposure, gender and race. Figure 3. Colour fundus photograph of a patient’s right eye: advanced dry age-related macular degeneration (geographic atrophy). There is central well-demarcated geographic atrophy of the retinal pigment epithelium with visible choroidal vessels and surrounding drusen How is AMD classified? AMD is commonly described as ‘dry’ or ‘wet’ (neovascular). Wet AMD may be further subdivided based on fluorescein angiogram and occasionally indocyanine green angiography appearances into classic, occult, retinal angiomatous proliferation and choroidal polyps. There are multiple classification systems of AMD, but the Age-Related Eye Disease Study (AREDS) system has a practical application in the prescription of prophylactic vitamins (see Table 1).1,2 38 ❚ Prescriber January 2017 What are the signs and symptoms of AMD? AMD may be asymptomatic in the early stages and is often identified incidentally at a routine optometry review. In dr y AMD, patients typically describe gradual onset blurred central vision, whereas in wet AMD the onset is more rapid over days to weeks. Patients with AMD may complain of difficulty reading or of missing letters in words. Subtler symptoms include impaired light-dark adaptation (the patient may describe a central dark patch in the visual field that clears within a few minutes as they adapt) and loss of contrast sensitivity. Metamorphopsia, the perception of distorted vision (“straight lines look wavy”), is suggestive of wet AMD. Charles Bonnet syndrome, in which patients repor t formed visual hallucinations, may occur in patients with severe loss of vision. Visual acuity may be normal in early dry and wet AMD, but deteriorates with progression of the disease. Dilated examination of the retina may reveal drusen, retinal pigmentar y changes and atrophy at the macula in dry AMD. Retinal haemorrhage and subretinal fluid are seen in addition to dry changes in wet AMD. Retinal imaging techniques Ocular coherence tomography (OCT) scanning is a noninvasive imaging technique that provides a cross-sectional 3D image of the retina and can detect intraretinal and subretinal fluid in wet AMD (see Figure 4). Fundus fluorescein angiography (FFA) is used to confirm the diagnosis and establish the angiographic subtype of wet AMD. To perform FFA, fluorescein dye is injected into a peripheral vein and a series of retinal images is taken. FFA may be combined with indocyanine green angio graphy where more detailed images of the choroidal vasculature are required. This is particularly helpful for detecting choroidal polyps and retinal angiomatous proliferation, which are subtypes of wet AMD. OCT angiography is a new imaging technique that uses OCT technology to visualise the retinal and choroidal vasculaprescriber.co.uk Age-related macular degeneration ture and may be used to detect choroidal neovascular membranes. It is less invasive than FFA but not yet widely available. The treatment options NICE has published technology appraisal guidance supporting the use of specific anti-VEGF therapies in AMD and is expected to publish full guidelines on the condition in August 2017. 5,6 The Royal College of Ophthalmologists published guidelines on AMD management in 2013.7 Dry AMD Treatment of dry AMD remains limited. Specific vitamin supplementation is recommended in patients with intermediate or advanced AMD based on the a AREDS trial. This randomised-controlled trial showed that the risk of progression from intermediate to advanced AMD was reduced by around 25 per cent in participants who took zinc and antioxidant supplements.8 AREDS was followed by the AREDS2 trial, which showed there was no detriment when beta-carotene was omitted.9 Betacarotene was therefore removed from the recommended formulation (see Box 1) as it can increase the risk of lung cancer in smokers. The benefit of supplementation in early AMD remains unproven. Wet AMD NICE currently recommends the antiVEGF agents ranibizumab (Lucentis) or aflibercept (Eylea) for use in subfoveal l THERAPY REVIEW ■ choroidal neovascular membranes (see Table 2). Patients may be treated if they have a visual acuity of 6/12 to 6/96 and there is no permanent structural damage to the fovea. These agents improve vision in around a third of patients, the majority will maintain their visual acuity and around 10 per cent will not respond to therapy.7 Bevacizumab (Avastin) is an anti-VEGF agent that was developed for use in colorectal carcinoma. It is cheaper than the other anti-VEGF agents but is unlicensed for use in AMD. It is sometimes used ‘off label’. These drugs are administered as an intravitreal injection under topical local anaesthetic. This takes place as a day case in a hospital or community unit, often by nurses or trained allied health- b Macular haemorrhages Subretinal fluid Figure 4. Colour fundus photographs and ocular coherence tomography (OCT) scans of a right eye before anti-VEGF treatment [a]; and after anti-VEGF treatment [b]. There is resolution of the macular haemorrhages and subretinal fluid prescriber.co.uk Prescriber January 2017 ❚ 39 ■ THERAPY REVIEW l Age-related macular degeneration 500mg vitamin C 400IU vitamin E 80mg zinc oxide 2mg copper ± lutein and zeaxanthin Box 1. Currently recommended dietary supplementation for patients with intermediate or advanced age-related macular degeneration care professionals. Clinical trials administered monthly injections for 24 months. In the NHS, injections are usually administered monthly for three months. After this, treatments are either given each month as a PRN (when required) regimen or as part of a treat and extend regimen, ie treat monthly until stable and then extend the treatment interval each time the patient is stable up to an injection once every three months. Treatment is then withdrawn after a period of stability or treatment failure. Potentially serious adverse events occur in <0.1% of intravitreal injections and include endophthalmitis, retinal detachment and cataract. Systemic antiVEGF agents confer an increased risk of events classified as arterial thrombo embolism (ATE), including myocardial infarction and stroke. There may be a small increased risk of these events in patients who receive intravitreal anti-VEGF agents. The MARINA trial demonstrated an ATE rate of 4.6% in recipients of ranibizumab versus 3.8% in recipients of a sham injection at 24 months; however, this was not statistically significant.10 Photodynamic therapy is rarely used but is an option in patients with choroidal polyps. Macular Society www.macularsociety.org 0300 3030 111 What is the GP’s role in management? NHS low vision support http://www.nhs.uk/Livewell/ Eyehealth/Pages/Livingwithlowvision. aspx The rapid onset of central distortion in an older adult should be considered AMD until proven otherwise. GPs ought to make an urgent referral to a local optometry or hospital retina service, depending on local structuring of services. The Royal College of Ophthalmologists has developed a “Wet AMD rapid access referral” form for optometrists and GPs.15 GPs may provide advice on how to slow progression of the disease. Patients who smoke should be suppor ted in smoking cessation. Patients should be advised to eat a diet rich in dark green leafy vegetables and on the benefits of vitamin supplementation in intermediate and advanced AMD. Complications of intravitreal injections are rare but potentially sight threatening. Drug name Mode of action Key relevant trials NICE approved? Ranibizumab (Lucentis) Humanised Fab fragment of a monoclonal antibody that binds to and inhibits the action of all isoforms of VEGF-A MARINA10 ANCHOR11 (superiority studies against sham injection) Yes Aflibercept (Eylea) Fusion protein that inhibits all isoforms of VEGF-A and placental growth factor VIEW1/VIEW212 (noninferiority studies against ranibizumab) Yes Bevacizumab (Avastin) Humanised full-length monoclonal antibody derived from the same antibody as ranibizumab. Likely to bind to all the same isoforms of VEGF-A as ranibizumab, but with a different affinity CATT13 IVAN14 (noninferiority studies against ranibizumab) No VEGF-A = vascular endothelial growth factor A Table 2. Properties of antiangiogenic therapies for wet age-related macular degeneration 40 ❚ Prescriber January 2017 Royal National Institute for the Blind (RNIB) www.rnib.org.uk 0303 123 9999 DVLA https://www.gov.uk/guidance/visualdisorders-assessing-fitness-to-drive Box 2. Sources of information and support for patients with age-related macular degeneration Patients who present with reduced vision following an intravitreal injection should be referred to an eye casualty unit or discussed with an on-call ophthalmologist. GPs can signpost relevant charities or low vision services for practical advice and emotional support (see Box 2). Clinicians must be vigilant to the development of depression, as visual impairment in older people is associated with a higher than normal risk of depression.16 Referral to an ophthalmologist for registration of visual impairment should be considered for patients with a visual acuity of 6/60 or worse in both eyes. Drivers with a car or motorcycle licence require visual acuity of 6/12 or better with both eyes open and patients should be advised to contact the DVLA if their corrected visual acuity is below the threshold for driving. Conclusion AMD is a common cause of visual loss in older people. Intravitreal anti-VEGF injections are the mainstay of treatment for wet AMD. In patients with intermediate or advanced AMD, vitamin supplements may slow progression. GPs play a critical role in identification and timely referral, facilitating smoking cessation and enabling patients to access support services for the visually impaired. References 1. Ferris FL, et al. Clinical classification of age-related macular degeneration. Ophthalmology 2013;120(4):844–51. prescriber.co.uk Age-related macular degeneration 2. Age-Related Eye Disease Study Research G. The Age-Related Eye Disease Study system for classifying age-related macular degeneration from stereoscopic color fundus photographs: the Age-Related Eye Disease Study report number 6. Am J Ophthalmol 2001; 132(5):668–81. 3. Tan JS, et al. Smoking and the long-term incidence of age-related macular degeneration: the Blue Mountains Eye Study. Arch Ophthalmol 2007;125(8):1089–95. 4. Chakravarthy U, et al. Clinical risk factors for age-related macular degeneration: a systematic review and meta-analysis. BMC Ophthalmol 2010;10:31. 5. NICE. Ranibizumab and pegaptanib for the treatment of age-related macular degeneration. TA155. August 2008. Last updated: May 2012. www.nice.org.uk/guidance/ta155 6. NICE. Aflibercept solution for injection for treating wet age-related macular degeneration. TA294. July 2013. www.nice.org.uk/ guidance/ta294 7. Royal College of Ophthalmologists. Agerelated macular degeneration: guidelines for management. September 2013. www.rcophth. ac.uk/standards-publications-research/ clinical-guidelines 8. A randomized, placebo-controlled, clinical trial of high dose supplementation with vitamins C and E, beta carotene, and zinc for age-related macular degeneration and vision loss: AREDS report no. 8. Arch Ophthalmol 2001;119(10):1417–36. 9. Age-Related Eye Disease Study 2 Research Group. Lutein + zeaxanthin and omega-3 fatty acids for age-related macular degeneration: the Age Related Eye Disease Study 2 (AREDS2) randomized clinical trial. JAMA 2013;309(19):2005–15. 10. Rosenfeld PJ, et al. Ranibizumab for neovascular age-related macular degeneration. New Engl J Med 2006;355(14):1419–31. 11. Brown DM, et al. Ranibizumab versus ver teporfin for neovascular age-related macular degeneration. New Engl J Med 2006;355(14):1432–44. 12. Heier JS, et al. Intravitreal aflibercept (VEGF trap-eye) in wet age-related macular degeneration. Ophthalmology 2012;119(12):2537–48. 13. Mar tin DF, et al. Ranibizumab and bevacizumab for neovascular age-related l THERAPY REVIEW ■ macular degeneration. New Engl J Med 2011;364(20):1897–908. 14. Chakravarthy U, et al. Ranibizumab versus bevacizumab to treat neovascular age-related macular degeneration: one-year findings from the IVAN randomized trial. Ophthalmology 2012;119(7):1399–411. 15. Royal College of Ophthalmologists. Wet AMD rapid access referral form. https://www.rcophth.ac.uk/wp-content/ uploads/2015/04/2010-SCI-048-AMDElectronic-Referral-Form-edited.pdf 16. Evans JR, et al. Depression and anxiety in visually impaired older people. Ophthalmology 2007;114(2):283–8. Declaration of interests None to declare. Dr Horton is a medical ophthalmology specialty registrar and Dr Guly is a consultant ophthalmic physician, University Hospitals Bristol NHS Foundation Trust POEMs Single-dose dexamethasone an option for acute adult asthma Clinical question: Is a single dose of dexamethasone as effective as five days of prednisone for acute exacerbations of asthma? Bottom line: A single dose of 12mg dexamethasone, which has a longer duration of action than prednisone, is almost as effective as five days of 60mg prednisone for the prevention of relapse in adults with acute asthma treated in a emergency department. It is a reasonable option for treatment in the emergency department, given its fewer side-effects. In this study, patients who received the single dose also took placebo for four days; further research is needed to determine whether patients are comfortable with taking just a single dose. (LOE = 2b) Reference: Rehrer MW, et al. A randomized controlled noninferiority trial of single dose prescriber.co.uk of oral dexamethasone versus 5 days of oral prednisone in acute adult asthma. Ann Emerg Med 2016;68(5):608–13. Study design: Randomised controlled trial (double-blinded). Funding source: Foundation. Allocation: Concealed. Setting: Emergency department. Synopsis: These investigators enrolled 456 adults younger than 56 years who presented with acute asthma to an emergency department and required at least one treatment with a beta-agonist. The patients were randomly assigned, using concealed allocation, to receive treatment with prednisone 60mg daily for five days or a single dose of dexamethasone 12mg followed by four days of placebo. Treatment was started in the emergency department. Of the 456 people initially enrolled, 376 could be evaluated; 16 were admitted before leaving the emergency department and 73 could not be contacted (more in the dexamethasone group). Over the subsequent two weeks, 12.1% of the dexamethasone group and 9.8% of prednisone group had a relapse that required additional treatment (difference 2.3%; 95% CI -4.1% to 8.6%). This difference did not meet the researchers’ threshold for noninferiority of 8%, meaning that treatment with dexamethasone was slightly less effective. The hospitalisation rate was low (3%) and did not differ between treatment groups. Side-effects were more common in the prednisone group. POEM (Patient Orientated Evidence that Matters) editors review more than 1200 studies monthly from over 100 medical journals, presenting only the best as Daily POEMs. For more information visit: www.essentialevidenceplus.com Prescriber January 2017 ❚ 41