Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Remote ischemic conditioning wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Cardiac surgery wikipedia , lookup
Jatene procedure wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
Electrocardiography wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
Atrial fibrillation wikipedia , lookup
1357
Inappropriate Sinus Tachycardia After Radiofrequency
Ablation of Para-Hisian Accessory Pathways
CARLO PAPPONE, M.D., GIUSEPPE STABILE, M.D..^^ GIUSEPPE ORETO. M.D.,**
ANTONIO DE SIMONE, M.D.,* MARIANO RILLO, M.D.,
PATRIZIO MAZZONE, M.D., RICCARDO CAPPATO. M.D.,t
and SERGIO CHIERCHIA. M,D.
From the Cardiology Department, Hospital San Raffaelc. Milan; ^Laboratory of Electrophysiotogy,
Clinica San Michele. Maddaloni. Caserta; **Department of Cardiology. University of Messina. Messina. Italy;
and tAllgemeines Krankenhaus St. Georg, II Medizinische Abteilung, Hamburg, Germany
I n a p p r o p r i a t e S i n u s T a c h y c a r d i a After C a t h e t e r A h l a t i o n . Introduction: Inappropriate sinus tachycardia (IST) has been observed following radiofrequency ablation (RFA) of
the AV nodal fast patbway. This study was aimed to prospectively analyze tbe incidence and
clinical signiticance of IST following RFA of para-Hisian accessory patbways (APs).
Methods and Results: Twenty-eight patients (pts) with para-Hisian APs underwent RFA. An
AP was defined as para-Hisian whenever its atrial and ventricular insertions were associated
witb a His-bundle potential > 0.1 mV. RF current was always delivered at tbe atrial aspect of
tbe tricuspid annulus. to a site where tbe His-bundle potential was < 0.15 niV. Time- and frequency-domain analysis of beart rate variability was performed in 22 patients, before and after
RFA. Abolition of AF conduction was obtained in all pts, and no AV conduction alteration occurred. Six pts (21.4%) presented witb IST 45 to 240 minutes after the ablation procedure. In 5
of tbem, IST disappeared spontaneously within 72 bours, wbereas in I pt ^-blockers were required for 2 montbs. The atrial potential amplitude (1.217 ± 0.264 mV vs 0.882 ± 0.173 mV, P =
0.009) and AA' potential amplitude ratio (2.633 vs 1.686, P = 0.05) were significantly higher in
pts wbo developed IST than in those who did not. A marked decrease in heart rate variability
was observed only in pts wbo developed IST.
Conclusion: IST is a relatively frequent complication after RFA of para-Hisian APs: it is
generally sbort-lasting and usually does not require any treatment. IST after catbeter ablation
is likely to depend upon transient parasympatbetic denervation of the sinus node, (f Cardiovasc
Electrophy.siol, Vol. 8, pp. 1357-1365, Decemher 1997)
accessory pathways, arrhythmias, catheter ablation, heart rate variability, preexcitation, sinus node,
tachycardia
Inappropriate sinus tachycardia (IST)—a tachycardia that is excessive with respect to the level of
physical or psychological stress^—has been observed
following radiofrequency ablation (RFA) of the
AV nodal fast pathway.'- Although the exact mechanism leading to this tachycardia is still debated, a
common explanation is that IST is caused by interruption of vagal fibers that are en tx>ute to the sinus
node through the AV nodal region.- If that were
the case, this cotnplication also should tx:cur after
ablation of accessory pathways (APs) close to tbe
His bundle or located in the anterior part of the AV
nodal region. The aim of this study was to
prospectively analyze the incidence and clinical significance of IST following RFA of para-Hisian^ APs.
Address for correspondence; Carlo Pappone. M.D.. Cardiology
Department. Hospital San Raffaele. Via Olgettina 60, 20132 Milano. Imly. Fax: 39-2-264-37398.
Methods
Manuscript received 26 August 1997; Accepted for publication 13
October 1997.
Twenty-eight of 737 patients (3.8%) referred to
our institutions between September 1992 and June
Introduction
1358
Journal of Cardiovascular Electrophysiology
Vol. 8. No. 12. Decetnber 1997
III
ACp
ACp
ACd
ACd
RVA
RVA
200 mm/s
200 mm/s
B
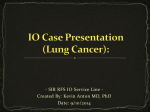
Figure 1. Patient / / with an overt accessory pathway. Surface and intracardiac electrograms recorded at the ablation site
before (A) and after (B) RF detivery. Before RF. the ahtotion catheter does not record a distinct His-bundle potential.
whereas after abolition of accessory pathway conduction a clear His-bundle potential is recorded, with an amptitude of 0.1
mV and an A/V amptitude ratio of 1.8, HRA = high right atrium; HIS = His bundle: CS = coronary sinu.s; AC = ablation
catheter: RVA = tight ventricular apex: p = proximal electrode pair: d = distal electrode pair.
1996 for RFA of APs had an AP located in the
para-Hisian region. Seven of the patients were male
(mean age 26.2 ± 7.1 years, range 15 to 37); none
had underlying heart disease. Twenty-five had an
overt pathway and three a concealed AP.
Electrophysiologic Study and Catheter Ablation
After giving written informed consent, all patients underwent electrophysiologic study and catheter ablation in a single session, while in Ihe fasting state, after discontinuation of all antianhythmic drugs for at least five half-lives. Four
quadripolar standard 6-French catheters with an
interelectrode spacing of 2 or 5 mm were inserted through the right or left femoral vein and
the left subclavian vein. The electrtxies were placed
in the high right atrium, at the AV Junction (Hisbundle recording site), in the right ventricular apex,
and in the coronary sinus. Mapping and ablation
of APs were performed using a steerable 7-French
quadripoiar catheter (Webster Laboratories, Watertown. MA, USA) wilh a 4-mm tip and 2-mm
interelectrtxle spacing. This catheter was inmxiuccd
via the right femoral vein in 24 patients and via
the right subclavian vein in 4. Leads I, III. and V,,
and intracardiac electrograms were recorded simultaneously u.sing a multichannel recorder (Midas, PPG Biomedical Systems. Overland Park, KS,
USA; or Bard-USCI, Billerica. MA, USA), in unipolar and bipolar fashion, after tiltering at 30 to
500 Hz. Mapping o\' manifest APs was performed
during sinus rhythm or atrial pacing, whereas mapping of concealed APs was peribnned during orthodromic recipnx-ating tachycardia or during right
ventricular pacing. The peak-to-peak amplitude of
bipolar electrograms was measured to detennine
the amplitude of atrial, ventricular, His-bundle. and
AP potentials. Whenever identification of the Hisbundle activation potential in the anteroseptal re-
Pappone, et al.
Inappropriate Sinus Tachycardia After Catheter Ablation
1359
III
in
V!
VI
V
HRA lo
HRA la
HLSp
IIISp
HIScl
MLS d
CSp
CSp
CSd
CSd
ACp
ACp
ACtl
RVA
RVA
!OOmm/s
lOOmm/s
B
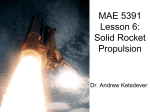
Figure 2. Patient 7 with a concealed accessory pathway. Surface and intracardiac electrograms recorded at the ablation site
during AV reentrant tachycardia before (A) and after (B) RF delivery, during sinus rtiythm. The His-bundle potential amplitude is 0.15 mV. witti an AN amptiliide ratio of 2.3. Abbreviations as in Figure L
gion was expected to be obscured by the presence
of a preexcited local ventricular potential, premature extrastimuli were delivered from the high right
atrium in the attempt to tlnd the AP refractory, in
order to analyze the AV conduction sequence of
nonpreexcited beats. An AP location was defined
as para-Hisian whenever the atrial and ventricular insertions of the AP were associated with a
large His-bundle potential > 0.1 mV.' For manifest APs. the optimal site for RF application was
selected on the basis of: (1) the shortest A-V interval; (2) a Va-QRS > 0 msec; (3) the presence
of a Kent potential; and (4) electrogram stability
and continuous electrical activity (CEA) t>etween
atrial and ventricular activation potentials-* (Fig. I).
For concealed APs. the optimal ablation site was
characterized by: (1) the shortest V-A interval; (2)
the Kent potential; and (3) the electrogram stability and CEA^ recorded during orthodromic tachycardia (Fig. 2). RF current was always delivered
at the atrial aspect of the tricuspid annulus^'' to a
site where the amplitude of the His-bundle potential was < 0.15 mV. RF energy was delivered as
a continuous, unmodulated sine wave at 5(X) Hz
(RFG 3C. 3D Radionics. Inc., Burlington, MA.
USA) between the distal electrode of the ablation
catheter and a large skin electrode Itxiated on the
posterior chest, at a power setting of 15 to 25 W.
In the last 18 patients, RF delivery was guided
by temperature monitoring at a temperature setting
of 50°C. Application of energy was stopped if AP
block did not occur within 10 seconds, or if sustained Junctional rhythm appeared during energy
delivery.
Postablation and FoUow-Up Evaluation
Sixty minutes after ablation, all patients underwent a control electi ophysiologic study, under basal
conditions and during isoproterenol infusion. Before discharge from the hospital (usually 36
hours after ablation), an ECG, chest X-ray, echocar-
1360
Journal of Cardiovascular Electrophysiology
Vol. 8. No. 12, December 1997
^ 2
S Sa
=1
tr
o
'•3
— -
OC
_
o-
i O ' lo"^: -• r)q r*^
'^ ^
X ^"^ '^'
— -^
PJ° o-; g) —
m
in
m
14
s
-t
—
—
n
—
—
—
—
c
I II
u
2
on
? ' S
_
a*
3 C 5
>
r-i
r
o
—
o
r i r ^ ,
ri
c
r-;
c
r-
c
c
o
o
r
o
d
- < t » n N 0 t ~ - 0 0 0 \ O
—
~
o
—
o
P
o
>q
—
Pappone etat
c
o^
oc
n
00
c
•9
ON
2 Ci
3.
ct n
o
"ra
£
U
C
ON
ri
n
o
^o
•*- t ;
0 —
u
?j 3
-^K £
1^
3
"ra
ra
> II U
'-'
:hm =
- puls
X
ON
in
ra ra c;
2 w
•r JJ -^
- «, R "j
!l" =
c; c in "O S CO I'
2 C CO "^
= -o ca S^
—
fN
—
—
—
—
Inappropriate Sinus Tachycardia After Catheter Ablation
1361
diogram, and 24-hour Holter monitoring were perfomied in all patients. Those who showed 1ST underwent Holter monitoring 3 and 30 days after the
procedure. During a 1-year follow-up, all patients
underwent a control visit every 3 months.
Definition of 1ST
The reeognition of 1ST was based on both
symptoms and evidence of tachycardia in one of
the routine ECGs recorded with the patient in
the supine position while resting in bed 2 and 4
hours after discharge from the cardiac catheterization laboratory. 1ST was diagnosed if the following were present^-^: (1) P wave axis and morphology during tachycardia identical or very similar to those during sinus rhythm; (2) resting heart
rate > 1(X); (3) exclusion of secondary causes of
sinus tachycardia; and (4) palpitations associated
with sinus tachycardia.
Patients were divided into two groups: (1} those
who developed 1ST (group 1); and (2) those who
did not develop 1ST (group 2). The prevalence of
1ST was evaluated in the group of patients with
para-Hisian AP and compared with that observed
in a group of 167 consecutive patients with midseptal, right posteroseptal, and right anterior APs
refeired for ablation during tlie same period.
A V Conduction
To assess the effect of RF pulses on AV conduction, the preablation measurements of AH interval and Wenekebach point were compared with
those observed obtained after ablation. Since
changes in these parameters may be influenced by
their basal values, nomialized values were calculated as follows.
Normalized AAH (N AAH)
= AH after ablation - AH before ablation/
u —
-r
AH before ablation
> e "u
Normalized AWP (N AWP)
O
•—
O
C
O
C
—'
= WP after ablation - WP before ablation/
--S 5
o ra n
WP before ablation
'5 o
3 jj y c
%X •^^
O^
o
d
—
d
oc
q
d
—
d
—
d
p
c
o =! =! .E
^ .2 .2 1
S SS o
< ra a c
Sympathovagal Balance
The sympathovagal balance was assessed in 22
patients by time- and frequency-domain analysis
of heart rate variability calculated from 24-hour
Holter tape recordings. Holter monitoring was per-
1362
Journal of Cardiovascular Electrophysiology
Vot. 8. No. 12, December 1997
TABLE 2
Clinical Characteristics of Patients Developing Inappropriate Sinus Tachycardia (1ST)
After Para-Hisian Accessory Pathway Abiation
Baseline Rate*
1ST Rate§
Duration of 1ST
Pt. No.
Age/Sex
(beats/min)
(beats/min)
(hours or days)
Treatment
4
21/F
78
[M)
.16 h
None
84
7
37/M
135
60 d
P-blocker
70
8
24/F
125
48 h
None
66
16
19/M
144
48 h
None
68
21
22/M
132
48 h
None
72
23
29/F
124
36 h
None
•Baseline rate is ihe rale observed in ihe admission ECG; §1ST rate is the heart rale in ihe first p<jstablalion HCG (recorded
within 4 hours from the procedure) that revealed 1ST.
formed upon admission, and 6 hours after ablation, using a two-channel Holter recorder, and was
evaluated semiautomatically (Oxford Medilog Excel. Abingdon, United Kingdom; and Delmar
Avionics, Irvine, CA, USA). Heart rate variability was analyzed from the Holter recordings using a commercially available software algorithm
(Delmar Avionics). Of the various time-domain
indexes of heart rate variability, we evaluated the
MSSD (root mean square of difference of successive RR intervals) and the PNN50 (percentage
of adjacent RR intervals that differed by > 50
msec).'' Power spectral analysis was perfonned by
a fast Fourier transform algorithm producing a
spectrum for the 0.01- to 1.0-Hz frequency band.
Low-frequency (LF) power (0.04 to 0.15 Hz) and
higb-frequency (HF) power (0.15 to 0.4 Hz) spectra were obtained, and the LF/HF ratio'"" was calculated.
Statistical Analysis
Data are presented as mean ± 1 SD, when appropriate. Differences between groups were ana-
lyzed using the Student's /-te.st. P < 0.05 was considered statistically significant.
Results
Permanent abolition of AP conduction was
obtained in all patients. The mean number of RF
pulses required to induce AP conduction bkx:k was
3.2 ± 1.9 (range 1 to 8). The time between the onset of RF delivery and AP conduction block (ablation time) ranged between 1.3 and 5.4 seconds
(mean 2.9 ± 1.1). The mean time of the ablative
procedure was 148.6 ± 30.3 minutes, with an average fluoroscopy time of 25.3 ± 5.8 minutes.
Table 1 shows the characteristics of the electrograms recorded at successful ablation sites and
parameters relative to RF current effects on AV
nodal conduction. Six patients (21.4%) developed 1ST 45 to 240 minutes after tbe ablation procedure (Table 2). In five of them tbe aiThythmia
subsided spontaneously within 72 hours, whereas
in one patient 1ST lasted about 2 months and required drug therapy (atenolol, 100 mg o.d.) to re-
TABLE 3
Electrophysiologic Parameters. Electrogram Characteristics at Successful Ablation Sites,
and Holler Monitoring Data in Group I and Group 2 Patients
His-bundle potential amplitude {mV)
Atrial poteniial amplitude (mV)
Ventricukir potential amplitude (mV)
A/V ratio
N AAH
N AWP
RBBB (Pts)
A V Junctional Rhythm (Pts)
RF pulses
Ablation time (sec)
Holter average heart rate
Holter minimal heart rate
Holter maximal heart rate
Abbreviations a.s in Table 1.
Group 1
0.11 1 ± 0.029
1.217 ±0.264
0.467 ± 0.082
2.633 ± 0.463
3.62%
1.65%
1/6(16.7%)
4/6 (66.7%)
5.25 ± 1.9
3.92 ± 0.95
100.8 ± 6
77.0 ± 7.2
147.5 ± 8.1
Group 2
0.092 ± 0.026
0.882 ± 0.173
0.557 ±0.158
1.686 ±0.531
4.27%
1.44%
6/22 (27.3%)
5/22 (22.7%)
2.27 ± 1.24
2.63 ± 0.74
69.6 ± 11
4.S.6 ± 7
101.2 ± iO.S
l>
0.1 .^
0.0009
0.2
o.oo.s
o.«
0.7
0.6
0.04
0.04
0.01
<O.(X)OI
<0.0(H)1
<O,()(H)I
Pappone, et at.
Inappropriate Sinus Tachycardia After Catheter Ablation
duce the heart rate. Among control patients, only
1 of 167 (0.3%) exhibited 1ST that lasted 36 hours.
Table 3 summarizes the electrophysiologic parameters and electrogram characteristics at ablation sites in groups 1 and 2. His-bundie potential
amplitude, atrial potential amplitude, and AV amplitude ratio aie significantly higher in patients who
developed 1ST than in those who did not. There
was no significant change in AV conduction parameters (N AAH and N AWP) in both groups.
With respect to group 2, patients of group I showed
a higher incidence of A-V junctional rhythm during RF delivery, a higher number of RF pulses,
and longer ablation times. Only 1 patient of group
1 (16.7%) developed right bundle branch block
(RBBB) after RF ablation, whereas 6 (27.3%) group
2 patients showed RBBB after RF ablation.
Table 4 summarizes the results obtained by timeand frequency-domain analysis of Holter recordings obtained before and after ablation. Compari.son of pre- and postablation time-domain analysis
revealed a .significant decrease in heait rate variability, expressed as MSSD and PNN50, in patients who developed 1ST. In these patients, frequency-domain analysis revealed a significant
poslablation increase of LF/HF ratio, due to marked
attenuation of the HF component. Time- and frequency-domain analysis pertbmied in group 1 patients 30 days after ablation revealed resolution of
such abnormalities, except for patient 7, in whom
normalization occurred after 2 months. No signif-
1363
icant acute and chronic modifications in time- and
frequency-domain parameters were observed in
group 2 patients.
There were no short-term or late complications related to the ablation procedure, apart from
RBBB. During a mean follow-up period of 22 ±
13 months, all patients were free of arrhythmias,
and none developed transient or (persistent PR prolongation. In the 25 patients with overt APs, serial ECGs failed to show preexcitation.
Discussion
The present study provides a clinical model for
the study of 1ST that follows RFA. The major findings are that: (1) the occurrence of 1ST is direcdy
related to the characteristics of the electrogram
recorded at the ablation site (the amplitude of the
atrial potential and the AfW ratio); and (2) development of 1ST is associated with a marked decrease
in the parasympathetic drive to the sinus node.
Mechanism of Postablation 1ST
1ST has been described as a possible complication following RFA of the AV nodal fasl pathway
in patients with AV nodal reentrant tachycardia, but
has never been repoited following RFA of the slow
AV nodal pathway. It has been proposed that the
transient increase in sinus rate associated with fast
AV nodal pathway ablation may depend ujxm ei-
TABLE 4
Acute and Chronic Changes in Time- and h'i-et|uency-Domain indexes
of Heai-i Rale Variability After RadLorret|Lieney Abtalion
Before
Ablation
6 Hours After
Ablation
P
301)ay,s After
Ablation
Group 1 (n = 5 )
MSSD (msec)
27.2 ± 6.61
17.2 ± 6 . 9 1
0.OOO09
24.8 ± 6 , 1 4
PNN50 {%)
7.1 ± 3.1
4,1 ± 1.8
0,01
6,9 ± 2.9
HF power (msec)
346 ± 29
251 ± 37
0.008
340 ± 30
LF/HF
2.82 ± 0.64
3.96 ± 0,46
0.0003
2,78 ± 0.65
P
O.(X)01*
0.()09t
0.01*
0.3t
0.012*
0.14t
0,02*
0.77t
Group 2 (n = 17)
MSSD (msec)
26,7 ± 4.95
26.1 ± 4,4
0.13
PNN50 (%)
7. II ± 1,4
7.06 ± 1.3
0,51
7.15 ± 1.4
HF power (msec)
348 ± 30
346 ± 31
0.62
349 ± 29
LF/HF
2,91 ± 0 . 5 4
3.01 ± 0,62
0.28
2,95 ± 0.5
26 ± 4,42
0.87*
0.14t
0.42*
0.18t
0.36*
0.59t
0,5*
MSDD = root mean square of differences of successive RR intervals; PNN50 = percentage of adjaceni RR intervals ihat
differ by > 50 msec; HF = high frequency; LF = low frequency. *P value between 6 hours and 30 days afier ablalion; fP
value belween before ablation and 30 days after ablation.
I .^64
Journal of Cardiovascular Electrophysiology
Vol. ^. No. 12. Decetnber 1997
ther the hemodynamic impairment associated
with prolongation of the AV conduction time'^ or
the acute damage of parasympathetic fibers caused
by the thermocoagulative lesion. Morillo et ai.^
Imported a markedly depressed cardiovagal response
in all patients with post-RF 1ST. and suggested that
the sinus ntxle response to efferent vagal stimulation was impaired. Although little is known about
the functional anatomy of autonomic innervation
of the human heart, some studies"'^ have shown
that postganglionic parasympathetic fibers that innervate the sinoatrial node mn across the region of
the AV node. It has been assumed''' that RF current applied to the region of the AV node may damage these fibers and cause a decrease in parasympathetic control of sinus node activity. In the present study, both time- and frequency-domain indexes
of heart rate variability suggest the occun^ence of
parasympathetic denervation of the sinus node
immediately after ablation. Since these abnormalities disappeared in one patient after 2 months,
the possibility of reinnervation may be taken into
account.'^ Our data are in agreement with those of
Kocovic et al..'' who found the most striking abnormalities of heart rate and heart rate variability
in patients in whom alterations of AV nodal function were induced by RF energy. They suggested
that most of parasympathetic ganglia and postganglionic parasympathetic fibers lie in the midand anterior portions oi" the low interatrial septum,
namely in the region that represents the target for
RF pulse energy delivery in fast AV nodal pathway ablation. In the present study, the cK-currence
of 1ST following ablation of piira-Hisian APs was
directly related to the amplitude of the atrial potential and the A/V ratio, suggesting that the more
"atrial" the lesion directed to the region of tricuspid annulus, the greater the likelihtmd of affecting
the autonomic balance of the sinus node.
The low incidence (0.6%) of 1ST following RF
ablation of mid-septal, right posteroseptal. and right
anterior APs is a further confirmation that vagal
fibers en route to the sinus node run through the anterosuperior region of the interatrial septum, i.e., relatively far from the target for ablation of these APs.
Clinical Significance of 1ST
In the present study. 1ST occuired in 21.4% of
patients undergoing ablation of a para-Hisian AP.
This value is in agreement with those reported in
patients undergoing ablation of the fast AV nodal
pathway.'- However, none of our patients who developed this arrhythmia exhibited a procedure-re-
lated prolongation of atrio-Hisian conduction. This
finding makes it unlikely that 1ST is due to the
acute hemodynamic imbalance that may follow a
lack of optimal coordination of atrial and ventricular contraction." In some patients, the arrhythmia
was associated with symptoms resembling those
of AV reentrant tachycardia; in all cases but one.
however, 1ST did not require any treatment.
Approach to Para-Hisian AP Ablation
In this study, ablation of piu-a-Hisian APs has
been obtained by applying RF energy to the atiial
aspect of the tricuspid annulus ("atrial" approach),
as reflected by an AA' electrogram ratio > I in any
case. This does not automatically mean that the
"atrial" approach is better than the "ventricular"
one in ablation of para-Hisian or anteroseptal APs.
Our choice was dictated by the experience we developed with such a type of procedure, but it is obvious that the "ventricular" approach may be as
successful as the "atrial" one in experienced hands.
The data reported in the present research suggest that a more "atrial" lesion is associated with
a relatively high incidence of 1ST, whereas a more
"ventricular" (or less "atrial") lesion results in a
higher incidence of RBBB. The occurrence of
RBBB associated with the "ventricular" approach
is explained by application of RF energy to a site
close to the right bundle bnmch. which can be diunaged unintentionally. This is shown in Table 3. The
average AA' electrogram ratio is 2.633 in group 1
(1ST patients), whereas it is 1.686 in group 2 (noIST patients). The incidence of RBBB is higher in
group 2 (27.3%) than in group I (16.7%), altliough
the ditference is not statistically significant due to
the limited number of cases.
Study LAtnitatiom
There are several potential limitations of this
study. (1) The number of patients included is relatively small. (2) The anxiety related to cardiac
catheterization may result in increased sympathetic
tone, which could increase the sinus rate and decrease heart rate variability. (3) Although the arrhythmia was probably related to reduced paRLsympathetic tone in our patients, we cannot rule out
the possibility that a relative increase in sympathetic acfivity. related to the RF lesion itself, might
have been responsible for it. (4) We did not use
alternative autonomic function tests, such as the
cold face or isoproterenoi sensitivity, to assess
the mechanism of 1ST
Pappone, et at. Inappropriate Sinus Tachycardia After Catheter Ablation
Conclusion
1ST is a relatively frequent occurrence after RF
catheter ablation of para-Hisian APs. It generally
terminates spontaneously within a short time and
usually does not require any treatment. The occurrence of 1ST is directly related to the amplitude
of the atriaJ potential and to the AA' amplitude ratio in the electrogram recorded at the successful
ablation site. It also appears to be related to the
number of RF pulses and to the time between the
onset of the RF pulse and permanent abolition of
AP conduction, whereas it does not appear to be
dependent upon alterations in AV conduction. The
development of 1ST after catheter ablation is likely
to be the expression of transient parasympathetic
denervation of the sinus node.
Achuwtedgment: The aulhors acknowledge Dr. Francesco FraioH,
Reseiirch Fellow in Computer Science. Division of Cardiology, IslitulD Scientifico San Rafliiele. Milan, for his outstanding contribiition to the statistical analysis of the data.
References
1. Ehlert FA. Goldberger JJ. Brooks R. el al: Persistent
inappropriate sinus tachycardia after radiofrequency
current catheter modification of the atrioventricular
node. Am J Cardiol 1992;69:I{)92-1095.
2. Skeberis V, Simonis F. Tsakonas K, et al: Inappropriate sinus tachycardia following radiofrequency ablation of AV nodal tachycardia: Incidence and clinical
significance. PACE 1994;17:927-934.
3. Haissaguerre M. Markus F. Poquet F, et al: Electrocardiographic characteristics and catheter ablation of
parahissian accessory pathways. Circulation 1994:90:
1124-1128,
4. Calkins H. Kim YN. Schmaltz S, et al: Electrogram
criteria for identification of appropriate target sites for
radiofrequency catheter ablation of accessory atrioventricular connections. Circulation 1992;85:565-573.
1365
5. Kuck KH. Friday KJ. Kunze KP. et al: Sites of conduction block in accessory atrioventricular pathway: Basi,s
for concealed acces.sory pathways. Circulation 1990;
82:407-417.
6. Schluter M. Kuck KH: Catheter ablation from right
atrium of anteroseptal accessory pathways using radiofrequency current. J Am CoU Cardiol 1992;19:663670.
7. Morillo CA. Klein GJ, Thakur RK. et al: Mechanism
of "inappropriate" sinus tachycardia: Role of syinpathovagal balance. Circulation 1994;90:X73-877,
S. Lee RJ. Kalman J. Fitzpatrick AP, et al: Radiofrequency
catheter modification of the sinus node for "inappropriate" sinus tachycardia. Circulation 1995:92:2919-2928,
9. Kocovic DZ. Harada T, Shea JB. et al: Alieraiions of
beart rate and heart rate variability after radiofrequency
catheter ablation of supraventricular tachycardia. Oelineation of parasympathetic pathways in the human
hean. Circulation 1993;88:1671 -1681,
10. Fallen EL, Kamath MV. Ghista DN: Power spectrum o!"
heart rate variability: A noninvasive lest of integrated
neurocardiac function. Clin Invest Med 1988:2:331-340.
11. Malliani A. Pagani M. Lombardi F. et al: Cardiovascular neural regulation explored in the frequency dntiialn.
Circulation 1991:84:482-492.
12. Haskell RJ, French WJ: Optimum AV interval in dual
chamber pacemakers, PACE 1986:9:670-675.
13. Motomura S. Iijima T. Taira N: Cholinergic innervation in intracardiac autonotiiic nerves in atrioveniricular junctional area. Am J Physiol 1980;239(Heart Circ
Physiol 8):HI81-HI88.
14. Forgsen S: The distribution of sympathetic nerve fibers
in the AV node and the AV bundle of the bovine heart.
Hi.stochemJ 1986; 18:625-638.
15. Randall WC, Ardell JL: Nervous control of the heart:
Anatomy and pathophysiology. In Zipes DP. Jalife J,
eds: Cardiac Electrophysiology: From Celt to Bedside.
WB Saunders Co.. Philadelphia. 1990. p, 291.
16. Racker D: Atrioventricular node and input pathways;
A correlated gross anatomical and histologicai study of
the canine atrioventricular junctional region. Anat Rec
1989;224:336-354.