Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
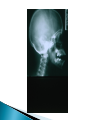
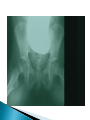
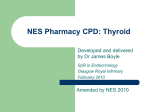
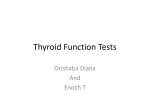
Rob Lindsay, MD Adjunct Professor of Pediatrics University of Utah School of Medicine 10 year old girl with documented autoimmune (Hashimoto) thyroiditis and hypothyroidism. Her initial TSH was > 1000mU/L. Type 1 Diabetes Mellitus Down Syndrome Turner’s Syndrome Celiac Disease Klinefelter’s Syndrome Serum Free T4 and TSH are sufficient Serum T3 levels often misleading If measuring total T4 also do T3 resin uptake or thyroid binding protein Antithyroglobulin and antithyroid peroxidase antibodies Thyroid imaging rarely indicated NHANES III (1988 – 1994) Adolescents 12-19 years of age 6.3% positive antithyroglobulin 4.8% positive antithyroid peroxidase antibodies 2:1 Female:Male 105 children with positive antibodies and normal TSH followed for 5 years: 65% remained euthyroid 10% developed mild TSH elevation 26% developed TSH twofold above normal 55 children with positive antibodies and mildly elevated TSH levels: 29% reverted to normal TSH 29% were unchanged 42% developed TSH twofold above normal 1:3000 to 1:4000 in newborn infants More common in Hispanic and Native American infants at 1:2000 Less common in African American infants at 1:32,000 Consistently 2:1 Female:Male 85% are sporadic – 15% hereditary 90% permanent – 10% transient Only 5% suspected by clinical diagnosis ◦ At time of newborn screen ◦ At 2-3 weeks of age Birth weight and length normal OFC slightly increased Gestational age > 42 weeks in 33% Primary T4 measurement with backup TSH Primary TSH measurement Recall rate (T4 <10%, TSH > 20 mU/L ◦ Primary T4 - 0.3% ◦ Primary TSH – 0.05% Free T4 – Upper half of normal range: ◦ 1.4 – 2.3 ng/dl TSH < 10 mU/L ◦ May take one month of treatment Before Newborn Screening: ◦ If diagnosed between birth and 3 months IQ = 89 ◦ If diagnosed between 3 and 6 months IQ = 71 ◦ If diagnosed after 6 months IQ = 54 1 year-old child with undiagnosed/untreated congenital hypothyroidism who was born before national screening programs for this condition. She was treated with replacement thyroid hormone, and 6 months later had a more normal facial appearance but significant developmental delays due to delay in diagnosis and treatment. New England Congenital Hypothyroidism Collaborative ◦ Verbal IQ ◦ Performance IQ ◦ Full Scale IQ At 6 years of age. 109 107 109 New England Congenital Hypothyrodism Collaborative ◦ Inadequate treatment in first 3 years IQ = 87 A small proportion may have: Language deficits Problems with visual-spatial integration Ataxia Gross and fine motor incoordination Muscle tone abnormalities Short attention span Strabismus 10% will have sensorineural deafness Baloch Z, Carayon P, Conte-Devolx B, et al. Laboratory medicine practice guidelines. Laboratory support for the diagnosis and monitoring of thyroid disease. Thyroid 2003; 13:3. Cassio A, Ricci G, Baronio F, et al. Long-term clinical significance of thyroid autoimmunity in children with celiac disease. J Pediatr 2010; 156:292. Chiesa A, Gruñeiro de Papendieck L, Keselman A, et al. Final height in longterm primary hypothyroid children. J Pediatr Endocrinol Metab 1998; 11:51. Chiovato L, Larizza D, Bendinelli G, et al. Autoimmune hypothyroidism and hyperthyroidism in patients with Turner’s syndrome. Eur J Endocrinol 1996; 134-568. de Vries S, Bulvik S, Phillip M. Chronic autoimmune thyroiditis in children and adolescents: at presentation and during long-term follow-up. Arch Dis Child 2009; 94:33 Elmlinger MW, Kühnel W, Lambrecht HG, Ranke MB. Reference intervals from birth to adulthood for serum thyroxine (T4 ), triiodothyronine (T3), free T3, free T4, thyroxine binding globulin (TBG) and thyrotropin (TSH). Clin Chem Lab Med 2001: 39;973. Hollowell JG, Staehling NW, Flanders WD, et al. Serum TSH, T(4), and thyroid antibodies in the United States population (1988 to 1994): National Health and Nutrition Examination Survey (NHANES III). J Clin Endocrinol Metab 2002; 87:489. Lazar L, Frumkin RB, Battat E, et al. Natural history of thyroid function tests over 5 years in a large pediatric cohort. J Clin Endocrinol Metab 2009; 94:1678. Lindsay AN, Voorhess ML, MacGillivray MH. Multicystic ovaries detected by sonography in children with hypothyroidism. AJDC 1980; 134:588. Lindsay AN, Voorhess ML, MacGillivray MH. Multicystic ovaries in primary hypothyroidism. Obstetrics & Gynecology 1983; 61:433. Lindsay AN, Voorhess ML. Slipped capital femoral epiphysis in hypothyroidism. AJDC 1984; 138:1149. Moore DC. Natural course of ‘subclinical; hypothyroidism in childhood and adolescence. Arch Pediatr Adolesc Med 1996; 150:293. Nelson JC, Clark SJ, Borut DL, et al. Age-related changes in serum free thyroxine during childhood and adolescence. J Pediatr 1993; 123:899. Ozer G, Yüksel B, Kozanoġlu M, et al. Growth and development of 290 hypothyroidic patients at diagnosis. Acta Paediatr Jpn 1995; 37:145. Radetti ML, Gottardi E, Bona G, et al. The natural history of euthyroid Hashimoto’s thyroiditis in children. J Pediatr 2006; 149:827. Rallison ML, Dobyns BM, Meikle AW, et al. Natural history of thyroid abnormalities: prevalence, incidence and regression of thyroid diseases in adolescents and young adults. Am J Med 1991; 91:363. Rivkees SA, Bode HH, Crawford JD. Long-term growth in juvenile acquired hypothyroidism: the failure to achieve normal adult stature. N Engl J Med 1988; 318:599. Sattar N, Lazare F, Kacer M, et al. Celiac disease in children, adolescents, and young adults with autoimmune thyroid disease. J Pediatr 2011; 158:272. Sklar CA, Qazi R, David R. Juvenile autoimmune thyroiditis. Hormonal status at presentation and after long-term follow-up. Am J Dis Child 1986; 140:877.