Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
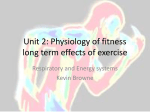
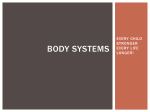
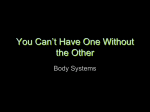
1 Clinical Science (1985)68,l-10 I EDITORIAL REVIEW I The respiratory muscles MALCOLM GREEN A N D J O H N MOXHAM Brompron and King’s College Hospitals, London Introduction Structure The respiratory muscles provide the motive power for breathing. Despite this central role in ventilation their physiology has been relatively neglected, perhaps partly because of the complexity of their function, and the difficulties of studying them. However, in the last decade, there has been considerable increase in interest, and a number of new concepts have arisen [l-31. It is now appreciated that the translation of central nervous output into ventilation requires a sophisticated integration of the respiratory muscles, which have to subserve the requirements of posture and body movement, simultaneously with breathing. The importance of the shape (configuration) of the respiratory system to muscle action has been emphasized. Analysis has shown that the functions of the diaphragm are complex: it is anatomically and embryologically derived from two muscles, and these parts may have different physiological actions. The abdominal muscles appear to be not only powerful muscles of expiration, but also facilitate inspiration. Both internal and external intercostal muscles now seem to be inspiratory at low lung volumes and expiratory at high lung volumes. Like all skeletal muscles the respiratory muscles are capable of fatigue after heavy loads. It is increasingly believed that respiratory muscle fatigue may play an important part in the pathogenesis of respiratory failure, and part of the value of artificial ventilation may lie in resting the respiratory muscles. The respiratory muscles comprise the diaphragm, the intercostal muscles, the abdominal muscles, and the so-called ‘accessory’ muscles including the sternomastoid and scalene muscles. However, probably all of the muscles of the trunk and neck can be recruited as respiratory muscles under heavy loads. The respiratory muscles are all skeletal (‘voluntary’) muscles, consisting of motor units innervated by a-motor neurones derived from anterior horn cells in the spinal column down to L.2. The accessory, intercostal and abdominal muscles are well supplied with muscle spindles, tendon organs and Paccinian corpuscles, providing an anatomical basis for sensory input from these muscles [l]. The diaphragm contains relatively fewer sensory endorgans, and there appear to be more tendon organs than muscle spindles [4]. There are, however, afferent fibres in the phrenic nerve of the cat, and afferent traffic has been recorded. The paucity of end-organs may reflect the tendency of the diaphragm to contract uniformly so that relatively few organs are necessary to sample accurately its functions [5].The main purpose of the diaphragm is to generate pressure differences, and the relatively greater number of tendon organs may reflect this, since tendon organs can sensitively reflect physiological contraction of muscle fibres Correspondence: Dr Malcolm Green, Brompton Hospital, Fulham Road, London SW3 6HP. PI. The respiratory muscles contain a mixture of type 1 (slow twitch, oxygen dependent, fatigue resistant fibres) and type 2 (fast twitch fibres, most of which fatigue quickly, using glycolytic energy stores) in approximately the same proportion as limb skeletal muscles. In man the diaphragm contains about 55% of type 1 and 45% of type 2 fibres, although the number of studies is small and there appears to be variability between subjects [6]. The physiological attributes and size of fibres can be altered by suitable training and detraining programmes in animals [7]. Physiology The respiratory muscles including the diaphragm appear to have physiological properties similar to the other skeletal muscles; they generate maximum force at resting length, and the force falls off as length diminishes: the length-tension relation- 2 M. Green and J. Moxharn ship. The diaphragm shows the same property studied both in vitro [8] and in vivo [9, lo]. It also tends to become less curved as it shortens, thus generating less pressure across it, by the Laplace relation [ l l ] . This is probably a small effect in normal subjects but may become significant in hyperinflation. The most important consequence is that lung volume influences the pressures the diaphragm can generate, being maximal when it is longest, and most curved, at low lung volumes. The force developed by skeletal muscles also falls off as the speed of shortening increases. It has been confirmed that the respiratory muscles also show this force-velocity relationship [12]. Thus as respiratory rate and depth increases the velocity of muscle shortening increases, and force generated for a given neural output falls. The respiratory muscles have similar time courses of pressure development [13, 141 and of relaxation [ 151 as do limb muscles. The diaphragm Anatomically the diaphragm consists of two main parts, inserted into the central tendinous dome. The larger (costal) part originates over the inner surfaces of the six lowest ribs and cartilages. These fibres initially run directly upwards, parallel and ‘apposed’ to the inner surface of the rib cage. This ‘area of apposition’ represents up to onethird of the surface area of the rib cage at end expiration, but diminishes during inspiration [ 161. Both the origins and insertions of these costal fibres are mobile, and potentially move with respiration. By contrast the lumbar (crural) portion has its origins on the second to fourth lumbar vertebrae and associated ligaments, which do not move with respiration. Contraction of the diaphragm has several effects [2, 16-19] (Fig. 1). (1) The central dome of the diaphragm descends with little change in its shape, peeling the muscular fibres from the inner surface of the rib cage along the area of apposition [lo]. This tends to cause a fall in pleural pressure and an increase in lung volume (inspiration). (2) Contraction of the diaphragm causes an increase in abdominal pressure. In the absence of abdominal muscle contraction this causes the anterior abdominal wall to move outwards. There is also outward pressure exerted on the lower rib cage through the area of apposition. This force is inspiratory in direction and has been called the ‘appositional component’ [20]. (3) The costal fibres of the diaphragm tend to lift the lower rib cage (insertional force). Because force m i a p Appositional p o s i t Area i o of n FIG. 1. Diagram to illustrate the actions of the diaphragm. On contraction the dome descends and abdominal pressure (Pab) rises. This expands the lower rib cage via an ‘appositional force’ and simultaneously the costal diaphragm elevates the lower rib cage (‘insertional force’) with a resultant force R. These actions cause a fall in pleural pressure (Ppl), inspiration, and a tendency to indrawing of the upper rib cage. of the shape and articulations of the ribs, upward movement also tends to cause forwards (pump handle) and outward (bucket handle) motion, particularly at low lung volumes. Since these fibres of the diaphragm are mobile at both ends a fulcrum is necessary to prevent mere descent of the dome [(l) above]. This is provided by the abdominal contents and anterior abdominal wall. Removing the abdominal viscera in horses, dogs and rabbits changes the result of costal diaphragm contraction from expanding the lower rib cage to contractingit [17, 18,211. When the diaphragm acts in isolation it also tends to have some expiratory components. Patients with transection of the lower cervical cord but intact phrenic nerve and diaphragm function show paradoxical motion inwards of the upper rib cage during inspiration [22,23]. This may also be seen during spinal anaesthesia [24] and diaphragm pacing [25]. Different physiological functions of the two parts of the diaphragm were proposed by Keith in 1904 [26] and subsequently by Briscoe in 1920 [27] but these suggestions have been ignored until recently. It has now been shown that the costal part of the diaphragm is active whilst the crural part is silent during vomiting, as might be expected [281. De Troyer and colleagues have demonstrated in dogs that both parts of the diaphragm cause an increase in abdominal pressure and a fall in pleural pressure..However, only the costal part has a direct The respiratory muscles inspiratory action on the rib cage by lifting the lower ribs [l8, 291. There has been considerable debate as to the relative contribution of the direct effects of the diaphragm on the rib cage, and its indirect effects via the abdominal and pleural pressure [30-321. Goldman & Mead [33] argued that the diaphragm expanded the rib cage along its relaxed pressure-volume characteristic. It now appears, however, that the rib cage deforms when intercostal activity is absent and that the pressures applied are complex, depending at least in part on the relative contributions of the two parts of the diaphragm [34]. Intercostal muscles The importance of the intercostal muscles in stabilizing the rib cage and preventing paradoxical motion of its parts has been mentioned above, Even in quiet breathing in normal subjects they appear to play a necessary role in ensuring coordinated movement of the whole of the rib cage WI. The parasternal intercostals elevate the ribs, but tend to lower the sternum [35], and are active during inspiration even in quiet breathing [36-381. The external intercostal muscles run from the lower surface of each rib anteriorly and inferiorly to the upper surface of the rib below. The internal intercostals by contrast run inferiorly and posteriorly. On the basis of this anatomical arrangement Hamberger concluded in 1727 [39] that the external intercostal muscles were inspiratory since by their contraction each lower rib was pulled upwards and backwards towards the rib above it, thereby swinging outwards. Conversely the internal intercostal muscles pulled each upper rib posteriorly, downwards, and inwards, to cause expiration. Electromyographic studies have shown that the external intercostals are active during inspiration and internal intercostals during expiration [36, 371. However, recently doubt has been cast on Hamberger’s hypothesis by the studies of De Troyer and colleagues who have: shown in dogs that the action of the intercostal muscles depends on lung volume [40]. At low lung volumes both external and internal intercostal muscles are inspiratory when they contract, and at high lung volumes both groups are expiratory, Since the uppermost and lowermost ribs are mobile, there must be stabilization of the rib cage for effective action by the intercostal muscles. The scalene and sternomastoid muscles stabilize the upper rib cage during inspiration, and the abdominal muscles help fnate the lower rib cage during expiration [35,41]. 3 Abdominal muscles Contraction of these powerful muscles tends to pull the rib cage inwards and downwards and to push the abdominal contents upwards, elevating the diaphragm. Both these actions cause expiration and these muscles have generally been viewed as purely expiratory [42]. However, their actions now appear to have additional complexities [20, 431. Thus contraction of the abdominal muscles increases abdominal pressure. This, as seen above (Fig. l), tends to expand the lower rib cage through the area of apposition, an inspiratory motion. Furthermore upward motion of the dome of the diaphragm tends to stretch its costal fibres, and thus to lift the lower rib cage, which is also in an inspiratory direction. Theoretically, the net effect of contraction of abdominal muscles would depend on the relative importance of these factors, and studies in dogs have shown a significant inspiratory tendency, particularly of the external oblique muscles [43]. The abdominal muscles also ensure that the diaphragm returns to its resting length at endexpiration, so that it is best placed on its lengthtension characteristic for subsequent contraction during inspiration [lo, 22, 441. The maintenance of abdominal pressure by abdominal muscle contraction during inspiration serves as a fulcrum for the costal diaphragm to elevate the lower ribs, so that the abdominal muscles can be considered as ‘accessory muscles of inspiration’ [20]. The abdominal muscles are electrically silent during quiet breathing when supine, but when erect there is tonic activity which is greatest in the lower abdomen [45]. This has been conceived as entirely postural [37, 461. However, active contraction of the abdominal muscles during both inspiration and expiration may play a role in both phases of breathing, suggesting that this activity may be partly ventilatory. Accessory muscles The most important of these are the scalene muscles and the sternomastoids. Studies of the scalenes using needle electrodes show that they have inspiratory electrical activity even during quiet breathing, so that they should probably be viewed as muscles of normal inspiration rather than ‘accessory muscles’ [41], acting to elevate, or to prevent downward displacement of, the upper rib cage during inspiration [351. These muscles have increased activity during stimulated ventilation, in patients with lesions of the upper cervical cord and in chronic airways obstruction [23,47]. 4 M. Green and J. Moxham Configuration and lung volume During inspiration the mechanical difficulty of producing a negative pressure pump using only contractile elements has been overcome by the complex geometry and interactions of the respiratory muscles. The shape of the system has been termed its configuration, and this importantly determines the efficiency of ventilation. Configuration is closely, but not uniquely, related to lung volume. As lung volume increases the respiratory muscles become less advantageously placed for inspiration and more advantageously placed for expiration. In normal subjects this appears to be an important mechanism for maximizing the efficient use of the muscles. However, it can have disadvantages in disease: airways obstruction leads to hyperinflation, putting the inspiratory muscles at a less advantageous configuration. By contrast fibrotic lung diseases, causing a reduction of lung size, tend to put the inspiratory muscles at a more advantageous configuration so that they are better placed to overcome the increased mechanical load provided by the stiff lungs [48]. Modelling the respiratory muscles A number of attempts have been made to model the function of the respiratory muscles using mechanical, electrical or pneumatic analogies [34]. A mechanical model, modified from these by permission, is shown in Fig. 2. Sterno-mastoids Intercost muscles Rib cage Abdominal muscles - FIG. 2. Diagram to illustrate some of the respiratory muscle actions. This model shows the effect of the two muscular parts of the diaphragm in causing descent of the dome. The costal diaphragm in addition elevates the rib cage. The role of the intercostal muscles is not easily depicted: they cause elevation or descent of the rib cage, depending partly on its initial position. The abdominal contents are shown as a hydraulic system containing compressible fluid. Rise in abdominal pressure (Pab) tends to stabilize the diaphragm and expand the lower rib cage. The abdominal muscles by relaxing can facilitate descent of the diaphragm, and by contracting cause elevation of the dome of the diaphragm. The scalenes and sternomastoids fixate, or tend to elevate, the upper rib cage. Respiratory muscle fatigue Patients with severe lung disease and hyperinflation have reduced force generating capacity of the respiratory muscles. In contrast their ventilatory requirements are increased. The muscles, particularly the inspiratory muscles, are subject to large loads with every breath for prolonged periods and with little opportunity for rest. Patients with severe chronic airways obstruction have a high neural output to the respiratory muscles [49] comparable with that required to sustain near maximum ventilation in normal subjects. This combination of high drive and large loads for long periods has led to the suggestion, by analogy with limb muscles, that fatigue could develop in the respiratory muscles and contribute to hypercapnic ventilatory failure [50]. Muscle fatigue can usefully be defined as the inability to sustain the required force with continued contractions. This is a characteristic of limb muscles and recent studies have demonstrated that the respiratory muscies can also fatigue. Normal subjects can sustain large respiratory loads for only short periods. Thus the diaphragm cannot maintain greater than 40% of its maximum pressure with each breath indefinitely [Sl]. The overall respiratory pressures that can be sustained indefinitely are further reduced (i) by high lung volumes when the muscles are shortened, (ii) as mean inspiratory flow rates increase when there is increased velocity of shortening, (iii) as breathing frequency increases, (iv) as the proportion of the time devoted to inspiration during each breath rises with longer contraction of the inspiratory muscles [52,53]. In spite of much research over recent years, the precise cause of skeletal muscle fatigue is not clear; indeed it is unlikely that a single cause is responsible and it is probable that under different circumstances a variety of factors can become relevant. Reduced central neural drive, especially The respiratoly muscles during sustained maximum voluntary effort, may be important [54]. However, for many contractions including the repetitive submaximal ones of ventilation, an important aspect of fatigue is likely to be reduced muscle contractility [55]. As fatiguing exercise continues and contractility falls, so central firing frequency increases to counteract force loss, but eventually central frequency itself falls despite the reduction in muscle tension. This fall in firing frequency may represent an adaptation to peripheral fatigue that avoids excessive ATP depletion and the onset of rigor. The situation may be rather different when a muscle is acutely subjected to an overwhelming load. In this case there is likely to be a rapid fall in local chemical energy supplies and a failure of muscle excitation, an energy consuming process, thereby causing a ‘catastrophic’ loss of force but no further energy consumption [56]. During respiratory failure both these patterns of fatigue may operate. In patients with longstanding respiratory disease, due to chronic airways obstruction or scoliosis, the central nervous system may modify respiration in response to muscle fatigue by changing the respiratory rate, inspiratory time and mean inspiratory flow, thereby avoiding critical depletion of chemical energy stores but only at the expense of allowing hypoventilation and hypercapnia. By contrast in severe acute disease, as in life-threatening asthma, the overwhelming load on the respiratory muscles may precipitate catastrophic force loss and acute ventilatory failure. Detection of fatigue Detection of fatigue in the respiratory muscles is difficult because there is no simple technique for measuring their force generation. Therefore, less direct techniques have been employed. Muscle fatigue has been investigated by measuring the frequency spectrum of the electromyogram (EMG) [57]. When skeletal muscle generates a tension that cannot be sustained there is an early alteration in the EMG with reduction in high frequency and increase in low frequency activity, resulting in reduction in the EMG ‘high/low’ ratio. This has been used as a marker of muscle fatigue and has been applied to the muscles of respiration, particularly the diaphragm [58]. However, the cause of the shift in the power spectrum is not known, nor is the relation of the EMG change to force loss understood; for example, after diaphragm and quadriceps fatigue the high/ low ratio returns to normal at a time when force generation is still abnormal [59]. 5 With fatigue the speed of muscle characteristically slows. Recent work on the respiratory muscles has examined the relaxation of the human diaphragm measured from transdiaphragmatic pressure during a maximal sniff. In normal subjects the relaxation rate for the non-fatigued diaphragm is similar to that of limb muscles and after prolonged inspiratory loading relaxation is slowed [ 151. The investigation of respiratory muscle relaxation rates may be possible in patients and allow identification of fatigue clinically. Some of the techniques used to study limb muscle fatigue can also be applied to the respiratory muscles. Studies in resting hand and leg muscles of the force produced by electrical stimulation show a characteristic relationship of stimulation frequency to force, described by the frequency-force curve [60]. With fatigue the shape of the curve is altered with a reduction in the forces generated at high stimulation frequencies (‘high frequency fatigue’) [61] and/or reduction in the forces at low stimulation frequencies, less than 30 Hz (‘low frequency fatigue’) [62]. In high frequency fatigue there is defective muscular excitation due either to neuromuscular junction failure or to impaired depolarization of the muscle cell membrane. This excitatory failure is associated with a reduced EMG and is rapidly restored to normal by rest. In low frequency fatigue excitation of the muscle cell membrane is normal and the EMG is not diminished, but the force per membrane action potential is reduced implying impaired contractility of the muscle fibre itself. This type of fatigue can be long lasting, sometimes persisting for many hours. After prolonged muscular activity, force generation at low frequencies may also be reduced by changes in tendons which become more extensible [63]. Furthermore muscle shortening due to hyperinflation reduces forces at low frequencies to a greater extent than at high frequencies [64]. Thus, a number of factors can shift the frequencyforce curve to the right and may be of particular physiological importance because the firing frequency of motor neurones during everyday activities is low (5-30 Hz) [65]. Even during a maximum voluntary contraction the motor neurone firing frequency falls to below 30Hz within a few seconds [66]. Electrical stimulation has been used to investigate the contractile properties of the respiratory muscles and to detect fatigue. Crucially the frequency-force curve of the sternomastoid and the frequency-transdiaphragmatic pressure curve of the diaphragm have the same shape as the curves of other skeletal muscles [67, 681. In normal subjects, inspiratory loading and sustained M. Green and J. Moxharn 6 maximum voluntary ventilation produces low frequency fatigue both in the sternomastoid and also in the diaphragm (Fig. 3). Furthermore, patients with chronic airways obstruction who voluntarily breathe maximally develop low frequency fatigue of the sternomastoid [69]. To date it has not been possible to evaluate low frequency fatigue of the diaphragm in these patients. Although it is likely that low frequency fatigue of the respiratory muscles is of clinical importance, the detection of such fatigue in patients with respiratory failure presents great difficulties. During very brief maximum voluntary efforts lasting less than 2 or 3 s motor neurone firing frequencies are high so that force generation is little affected by low frequency fatigue, probably due to saturation of the interior of muscle fibres with calcium ions [70]. Thus maximum respiratory pressures, peak expiratory flow rates and forced vital capacity are not reduced [71]. Resting ventilation is associated with lower neural firing frequencies. Experimental data for the cat suggest that during tidal breathing phrenic motor neurone firing frequency is 10-15 Hz rising to 20-30 Hz with COz stimulation [72]. Low frequency fatigue might therefore cause an important fall in respira- tory muscle force production not revealed by tests of maximum effort. Consistent with this suggestion is the observation that respiratory muscle fatigue may cause a reduction in the ventilatory response to carbon dioxide of normal subjects [71]. In limb muscles, fatigue is most likely to develop when contractions are each a large proportion of maximum force. During high force contractions many limb muscles become ischaemic [73] and metabolism is therefore anaerobic. However, the blood supply of the diaphragm is excellent and continues to rise with hyperventilation [74]. Despite this there could be poor oxygen delivery at a cellular level, particularly when the respiratory muscles contract throughout the respiratory cycle, as may be the case in severe asthma. The importance of oxygen delivery appears to be -supported by the observation that during loaded breathing the endurance of the inspiratory muscles of normal subjects is decreased by hypoxia [51]. However, the mechanism of this effect is not clear and could be mediated via the central nervous system or through a direct action on peripheral muscle. Therapy 0 20 40 60 80 100 Stimulation frequency (Hz) FIG. 3. Frequency-pressure curves of the diaphragm. The phrenic nerve of a normal subject was stimulated in the neck at increasing frequencies (abscissa) and the resultant transdiaphragmatic pressure (A) was measured with oesophageal and gastric balloons and expressed as a percentage of the maximum Pdi (ordinate). The subject then fatigued his diaphragm by breathing through an inspiratory resistance to exhaustion. After fatigue (A) there was a characteristic shift of the curve to the right. Treatment of patients with respiratory disease should take account of factors that can affect respiratory muscle function. Adequate nutrition is important to maintain muscle mass since wasting causes weakness and predisposes to fatigue. In wasting diseases the respiratory muscles atrophy and pressure generation is impaired [75]. High dose steroids commonly used in chest medicine and known to cause skeletal muscle wasting could produce respiratory muscle weakness in addition to hypokalaemia. It is possible to increase the strength and endurance of muscle by appropriate training. It is not known whether training renders muscle less susceptible to low frequency fatigue, but training for strength may raise the threshold for fatigue and endurance training increases capillaries, mitochondria and oxidative enzymes. Maximum respiratory pressures can be increased in normal subjects by training [76] and specific training of the respiratory muscles can improve ventilatory performance of patients with cystic fibrosis, quadriplegia and chronic airways obstruction [77-791. However, respiratory muscle training is difficult, the increases in strength may be only small [80] and whether such training schedules produce long term benefit remains uncertain. Therapy directed at the underlying respiratory disorder may reduce the load on the respiratory The respiratoory muscles muscles to a level that will not precipitate or perpetuate fatigue. Delivery of oxygen to the working muscle can be optimized by attention to arterial 'oxygen tensions, haemoglobin levels and cardiac output. Metabolic acidosis should be corrected as well as other metabolic disturbances known to cause muscle weakness such as hypophosphataemia, hypokalaemia and disorders of calcium metabolism. Therapy that reduces overinflation may be particularly helpful by improving chest wall geometry, length-tension characteristics and restoring diaphragm curvature. Both low frequency fatigue and muscle shortening can be offset by an increase in motor neurone firing frequency; thus respiratory stimulants may have a short term therapeutic role. Conversely drugs causing depression of the respiratory centre may substantially impair ventilation. Drugs that increase muscle twitch tension would be particularly helpful, shifting the frequency-force curve to the left and improving force generation at physiological firing frequencies (Fig. 3). Furthermore, such a shift would diminish the effect of low frequency fatigue and muscle shortening. Xanthine-related drugs can improve the contractile performance of skeletal muscle studied in vitro [81] and aminophylline has been reported to improve the force-generating properties of the diaphragm in man [82]. However, studies in vivo of the effect of aminophylline on the adductor pollicis muscle of the hand show that twitch-tension, the frequency-force curve and low frequency fatigue are not affected by this drug at therapeutic concentrations [83]. Similarly the transdiaphragmatic twitch pressure from stimulation of the phrenic nerve of normal subjects is not affected by intravenous aminophylline [84]. Thus, while the usefulness of aminophylline in respiratory disease is not in doubt, a direct beneficial action on respiratory muscle contractility remains unproven. 0-Receptor agonists such as terbutaline and salbutamol may enhance respiratory muscle contractility [85]. The effect of terbutaline appears to be greater on fatigued than fresh muscle. This may be due to the slowing of muscle contraction and relaxation with fatigue since terbutaline has a greater potentiating effect on slow twitch than on fast twitch fibres. In patients with progressive respiratory failure, assisted ventilation may become necessary. If fatigue is present, one benefit may be the total resting of the respiratory muscles for sufficient time for fatigue to resolve. It is also conceivable that carefully selected patients can be helped by patient-triggered positive pressure ventilators to assist inspiration and reduce the workload of the respiratory muscles, protect against fatigue and 7 thereby avoid the necessity of intubation and mandatory ventilation. In patients with neuromuscular weakness, intermittent support by tank and cuirass ventilation can be beneficial. Scoliosis patients and those who have had thoracoplasties in the past can be similarly helped by intermittent assisted ventilation [86]. The mechanism whereby such patients derive benefit is not certain but resting the respiratory muscles may be an important factor serving to avoid or reverse fatigue. If this is so, efforts to rest the respiratory muscles intermittently by using techniques that do not require intubation may deserve careful reappraisal in patients with severe chronic airways obstruction. The clinical importance of respiratory muscle fatigue is not yet clear and further progress must depend on developing suitable techniques for its detection. Only then will the relative contributions of, for example, inadequate respiratory centre output or reduced muscle contractility become apparent. The many stages from central nervous system output via respiratory muscle force generation to the production of appropriate ventilation are of bewildering complexity. The process is one of integration, both when functioning normally and during ventilatory failure. Biological feedback serves to modify overall function in response to failure at any given level. Thus, in most cases of respiratory failure to identify any single step as the crucial weak link may be neither sensible nor possible. References 1. Campbell, E. J.M., Agostoni, E. & Newsom Davis, J. (1970) The Respirarory Muscles: Mechanics and Neural Conrrol, 2nd edn. Lloyd-Luke, London. 2. Derenne, J.P., Macklem, P.T. & Roussos, C. (1978) The respiratory muscles: mechanics, control and pathophysiology. State of the art. American Review of Respirarory Disease, 188, 119-133, 373-390, 581-601. 3. Green, M. & Moxham, J. (1983) The Respirarory Muscles. Recenr Advances in Respirarory Medicine, vol. 111, pp. 1-20. Ed. Flenley, D.C. & Petty, T.L. Churchill Livingstone, Edinburgh. 4. Corda, M., von Euler, C. & Lennerstrand, G. (1965) Proprioceptive innervation of the diaphragm. Journal ofPhysiology (London), 178,161-177. 5 . Green, M., Mead, J. & Sears, T.A. (1978) Muscle activity during chest wall restriction and positive pressure breathing in man. Respiration Physiology, 35,283-300. 6. Lieberman, D.A., Faulkner, J.A., Craig, A.B. & Maxwell, L.C. (1973) Performance and histochemical composition of guinea pig and human diaphragm. Journal o f Applied Physiology, 34,233-231. 7. Faulkner, J.A., Maxwell, L.C., Ruff, G.L. & White, T.P. (1979) The diaphragm as muscle. Contractile properties. American Review o f Respirarory Disease, 119 (Suppl. 2), 89-92. 8 M. Green and J. Moxham 8. Kim, M. J., Druz, W.S., Danon, J., Machnach, W. & Sharp, J.T. (1976) Mechanics of the canine diaphragm. Journal of Applied Physiology, 41,369-382. 9. Grassino, A., Goldman, M.D., Mead, J. & Sears, T.A. (1978) Mechanics of the human diaphragm during voluntary statics. Journal o f Applied Physiology, 44,829-839. 10. Braun, N.M.T. (1982) Force-length relation of the normal human diaphragm. Journal of Applied Physiology: Respiratory, Environmental and Exercise Physiology, 53,405-412. 11. Marshall, R. (1962) Relationship between stimulus and work of breathing at different lung volumes. Journal of Applied Physiology, 17,817-921. 12. Goldman, M.D., Grassino, A,, Mead, J. & Sears, T.A. (1978) Mechanics of the human diaphragm during voluntary contraction: dynamics. Journal of Applied Physiology: Respiratory, Environmental and Exercise Physiology, 44,840-848. 13. Mognoni, P., Saibene, F., Sant’Ambrogio, G. & Agostoni, E. (1968) Dynamics of the maximal contraction of the respiratory muscles. Respiration Physiology, 4, 193-202. 14. Miller, J.M. & Green, M. (1984) Time course of development of transdiaphragmatic pressure in man. Clinical Science, 66,41P. 15. Esau, S.A., Bye, P.T.B. & Pardy, R.L. (1983) Changes in rate of relaxation of sniffs with diaphragmatic fatigue in humans. Journal of Applied Physiology: Respiratory, Environmental and Exercise Physiology, 55, 731-735. 16. Mead, J. (1979) Functional significance of the area of apposition of diaphragm to rib cage. American Review ofRespirarory Disease, 119 (2), 31-32. 17. Duchenne, G.B. (1867) Physiology o f Motion (translated by Kaplan, E.B.). Saunders, Philadelphia. 18. De Troyer, A., Sampson, M., Sigrist, S. & Macklem, P.T. (1982) Action of the costal and crural parts of the diaphragm on the rib cage in dog. Journal o f Applied Physiology: Respiratory, Environmental and Exercise Physiology, 53, 30-39. 19. Mead, J . & Loring, S.H. (1982) Analysis of volume displacement and length changes of the diaphragm during breathing. Journal o f Applied Physiology: Respiratory, Environmental and Exercise Physiology, 53,750-755. 20. De Troyer, A. (1983) Mechanical action of the abdominal muscles. Clinical Respiratory Physiology, 19, 575-581. 21. D’Angelo, E. & Sant’Ambrogio, G. (1974) Direct action of contracting diaphragm on the rib cage in rabbits and dogs. Journal of Applied Physiology, 36, 7 15-7 19. 22. Mortola, J.P. & Sant’Ambrogio, G. (1978) Motion of the rib cage and abdomen in tetraplegic patients. Clinical Science and Molecular Medicine, 54, 25-32. 23. Danon, J., Druz, W.S., Goldberg, N.B. & Sharp, J.T. (1979) Function of the isolated paced diaphragm and the cervical accessory muscles in CI quadriplegics. American Review o f Respiratory Disease, 119, 909919. 24. Eisele, J., Trenchard, D., Burki, N. & Guz, A. (1968) The effect of chest wall block on respiratory sensation and control in man. Clinical Science, 35, 23-33. 25. Glenn, W.L., Hogan, J.F. & Phelps, M.L. (1980) Ventilatory support of the quadriplegic patient with respiratory paralysis by diaphragm pacing. Surgical Clinics of North America, 60, 1055-1078. 26. Keith, A. (1904) The nature of the mammalian diaphragm and pleural cavities. Journal of Anatomy and Physiology, 39,243-284. 27. Briscoe, G. (1920) The muscular mechanism of the diaphragm. Journal of Physiology (London), 54, 46-53. 28. Monges, H., Salducci, J. & Naudy, B. (1978) Dissociation between the electrical activity of the diaphragmatic dome and crura muscular fibres during oesophageal distension, vomiting and eructation. An electromyographic study in the dog. Journal de Physiologic (Paris), 74,541-554. 29. De Troyer, A., Sampson, M., Sigrist, S. & Macklem, P.T. (1981) The diaDhramn: - - two muscles. Science. 213,237-238. 30. Macklem. P.T.. Gross. D.. Grassino, A. & Roussos, C. (1978) Partitioning of the inspiratory pressure swings between diaphragm and intercostal/accessory muscles. Journal of Applied Physiology, 44, 200-208. 3 1. Goldman, M. (1979) Mechanical interaction between diaphragm and rib cage. Boston view. American Review of Respiratory Disease, 119 (2), 23-26. 32. Macklem, P.T. (1979) Ribcage-diiaphragm interaction: Montreal view. American Review of ResDiratow Disease, 119 (2), 27-29. 33. Goldman. M.D. & Mead. J. (1973) Mechanical interaction between the diaph;agm and rib cage. Journal of Applied Physiology, 35, 197-204. 34. Macklem, P.T., Macklem, D.M. & De Troyer, A. (1983) A model of inspiratory muscles mechanics. Journal of Applied Physiology: Respiratory, Environmental and Exercise Physiology, 55,547-557. 35. De Troyer, A. & Kelly, S. (1982) Chest wall mechanics in dogs with acute diaphragm paralysis. Journal of Applied Physiology: Respiratory, Environmental and Exercise Physiology, 53, 373-379. 36. Taylor, A. (1960) The contribution of the intercostal muscles to the effort of respiration in man. Journal of Physiology (London), 15 1, 390-402. 37. Delhez, L. (1974) Contribution Electromyographique d I’Etude de la Mecanique et du Controle Nerveux des Mouvements Respiratoires de I’Hornme. VaillantCarmanne, Liege. 38. De Troyer, A. & Sampson, M.G. (1982) Activation of the parasternal intercostals during breathing efforts in human subjects. Journal o f Applied Physiology: Respiratory, Environmental and Exercise Physiology, 52, 524-529. 39. Hamberger, G.E. (1749) De Respirationis Mechanismo. J.C. Croeker, Ienae. 40. De Troyer, A., Kelly, S. & Zin,W.A. (1983) Mechanical action of the intercostal muscles on the ribs. Science, 220, 87-89. 41. Raper, A.J., Thompson, W.T., Shapiro, W. & Patterson, J.L. (1966) Scalene and sternomastoid muscle function. Journal of Applied Physiology, 21, 497502. 42. Agostoni, E. & Campbell, E.J.M. (1970) The abdominal muscles. In: The Respiratory Muscles: Mechanics and Neural Control, pp. 175-180. Ed. Campbell, E.J., Agostoni, E. & Newsom-Davis, J. Lloyd-Luke, London. 43. De Troyer, A., Sampson, M., Sigrist, S. & Kelly, S. (1983) How the abdominal muscles act on the rib cage. Journal of Applied Physiology: Respiration, Environmental and Exercise Physiology, 54,465 -46 9. 44. Grimby, G., Goldman, M. & Mead, J. (1976) Respiratory muscles action inferred from rib cage and abdominal V-P partitioning. Journal of Applied Physiology, 41, 739-751. m e respiratoly muscles 45.Strohl, K.P., Mead, J., Banzett, R.B., Loring, S.H. & Kosch, P.C. (1981) Regional differences in abdominal muscle activity during various manoeuvres in humans. Journal o f Applied Physiology: Respiration, Environmental and Exercise Physiology, 51, 1471-1476. 46. Floyd, W.F. & Silver, P.H.S. (1950) Electromyographic study of patterns of activity of the anterior abdominal wall muscles in man. Journal o f Anatomy, 84, 132-145. 47.Campbell, E.J.M. (1970) Accessory muscles. In: The Respiratory Muscles: Mechanics and Neural Control, pp. 181-193. Ed. Campbell, E.J., Agostoni, E. & Newsom-Davis, J. Lloyd-Luke, London. 48. Brennan, J., Morns, A.J.R. & Green, M. (1983) Thoracoabdominal mechanics during tidal breathing in normal subjects and in emphysema and fibrosing alveolitis. Kkorax, 38,62-66. 49. Gribbin, H.R., Gardiner, I.T., Heinz, C.J., Gibson, G.J. & Pride, N.B. (1983) The role of impaired inspiratory muscle function in limiting ventilatory response to CO, in chronic airflow obstruction. Clinical Science, 64,487-495. 50. Macklem, P.T. & Roussos, C.S. (1977) Respiratory muscle fatigue: a cause of respiratory failure. Clinical Science, 53,419-422. 51. Roussos, C.S. & Macklem, P.T. (1977)Diaphragmatic fatigue in man. Journal o f Applied Physiology, 43, 189-197. 52.Roussos, C.S., Fixley, M., Gross, D. & Macklem, P.T. (1979) Fatigue in inspiratory muscles and their synergistic behavior. Journal of Applied Physiology, 46,879-904. 53.Bellemare, F. & Grassino, A. (1982) Evaluation of human diaphragm fatigue. Journal o f AppZied Physiology: Respiratory, Environmental and Exercise Physiology, 53,1196-1206. 54. Bigland-Ritchie, B., Jones, D.A., Hosking, G.P. & Edwards, R.H.T. (1978) Central and peripheral fatigue in sustained maximum voluntary contractions of human quadriceps muscles. Clinical Science and Molecular Medicine, 54,609-614. 55. Merton, P.A. (1954) Voluntary strength and fatigue. Journal of Physiology (London), 123,553-564. 56. Edwards, R.H.T. (1983)Biochemicalbasis of fatigue in exercise performance: catastrophe theory of muscular fatigue. In: Proceedings o f the Fifth International Symposium on the Biochemistry o f Exercise. Ed. Knuttgen, H.G., Vogel, J.A. & Poortmans, J.C. Human Kinetics Publishers Inc, Illinois. 57. Lindstrom, L., Magnusson, R. & Petersen, I. (1974) Muscle load influence on myoelectric signal characteristics. Scandinavian Journal o f Rehabilitation Medicine (Suppl. 3), 127-148. 58.Gross, D., Grassino, A., Ross, W.R.D. & Macklem, P.T. (1979)Electromyogram pattern of diaphragmatic fatigue. Journal of Applied Physiology, 46, 1-7. 59. Moxham, J., Edwards, R.H.T., Aubier, A., De Troyer, A., Farkas, G., Macklem, P.T. & Roussos, C. (1982) Changes in the EMG power spectrum (high/low ratio) with force fatigue in man. Journal of Applied Physiology: Respiratory, Environmental and Exercise Physiology, 53,1094-1099. 60.Edwards, R.H.T., Young, A., Hoskmg, G.P. & Jones, D.A. (1977)Human skeletal muscle function: description of tests and normal values. Clinical Science, 52, 282-290. 61.Edwards, R.H.T. (1978) Physiological analysis of skeletal muscle weakness and fatigue. Clinical Science, 55, 1-8. 9 62.Edwards, R.H.T., Hill, D.K., Jones, D.A. & Merton, P.A. (1977) Fatigue of long duration in human skeletal muscles after exercise. Journal of Physiology (London), 272,769-778. 63.Vigreux, B., Chockaert, J.C. & Pertuzon, E. (1980) Effects of fatigue on the series elastic component of human muscle. European Journal of Applied Physiology, 45, 11-17. 64.Edwards, R.H.T. (1979) The diaphragm as a muscle. Mechanisms underlying fatigue. American Review of Respirarory Disease, 119, 81-84. 65.Grimby, G. & Hannerz, J. (1977) Firing rate and recruitment order of two extensor motor units in different modes of voluntary contractions. Journal ofPhysiology (London), 264,865-879. 66. Bigland-Ritchie, B., Jones, D.A. &Woods, J.J. (1979) Excitation frequency and muscle fatigue: electrical responses during human voluntary and stimulated contractions. Experimental Neurology, 64, 414- 427. 67.Moxham, J., Wiles, C.M., Newham, D. & Edwards, R.H.T. (1980) Sternomastoid muscle function and fatigue in man. Clinical Science, 59,463-468. 68.Moxham, J., Morris, A.J.R., Spiro, S.G., Edwards, R.H.T. & Green, M. (1981)Contractile properties and fatigue of the diaphragm in man. Thorax, 36, 164168. 69.Moxham, J., Wiles, C.M., Newham, D. & Edwards, R.H.T. (1981)Contractile function and fatigue of the respiratory muscles in man. In: Human Muscle Fatigue: Physiological Mechanisms, pp . 197-212. CIBA Foundation Symposium 82. Pitman Medical, London. 70.Jones, D.A. (1981) Muscle fatigue due to changes beyond the neuromuscular junction. In: Human Muscle Farigue: Physiological Mechanisms, pp. 178192. CIBA Foundation symposium 82. Pitman Medical, London. 71.Moxham, J., Wiles C.M., Newham, D., Spiro, S.G. & Edwards, R.H.T. (1982) Respiratory muscle fatigue reduces the ventilatory response to carbon dioxide. Clinical Science, 62,40. 72.Iscoe, S., Dankoff, J., Migicovsky, R. & Polosa, C. (1976) Recruitment and discharge frequency of phrenic motoneurones during inspiration. Respirarion Physiology, 26,113-128. 73.Barcroft, H. & Milen, J.L.E. (1939) The blood flow through muscle during sustained contraction. Journal ofPhysiology (London), 97, 17-31. 74. Rochester, D.F. & Briscoe, A.M. (1979)Metabolism of the working diaphragm. American Review of Respirarory Disease, 119 (Suppl. 2), 101-106. 75. Arora, N.S. & Rochester, D.F. (1982) Respiratory muscle strength and maximal voluntary ventilation in under-nourished patients. American Review o f Respiratory Disease, 126,5-8. 76. Leith, D. & Bradley, M. (1976) Ventilatory muscle strength and endurance training. Journal o f Applied Physiology, 41,508-516. 77. Keens, T.G., Kastins, I.R.B., Wannamaker, E.M., Levison, H., Crozier, D.N. & Bryan, A.C. (1977) Ventilatory muscle endurance training in normal subjects and patients with cystic fibrosis. American Review of Respiratory Disease, 116, 853-860. 78.Gross, D., Ladd, H.W., Riley, E.J., Macklem, P.T. & Grassino, M.D. (1980)Effect of training on strength and endurance of diaphragm in quadriplegia. American Journal o f Medicine, 68,27-34. 79.Belman, M.J. & Mittman, C. (1980) Ventilatory muscle training improves exercise capacity in chronic 10 M. Green and J. Moxham obstructive pulmonary disease patients. American Review of Respiratory Disease, 121, 273-280. 80., Miller, J.M., Alison, J., Moxham, J., Dhillon, P. & Green, M. (1983) Respiratory muscle strength training. Clinical Respiratory Physiology, 19, 65. 81..Jones, D.A., Howell, S., Roussos, C. & Edwards, R.H.T. (1982) Low frequency fatigue in isolated skeletal muscles and the effects of methyl xanthines. Clinical Science, 63, 161-167. 82. Aubier, M., De Troyer, A., Sampson, M., Macklem, P.T. & Roussos, C. (1981) Aminophylline improves diaphragmatic contractility. New England Journal of Medicine, 305, 249-252. 83 .Wiles, C.M., Moxham, J., Newham, D. & Edwards, R.H.T. (1983) Aminophylline and fatigue of adductor pollicis in man. Clinical Science, 64,547-550. 84. Moxham, J., Miller, J.M., Wiles, C.M., Newham, D., Edwards, R.H.T. & Green, M. (1983) The effect of aminophylline on human diaphragm and limb muscle contractility. Thorax, 38, 232. 85. Aubier, M., Viires, N., Medrano, G., Murciano, D., Lecocguic, Y. & Pariente, R. (1983) Effects and mechanism of action of terbutaline on diaphragm contractility and fatigue. American Review of Respiratory Disease, 127 (no. 4, Part 2), 231. 86. Sawicka, E.H., Branthwaite, M.A. & Spencer, G.T. (1983) Respiratory failure after thoracoplasty: treatment by intermittent negative-pressure ventilation. Thorax, 38,433-435.