Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
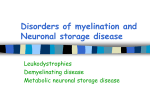
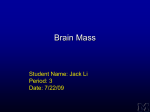
Case Study Steve Factor, M.D. PGY-4 Neurology Resident (2014-2015) Clinical History 26 year old female financial consultant with past medical history of migraines presents to Neurology Clinic with her boyfriend. He states that over the past few months she has become excessively impulsive and become prone to aggressive outbursts. In addition, he recently found out that she has had unprotected sex with three partners in as many weeks, but seems unconcerned with her new behavior and how it may affect him. She and her boyfriend deny any evidence of delusions, hallucinations. Mental Status Examination Mild deficits in the rate of information processing, attention, memory, cognitive flexibility, and problem solving. In conversation, she is mildly restless with improperly timed episodes of laughter, expansive affect, elevated mood and prone to sudden change of topic. A&Ox3, little insight or judgment into her actions. Neurologic Exam CN: 2-12 normal MOTOR: 5/5 strength in all extremities proximally and distally, normal bulk but slightly increased tone in bilateral lower extremities SENSORY: normal sensation in all modalities REFLEXES: 2+ in all extremities except 3+ bilateral patellas. No clonus, downgoing toes. CEREBELLAR: normal FTN, HTS bilaterally GAIT: mildly spastic gait with good casual arm swing Differential Diagnosis? Differential Diagnosis? Psychosis Bipolar Depression Schizophrenia Schizoaffective Disorder Excessive alcohol consumption Amphetamine/Cocaine use Expert Differential Diagnosis Anti-NMDA receptor encephalitis HIV dementia Huntington’s Disease Creutzfeld-Jakob Disease Multiple Sclerosis Porphyria Frontal Temporal Lobe Dementia Describe Imaging Findings T2 Flair T2 FLAIR T1 +C CT w/o contrast GRE T1 Imaging StudiesInterpretation Extensive symmetrical T2 hyperintensity in the periventricular white matter that extends to the subcallosal white matter with sparing of the subcortical U-fibers. Frontal, temporal, and parietal lobes are involved with frontal lobe predominance. Changes are confluent and the splenium is also involved. There is no diffusion restriction. What is differential diagnosis after imaging? What additional testing would you recommend? Other Studies Normal CBC, BMP, LFTs, coags Negative HIV test Normal Cortisol, ACTH levels EEG: normal awake and sleep LP: OP 14; 1 WBC, 17 RBC, 29 Glucose, 40 Protein No oligoclonal bands, normal IgG index JC virus Ab negative HSV/VZV pcr’s were negative What is new Differential Diagnosis? Differential Diagnosis Multiple Sclerosis- Marburg type Multiple Sclerosis ADEM Metachromatic Leukodystrophy Adrenoleukodystrophy Pelizaeus-Merzbacher disease Expert summary & interpretation Young patient presented with poor insight into her own behavioral disinhibition and dysexecutive cognitive syndrome. Tone was increased in her legs and gait was mildly spastic. MRI shows confluent bilateral periventricular white matter changes, most prominent frontally LP shows no evidence of inflammation or elevated IgG index Expert summary & interpretation Bilaterally symmetric T2 hyperintensity on MRI is highly uncommon for ADEM or MS and its multiple variants. Lack of IgG index elevation also helps rule out MS. Lack of ataxia, prominent psychiatric presentation, and lack of U-fiber involvement helps rule out PelizaeusMerzbacher disease. Bilateral frontal white matter involvement on MRI, lack of adrenal insufficiency helps rule out Adrenoleukodystrophy (MRI findings of biventricular hyperintensity in parieto-occipital regions). Expert summary & interpretation Psychiatric presentation with mild cognitive decline, spasticity in lower extremities, and MRI with biventricular confluent white matter lesions predominantly in frontal regions most consistent with diagnosis of Metachromatic Leukodystrophy, adult form. Metachromatic Leukodystrophy Metachromatic Leukodystrophy LFB Metachromatic Leukodystrophy LFB Metachromatic Leukodystrophy Cresyl Violet Metachromatic Leukodystrophy LFB / Cresyl Violet (Dentate Nucleus) Metachromatic Leukodystrophy Cresyl Violet Peripheral Nerve Metachromatic Leukodystrophy Cresyl Violet Renal Tubules Tay-Sachs (GM2 gangliosidosis) H&E LFB / PAS PAS Toluidine Blue Leukodystrophies for dummies What is a “Leukodystrophy”? Leuko- white, dystrophy- degenerating Unlike disorders such as MS or GBS where there is loss of previously normal myelin, leukodystrophies present with hypomyelination or dysmyelination Leukodystrophies for dummies- Diagnosis How does Leukodystrophy generally present? Childhood-onset leukodystrophy Presents after normal development; cognitive decline, some personality changes, loss of motor skills Adult-onset leukodystrophy Often presents with slowly worsening cognitive skills and psychiatric abnormalities (often mistaken at first for primary psychiatric disease), lower limb spasticity, sometimes bulbar palsy Leukodystrophies for dummies Types of Leukodystrophy of Adulthood: Adult cerebral X-linked and female heterozygote Adrenoleukodystrophy, Adrenomyeloneuropathy, Alexander disease, Leukodystrophy with neuroaxonal spheroids, Vanishing white matter disease, Metachromatic leukodystrophy Differential Diagnosis Infiltrative tumors (gliomas, CNS lymphoma), Toxic leukoencephalophy (chemo, radiation, drugs of abuse), Metabolic leukoencephalopathy (anoxia, CO poisoning), CNS inflammation (MS, ADEM), Infestion (HIV encephalopathy, PML, encephalitis), Vasculopathy (CADASIL) Leukodystrophies- Diagnosis of Adult-onset forms Metachromatic Leukodystrophy- Autosomal Recessive Defect in lysosomal enzyme Arylsulfatase A leads to accumulation of sulfatide in lipid membranes Diagnostic tests: Arylsylfatase A presence in leukocytes Urinary excretion of sulfatides Adrenoleukodystrophy –X-linked recessive Defect in ABCD1 (adenosine 5’-triphosphate-binding cassette transporter) which maps to Xq28; codes for peroxisomal membrane protein. Diagnostic test: serum very long chain fatty acids Alexander Disease- De novo mutations in majority GFAP gene mutation (GFAP= glial fibrillary acid protein) Pathophysiology possibly related to toxic GFAP aggregates Vanishing White Matter Disease- AR, penetrance age dependent Mutation in eIF2B possibly causes an abnormal unfolded protein response Leukodystrophies for dummiesDiagnosis by MR Imaging Recommended workup for Metachromatic Leukodystrophy CHILDHOOD/JUVENILE FORM: Gait disturbances ataxia, spastic quadriplegia, optic atrophy, peripheral neuropathy decerebrate posturing ADULT FORM: Presents in 20s-30s, sometimes as late as 70’s. Often with psychiatric changes dementia, spastic paraparesis, incontinence. Workup shows: MRI shows diffuse white matter changes (Anterior>Posterior) with U-fiber sparing High urinary excretion of sulfatides Low arylsulfatase A in leukocytes *Little role for traditional neuropathology* Treatments Bone marrow transplant or hematopoietic stem cell transplant Ineffective in symptomatic patients REFERENCES Costello, Daniel J; Eichler, April F; Eichler, Florian S. “Leukodystrophies: Classification, Diagnosis, and Treatment”. The Neurologist 15 (2009): 319-328. Print.