Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
The Quality of Life of People With Schizophrenia
in Boulder, Colorado, and Bologna, Italy
by Richard Warner, Qiovanni de Qirolamo, QabrieUa BeleUi, Carlo Bologna,
Angela Fioritti, and Qiorgio Rosini
median age at marriage is 4 to 6 years later and a larger
proportion of adults live with their family of origin than in
the United States. Italian public psychiatric services, likewise, are in some ways similar to those in the United
States and in other ways different. Italian mental health
systems, like those in the United States, are community
based and use equally few psychiatric hospital beds
(Fioritti et al. 1997). However, in northern Italy especially, employment programs have been more extensively
developed than in the United States, often including
worker cooperatives with a mixed work force of psychiatrically disabled and nondisabled people (Savio and
Righetti 1993; Warner and Polak 1995a), and treatment is
more likely to be delivered by home visiting (Bennett
1985; Tansella et al. 1987; Lesage 1989).
We hypothesized that the dissimilar culture and mental health services in the two countries lead to differences
in the quality of life (QOL) of people with serious mental
illness. For example, mentally ill people in Italy may be
more likely to live with family and to obtain employment
and less likely to marry and to be arrested for a crime. We
further hypothesized that, if objective differences exist,
they would lead to subjective differences in life satisfaction. For example, living at home may be associated with
differences in well-being or in the sense of independence
or privacy. This study uses measures of QOL and unmet
needs to assess the circumstances of people with schizophrenia in two regions, one in the United States and one
in Italy.
Abstract
The aim of the study was to compare the quality of life
(QOL) and needs of people with schizophrenia in comprehensive treatment systems in two countries. One
hundred people with schizophrenia and schizoaffective
disorder were randomly selected from the caseload of
a community mental health center in Boulder,
Colorado, and 70 were similarly selected from public
psychiatric treatment services in and around Bologna,
Italy. Subjects were interviewed with QOL and needs
assessment instruments and rated with the Brief
Psychiatric Rating Scale. Objective QOL measures
favored Bologna subjects over Boulder subjects, particularly with respect to employment, accommodation,
and family life. In a factor analysis, objective QOL
variables sorted separately from subjective satisfaction
ratings, suggesting that they measure different underlying constructs. Patient needs in both Boulder and
Bologna samples were primarily psychological and
social rather than basic survival issues. Boulder subjects were more likely to report accommodation needs.
Many apparent QOL advantages for Bologna subjects
could be attributed to the greater frequency with
which the Italian patients lived with family of origin.
Living with family also appeared to confer practical
benefits in meeting needs. Objective QOL measures
discriminated between patient populations better than
subjective ratings of satisfaction and well-being.
Key words: Quality of life, Italy, transnational
comparison.
Schizophrenia Bulletin, 24(4):559-568,1998.
The Sites
We randomly selected subjects with schizophrenia and
schizoaffective disorder from the caseload of a community mental health center in Boulder, Colorado, and from
public psychiatric treatment services in and around
Bologna, Italy. Because catchment areas for mental
Italy and the United States manifest economic and cultural similarities and differences. Both countries are
advanced industrial societies with large agricultural sectors, developed educational systems, and similar unemployment rates. Distinct differences are evident, however,
in religious affiliation, ethnic diversity, population mobility, and patterns of crime and family life. In Italy, the
Reprint requests should be sent to Or. R. Warner, Mental Health
Center of Boulder County, 1333 Iris Ave., Boulder, CO 80304.
559
Schizophrenia Bulletin, Vol. 24, No. 4, 1998
R. Warner et al.
health programs in Italy tend to be smaller, it was necessary to select Italian subjects from three neighboring treatment agencies to achieve a sufficient sample size. All
subjects were interviewed using the same QOL and needs
assessment instruments. Because small differences in the
characteristics of patient populations can produce significant differences in QOL measures, we held variation to a
minimum by selecting subjects from a circumscribed
diagnostic category in an identical fashion at each site.
Descriptions of the U.S. and Italian sites follow.
Boulder, Colorado. The economy of Boulder County is
based on a mixture of agrarian and high-technology
industries and government employment. Food production
companies, the computer industry, research establishments, and the University of Colorado are all large
employers. The two largest towns in the county are
Boulder (population, 104,000) and Longmont (52,000).
In addition, there are several smaller mountain and plains
communities ranging from suburban to rural. The unemployment rate in Boulder County during the period of the
study averaged 4.3 percent.
The Mental Health Center of Boulder County provides a complete range of inpatient and outpatient services for children and adults to a catchment area of
250,000 people. At any given time, the center is actively
serving about 3,000 clients, more than 600 of whom suffer from a psychosis. The agency has an extensive community support system for adults (Mosher and Burti 1989)
and operates a sheltered workshop, where about 60 clients
work part-time, and a clubhouse that maintains about 30
transitional and supported employment placements.
When necessary, patients are assigned to a small-caseload
team that provides daily contact, case management, medication monitoring, and money management. All patients
who qualify for disability support are enrolled in the
appropriate benefit program.
offers a full range of inpatient and outpatient services for
adults. (Child and adolescent services are more restricted
than in Boulder.) Much treatment is provided by home
visiting and some by coordination with the patient's family doctor. Family support and counseling as well as rehabilitation and vocational services are emphasized.
Supported employment and supervised accommodation
are widely available. The catchment area of Porto has
34,000 people; Saragozza, 38,000; and Bologna north,
172,000. The catchment area population and urban/suburban/rural makeup of the three districts combined are,
therefore, close to those of Boulder County.
Porto. In 1995, the mental health program had an
open caseload at any given time of about 600 patients,
more than 200 with a psychotic illness. The center provides up to 15 "work fellowships" (supported employment placements) and as many as six positions in a
worker cooperative.
Saragozza. The mental health center, in 1995, had
an open caseload of about 650 patients, more than 220
with psychosis. The agency provides about 24 supported
employment placements and 11 jobs in the same worker
cooperative as Porto.
Bologna north. The mental health center had an
open caseload of about 1,800 patients, 600 with psychosis. Treatment programs of the agency include a day
center and a crisis center. The agency provides 46 supported employment placements and 47 worker-cooperative jobs. The consumer-employing cooperatives include
a small ceramics factory and a landscaping and cleaning
enterprise. In addition, employment for patients in family-run agricultural businesses is readily available.
Methods
Each of the two principal investigators works in one of
the two comparison cities. Each spent time in the other
city studying the service system to better understand cultural and program differences. Between August 1994 and
July 1995, subjects with schizophrenia and schizoaffective disorder, aged 18 to 50, were selected (using random
number tables) from the comprehensive community mental health center in Boulder, Colorado, and the three public mental health treatment systems in Bologna. In
Boulder, 207 patients with schizophrenia or schizoaffective disorder in the target age group were enrolled in treatment with the mental health center. Of them, 136 active
cases were randomly selected; 100 consented to an interview and 36 refused. In Porto, from a population of 99
similar patients, 14 subjects were selected; 2 refused to be
interviewed. In Saragozza, 48 subjects were selected
from a population of 88 patients; 12 refused an interview.
Bologna, Italy. The population of Bologna is 390,000.
Three districts in and around the city were selected. The
first, Porto, and the second, Saragozza, are urban. The
third district, Bologna north, is semirural and rural. The
economy of urban Bologna is based on commercial and
manufacturing activities, administrative services for the
Emilia-Romagna region, and the University of Bologna
(90,000 students). The economy of Bologna north
includes a mixture of agrarian and high-technology industries and commercial activities. The unemployment rate
in Bologna during the period of the study averaged 3.3
percent.
Mental health services in Bologna are well developed
and coordinated (Fioritti et al. 1997). Mental hospitals
have been phased out over the past 18 years. Each district
560
Quality of Life in Two Countries
Schizophrenia Bulletin, Vol. 24, No. 4, 1998
In Bologna north, 24 subjects were selected from a population of 250 patients; 2 refused an interview. At each
site, the pool of subjects included patients ranging in
severity from high-functioning to the most severely disturbed. At both sites, some were living in supervised residences. Two patients in Boulder, but no subjects in
Bologna, were in long-term hospital care.
Consenting subjects were interviewed using the
Lancashire Quality of Life Profile (LQOLP) developed by
Oliver (Oliver 1988; Oliver et al. 1996) (a structured
interview based on Lehman's [1983] work) and a needsassessment instrument modified from the user section of
the Camberwell Needs Measure (Thornicroft et al. 1992).
Each instrument is a guided self-report; for this reason
interrater reliability tests were not indicated. The LQOLP
includes subjective ratings of satisfaction and objective
questions in nine life domains including employment,
income, housing, and social and family relations. The
needs-assessment instrument inquires about needs in 16
areas ranging from accommodation to sexual life.
Respondents report who is providing help in each area
and their satisfaction with and the importance of that help.
The interview was conducted by independent, trained
interviewers.
Subjects' psychopathology was rated by the treating
psychiatrist using the Expanded Brief Psychiatric Rating
Scale (BPRS-Expanded; Ventura et al. 1993). Subjects
were diagnosed by psychiatrists using DSM-III-R
(American Psychiatric Association 1987) criteria.
Differences between sites in QOL and needs ratings
were tested using chi-square or t tests. To limit error due
to multiple tests, Bonferroni limits were applied. Additional tests were conducted to examine the relationship
between relevant variables where indicated. Income and
earnings were adjusted using 1994 purchasing power parities, which are the rates of currency conversion that eliminate differences in the cost of living between countries
(Organization for Economic Cooperation and
Development 1995).
Results
Subjects were selected randomly at each site. Because the
selection was not proportional to the total pool of potential subjects at each site, the four samples were initially
analyzed separately. Significant differences were found
between the Italian sites for some demographic, clinical,
and outcome variables (years of education, age at first
psychiatric hospitalization, hours of employment, hourly
wage, and frequency of religious service attendance) but
these differences were considerably smaller and less
numerous than the differences between Boulder and the
three Bologna sites. Consequently, we reanalyzed the
data to compare the Boulder sample with a combined
Bologna sample and, for increased focus and clarity, we
present here the results of this comparison. The analysis
of Boulder and the three separate Bologna sites is available from the authors on request.
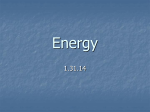
Characteristics of the Sample. Table 1 displays the
characteristics of the sample and those who refused the
interview in Boulder and Bologna. Refusers in Boulder
were more likely to be ethnic minority group members
and low treatment-service users (primarily due to low
treatment need), and less likely to have been recently hospitalized. Refusers in Bologna had greater total psychopathology scores.
Table 2 lists the demographic and clinical characteristics of the Boulder and Bologna samples. Bologna subjects had fewer years of education on average, were more
likely to be living with an unmarried partner, and to be
Catholic.
Across all sites, women were more likely than men to
be married, in a partnership, or divorced/separated
(X2 =15.31; p = 0.0016). Except for marital/partnership
status, gender had no significant relationship to any variable in the study.
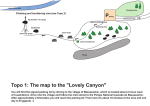
QOL. There were multiple objective QOL differences
between sites, but few differences in subjective satisfaction ratings. Table 3 lists most objective measures of
QOL but only those subjective ratings diat were significantly different between sites after applying Bonferroni
limits.
Table 1. Characteristics of sample and refusers
Boulder
n
Age, mean years
Gender, % male
Ethnic minority, %
Total treatment service
units (July-Dec. 1994)
In psychiatric hospital
in past 6 months, %
Bologna
n
Age, mean years
Gender, % male
Ethnic minority, %
Total psychopathology
score, mean
Note.—NS - not significant.
1
Chi-square.
2
ftest.
561
Sample
Refusers
100
38.1
68.0
9.0
36
38.6
72.2
22.2
NS
NS
0.041
186.5
79.2
0.001 2
21.0
5.5
0.0351
70
37.9
70.0
2.9
16
38.6
68.8
0.0
NS
NS
NS
55.1
68.6
0.0042
P
Schizophrenia Bulletin, Vol. 24, No. 4, 1998
R. Warner et al.
Boulder subjects and less likely to live in supervised
accommodation. The average length of stay in current
accommodation was six times greater for subjects in
Bologna, and more subjects in Boulder than Bologna
expressed a wish to move out of their present accommodation. In the sample as a whole, subjects living with
family had lived longer in current accommodation (207
months) than those who lived apart from family (54
months) (t = 8.28; p = 0.0001); and of those living with
family, 78 percent were in personally owned property
compared with 22 percent who were living apart (X2 =
50.14; p = < 0.0001). Multivariate analysis indicated that
country of residence (F = 78.53; p = 0.0001) and whether
living with family (F = 62.70; p = 0.0001) accounted for a
similar proportion of the variance in the length of residence in current accommodation.
Subjects living with family scored lower overall on
the BPRS-Expanded (49.3; standard deviation [SD] =
15.6) than those not living with family (54.2; SD = 15.6)
(r = 2.18; p = 0.030). Analysis of variance revealed no difference in total BPRS scores between Boulder and
Bologna patients who were living at home. Subjects living
with family reported lower satisfaction with influence at
home {t = 2.06; p = 0.041) and lower overall well-being
(f = 2.12; p = 0.035), but no difference in self-esteem or
satisfaction with independence, privacy, or other residents
of the home, compared with those living apart from family.
Patients from Bologna were more frequently in contact with relatives than were Boulder patients. Family
contact was more frequent among subjects Jiving with
family (X2 = 46.26; p = < 0.0001). Analysis of variance
indicated that living with family explained most of the
variance in frequency of family contact (F = 4.71; p =
0.031) when country of residence was entered into the
equation (F = 0.004; not significant). Both well-being
and self-esteem were positively correlated with satisfaction with frequency of family contact (well-being: r =
0.371, p = 0.0001; self-esteem: r = 0.216, p = 0.007) and
with satisfaction with family relations (well-being: r =
Table 2. Demographic and clinical
characteristics of people with schizophrenia in
Boulder, Colorado, and Bologna, Italy, samples
Boulder
(n = 100)
Bologna
(n = 70;>
P
Demographic
characteristics
37.9
Age, mean years
38.1
NS
Gender, % male
68.0
70.0
NS
9.0
2.9
NS
Ethnic minority, %
Education, mean years
13.0
0.0481
11.8
0.00132
Marital status, %
65.7
81.0
Single
10.0
Married
11.4
With partner
17.1
1.0
5.7
8.0
Divorced/separated
17.1
Have children, %
18.0
NS
Religion, %
24.0
82.9 <0.0001 3
Catholic
1.4
Protestant
29.0
Other
47.0
15.7
Clinical characteristics
Age at first psychiatric
hospitalization, years
23.2
22.5
NS
Psychopathology; mean
53.8
55.1
NS
total BPRS score
Note.—BPRS - Brief Psychiatric Rating Scale—Expanded
(Ventura et al. 1993); NS = not significant.
1
/ value = 1.99.
^hi-square^ 15.70.
^hi-square - 59.76.
For working subjects, the number of months worked
in the past 2 years, the hourly wage, and weekly earnings
(adjusted for cost of living) were all lower in Boulder than
Bologna. Adjusted income was lower for Boulder subjects than for those in Bologna, but this difference did not
exceed Bonferroni limits. More Boulder subjects felt they
had insufficient money to enjoy life.
Bologna patients were more likely to live with family
and to live in personally owned accommodation than
Table 3. Quality of life of people with schizophrenia In Boulder, Colorado, and Bologna, Italy,
samples
Boulder
(n=100)
Objective information
Employment
% Up to 29 hours/week
% 30+ hours/week
% unemployed
Hours worked/week, mean
For working subjects:
Hours worked/week, mean
Months worked in past 2 years, mean
Bologna
(n=70)
t
value
X2
P
7.50
0.024
36.0
8.0
56.0
7.6
30.0
22.9
47.1
12.9
2.43
0.016
17.4
12.1
23.7
18.7
2.10
3.83
0.039
0.0001
562
Schizophrenia Bulletin, Vol. 24, No. 4, 1998
Quality of Life in Two Countries
Table 3. Quality of life of people with schizophrenia In Boulder, Colorado, and Bologna, Italy,
samples (Continued)
Boulder
(n = 100)
Earnings/week, mean US$ corrected
for cost of living1
Hourly wage, mean US$ corrected for
cost of living1
Income
Income/month, mean US$ corrected for
cost of living1
Accommodation
Type, %
Owned house/apartment
Rented house/apartment
Staffed/supervised accommodation
Other (e.g., mobile home)
Living situation, %
With family
Independent
Supervised
Time in present accommodation, mean no. of
months
Number of others in home, mean
Religion
Services attended in past month, mean no.
Legal/safety
Accused of crime in past year, %
Assaulted in past year, %
Family
Frequency of family contact, %
Daily
Weekly
Monthly or less
Friendships
Visited friend in past week, %
Health
Physical handicap, %
Subjective Information
Subjective ratings significantly
different between sites2
Lack money to enjoy life, %
Wanted to move but unable, %
Satisfaction with frequency of doctor
contact, mean score
Bologna
(n = 70)
t
value
83.00
208.56
4.20
0.0001
4.68
9.38
3.93
0.0001
584.53
721.01
2.06
0.042
8.0
64.0
16.0
12.0
61.4
34.3
4.3
0.0
60.82
<0.0001
17.0
67.0
16.0
72.9
22.9
4.3
52.97
<0.0001
38.0
2.2
227.1
2.0
0.71
1.30
x2
11.61
0.0001
NS
2.21
0.028
18.0
15.0
4.3
11.4
7.15
0.007
NS
25.0
39.0
36.0
70.0
5.7
24.3
66.04
<0.0001
71.0
43.3
12.83
0.0003
23.0
7.1
7.53
0.006
72.0
57.0
41.4
31.4
15.96
12.17
4.83
5.51
3.92
0.00006
0.002
0.0001
1
1ncome figures have been adjusted using purchasing power parities, which are the rates of currency conversion that eliminate the differences in price levels (cost of living) between countries. (The 1994 rate from the Organization for Economic Cooperation and
Development, Main Economic Indicators, April 1995, was used.)
2
After applying Bonferroni limits.
with family reported visiting a friend than those not with
family (X2 = 17.46; p = 0.00003). Logistic regression
indicated that living with family (Wald = 17.46; p =
0.00001) exerted a greater effect on whether a subject visited a friend than did country of residence (Wald = 12.48;
p = 0.0004). Well-being (t = 3.24; p = 0.001) and self-
0.353, p = 0.0001; self-esteem: r = 0.172, p = 0.031), but
there was no correlation between actual frequency of family contact and satisfaction with frequency of contact or
with well-being.
Boulder patients were more likely to have visited a
friend in the prior week, and fewer subjects who lived
563
Schizophrenia Bulletin, Vol. 24, No. 4, 1998
R. Warner et al.
with family were less likely to report problems with
accommodation (X2 = 11.71; p = 0.0028) or agency help
with accommodation (r = 4.46; p = 0.0001).
Patients from Bologna frequently cited problems with
home care but reported more family help with home care.
Subjects living with family were more likely to report
family help with home care (t = 5.44; p = 0.0001); they
reported more satisfaction with this help (/ = 3.18; p =
0.003) and attached more importance to home care help
(t = 3.52; p = 0.001).
Subjects in Bologna were more likely to report family help with obtaining food than those in Boulder. Those
living with family were less likely to report agency help
with meals (r = 4.61; p = < 0.001) and were more likely to
report family help (/ = 3.61; p = < 0.001). Those living
with family were also less likely to report agency help
with budgeting (t = 3.88; p = 0.0001).
esteem (/ = 2.16; p = 0.032) were higher among those
who reported having a friend they could turn to for help,
but not among those who reported visiting a friend
recently.
Boulder subjects reported lower satisfaction with
their frequency of contact with a physician. They also
attended fewer religious services and were more likely to
report having been accused of a crime and to report a
physical handicap, but these differences did not exceed
Bonferroni limits.
We conducted a factor analysis of QOL variables
using varimax rotation. Four factors emerged with an
eigenvalue in excess of 3.0 and contributing 6 percent or
more of the variance. Objective measures and subjective
variables loaded on different factors. One factor loaded
subjective measures of social relations (satisfaction with
number of friends, family and interpersonal relations, and
leisure activities outside the home). Another loaded subjective measures of living circumstances (satisfaction with
living situation, satisfaction with privacy, independence
and influence in the home, and willingness to stay for a
long time in current accommodation). A third factor comprised objective measures of family/home circumstances
(living with family, frequency of contact with relatives,
type of accommodation, and length of time in current
accommodation). The fourth factor loaded objective
measures of income and work status (number of hours
worked, earnings, and total income). When the scores for
these factors were entered as dependent variables in separate analyses of variance (using Scheff6 ranges) across all
the sites, only the factor loaded with objective measures
of family/home circumstances distinguished between sites
( F = 14.5; p = < 0.0001).
Discussion
Limitations of the Study. Despite efforts to select similar samples at each site, differences emerged. The education level was lower in Bologna, presumably because
pupils graduate from high school 2 years earlier in Italy
than in the United States. Refusers in Boulder were more
likely to be low treatment-service users and less likely to
have been recently hospitalized, whereas refusers in the
rural Bologna site had higher total psychopathology
scores. The psychopathology of refusers was not measured in Boulder, and rehospitalization of refusers was not
assessed in Bologna, but the findings suggest that in
Boulder refusers were less disturbed than those who
agreed to an interview, whereas in Bologna refusers
tended to be more disturbed. This difference may have
been a result of the low frequency of treatment contact
with high-functioning patients in Boulder and their consequent unwillingness to come in for an interview. There
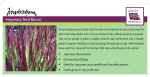
Needs. Table 4 lists the reported needs that were significantly different between sites after Bonferroni limits were
applied. Patients in the Boulder sample were more likely
to report a problem with accommodation. Subjects living
Table 4. Needs expressed by people with schizophrenia in Boulder, Colorado, and Bologna, Italy,
samples
Patient has a problem with (%)
Accommodation
Home care
Family helps with problem, mean
(0 = none, 3 = high)
Home care
Food
Satisfaction with help received, mean
(1 = low, 7 = high)
Home care
Boulder
(n=100)
Bologna
(n = 70)
20.0
20.0
7.4
23.5
r
value
X2
18.02
18.20
P
0.0001
0.0001
0.75
0.97
2.33
2.22
5.97
4.29
0.0001
0.0001
4.30
5.58
4.04
0.0001
Note.—Significant difference between sites after apptying Bonferroni limits.
564
Schizophrenia Bulletin, Vol. 24, No. 4, 1998
Quality of life in Two Countries
was no significant difference between the Boulder and
Bologna samples in any of the symptom clusters of the
BPRS-Expanded. Nevertheless, because one would
expect more stable patients to have objectively better
QOL, that such patients tended to be excluded from the
Boulder sample may have led to an underestimate of average QOL in Boulder.
The private psychiatric treatment sector is relatively
large in Boulder; patients with schizophrenia who are
working and have private health insurance benefits may
be more likely to be in private care and therefore absent
from die Boulder sample. Counterbalancing diis effect is
the possibility uiat some less disturbed people with schizophrenia in Bologna may not have been in treatment due
to die protective effect of living with family.
The differences in place of residence between patient
samples mirror differences in living circumstances of the
general populations in the two countries. In Bologna,
adult offspring are much more likely to live with their
family of origin than they are in Boulder. In Bologna, in
1991, 57 percent of single men aged 30 to 34 and 46 percent of single women of that age were living with tiieir
family of origin (Barbagli and Pisati 1995). Although
comparable U.S. statistics are not available, it is clear that
the American situation is very different. In 1993 in
Boulder, for example, only 3.1 percent of the population
was living in a household in which two adults were blood
related; for example, adult child and parent or adult siblings (Miller and Caldwell 1995). These figures illustrate
profound cultural differences. The value placed on staying close to one's family runs very deep in Italy and goes
far beyond possible financial advantages or the availability of housing. As one Italian sociologist remarked, "If in
the States a young person doesn't want to leave home,
everyone wonders what is wrong with the person. Here
[in Italy], if a young person wants to leave home, everyone wonders what is wrong with the family" (Bohlen
1996, p. 1).
QOL. Several QOL differences favored Bologna over
Boulder: higher rates of marriage and partnership; greater
lengdi of employment, higher wage rates, and greater total
earnings; fewer financial obstacles to the enjoyment of
life; more residential stability and home ownership; more
family contact; and greater satisfaction with physician
access. Other measures, such as frequency of religious
service attendance and reported accusation of criminal
activity, also favored Bologna subjects but did not exceed
Bonferroni limits. Boulder patients, on the other hand,
reported a greater likelihood of visiting friends.
Some QOL advantages for Bologna subjects are
attributable to the greater frequency with which Italian
patients lived with family. In Boulder, 17 percent of subjects were living with family, versus 73 percent in
Bologna. Elsewhere in Italy it is common for a large proportion of people with schizophrenia to live with family
(Lesage 1989); for example, 64 percent of a recent caseregister sample in south Verona (Faccincani et al. 1990)
and 84 percent in Genova (Marinoni et al. 1996). Average
length of stay in current accommodation was six times
greater for the Bologna sample than for Boulder, and, for
subjects who lived with family, length of stay was nearly
four times greater than for those who lived apart from
family. In multivariate analysis, living with family
proved to be a powerful factor in predicting length of residence. Residential stability could be considered particularly important for people with schizophrenia, who are
susceptible to the stress of life changes. Many more
Bologna patients lived in personally owned property,
pointing to greater residential security and probably less
economic stress for Bologna patients.
Although more Italian patients were living at home,
Italian families were not caring for the more severely disturbed patients. Total psychopadiology for patients living
at home was no greater in Bologna than in Boulder. From
die patient's perspective, there were some disadvantages
to living at home. Subjects living widi family reported
reduced well-being and less satisfaction with their influence at home. On the other hand, they did not report
restrictions on their independence or privacy, nor were
they more likely to want to move.
Patients from Bologna were more frequendy in contact with relatives, and multivariate analysis indicated that
die greater frequency of living with family accounted for
this difference. Because family contact was not associated widi increased satisfaction with frequency of family
contact or with well-being, it was not clear to what extent
die high level of contact was a QOL advantage. Boulder
patients, who less often lived with family, appear to have
been more socially outgoing; that is, they were much
more likely to have visited a friend in the prior week.
However, visiting friends per se is not necessarily better
than spending time widi relatives; opinions on this point
are likely to be influenced by culture. Future comparative
research with these populations could profitably explore
die impact of living widi family on social networks, support, and family burden.
Employment programs for people widi mental illness
are often more extensive in Italy dian die United States;
Bologna is no exception. As expected, various measures
Fewer subjects in Bologna reported wanting to move
out of their current accommodation, and multivariate
analysis showed that living with family is a powerful factor in predicting this subjective opinion.
565
Schizophrenia Bulletin, Vol. 24, No. 4, 1998
R. Warner et al.
of employment and earnings favored subjects in Bologna.
Average working hours were greatest in rural Bologna
north, where cooperatives employing patients are well
developed and where work on family farms was available.
The relatively poor employment picture in Boulder,
particularly the low full-time employment rate, may be a
result not only of differences in vocational opportunities
but also of work disincentives inherent in the U.S. disability benefit system (Warner and Polak 1995b). Most
patients in the Boulder sample were receiving either
Supplemental Security Income (SSI) or Social Security
Disability Income (SSDI). Because of a reduction in disability support and other benefits, SSI recipients make
only small gains in income when they begin to work;
SSDI recipients often prefer not to move from part-time
to full-time work because the pension can be discontinued
if the recipient earns more than $500 in any month
(Warner and Polak 1995Z>). In Italy, work disincentives in
this population are milder recipients who work may keep
their pension in addition to earnings until they reach a
much higher earnings limitation.
It is likely that the lower unemployment rate in
Bologna (3.3%) than Boulder (4.3%) influenced the
employment of subjects. It is also possible that average
hours of work for Boulder subjects may have, in fact,
been better than our figures suggest because Boulder
patients who refused to be interviewed may have included
a larger proportion of full-time workers.
Adjusted income was lower for Boulder subjects, in
part because of lower wage rates and fewer hours of
employment. More Boulder patients felt they lacked
money to enjoy life, a finding that could reflect both lower
income and the necessity for patients who live independently to spend their income on such necessities as food
and rent.
Bologna subjects were three times more likely than
Boulder patients to report being in a partnership, married
or otherwise—an important QOL advantage for Bologna
subjects. The greater income and residential stability of
Bologna patients may have made marriage and partnership more feasible. The high rate of unmarried partnership in the Bologna sample may reflect the long delay In
remarriage after divorce under Italian law.
The substantial differences between Italy and the
United States in the general availability of health care
might have been expected to produce differences between
the samples. Boulder patients reported a high rate of
physical disability and greater dissatisfaction with their
frequency of contact with a physician. Even greater differences might have emerged in a comparison with an
American community other than Boulder, where indigent
health clinics make care widely available.
566
Several of the QOL differences between the Boulder
and Bologna samples are factors that, in other research,
have been associated with differences in outcome. In a
case-register study of patients with schizophrenia in south
Verona, the stongest and most consistent predictors of
poor outcome included living alone, unemployment, and
being unmarried. As the authors point out, "Patients who
were isolated or lacked social support—the unmarried, the
unemployed, those living alone, and those without religious affilitation—were disproportionately heavy users of
the mental health services" (Thornicroft et al. 1993,
p. 486). It is not clear that these social factors lead to
poor outcome, but a bidirectional pattern of causality is
possible (Thornicroft et al. 1995). If so, patients in
Bologna may be more likely to achieve stability and low
need for services.
Subjective and Objective Measures. We distinguish
between subjective and objective QOL data in this article,
even though, because all the information was gathered by
interviewing subjects, it could all be considered subjective. Here, "objective" refers to a fact, such as income or
religious affiliation, reported by the subject; "subjective"
refers to the level of satisfaction about some aspect of life.
Subjective satisfaction ratings revealed few differences
between the samples despite major differences in objective QOL measures. Subjects may be limited by the horizons of their experience in making subjective ratings. As
Barry and Crosby (1996) comment, "Expressed levels of
life satisfaction, which generally tend to be quite high
regardless of the population surveyed, are not absolute
indicators of life quality . . . their reporting is subject to a
whole host of cognitive and social factors" (p. 215).
In a factor analysis of the QOL variables, four major
factors emerged; objective measures and subjective variables loaded onto different factors, suggesting that they
measure different underlying constructs. When the four
factors were entered as dependent variables in separate
analyses of variance, only the factor loaded with objective
measures of family and home circumstances distinguished
between sites. These findings, which confirm earlier
research, suggest that assessment aimed at distinguishing
outcome for people with schizophrenia in different treatment systems should include both objective and subjective measures.
Needs. There was no difference between samples in the
average number of unmet needs, but some needs were
more prominent in one sample than the other. It is likely
that, as material circumstances change, people do not
reduce their total needs but change earlier needs for new
ones. The most prominent needs in both U.S. and Italian
Schizophrenia Bulletin, Vol. 24, No. 4, 1998
Quality of Life in Two Countries
samples were primarily psychological or social; these
include problems with psychological health, finding work
or daily activities, maintaining social contacts, obtaining
information about one's illness, and maintaining an adequate sex life. Problems with obtaining basic needs such
as housing, food, financial benefits, or personal care were
not commonly reported in either country. Boulder
patients frequently reported problems with physical
health, and concerns about home care were common
among Bologna subjects. These findings are similar to
those of a study of outpatients with schizophrenia in south
Verona in which unmet clinical needs outnumbered living
skills needs by four to one (Lesage et al. 1991).
As observed in the case of QOL measures, patient
needs also appeared to be influenced by the higher frequency with which patients in Bologna were living with
family. Families in Bologna often met needs that in
Boulder were more likely to be addressed by the treatment service system. Thus, patients in the Bologna samples and subjects living with family were less likely to
report a problem with accommodation, more likely to
report family help with home care and with obtaining
food, and less likely to report agency help with budgeting.
3rd ed., revised. Washington, DC: The Association,
1987.
Barbagli, M., and Pisati, M. Rapporto sulla situazione
sociale a Bologna. Bologna, Italy: n Mulino, 1995.
Barry, M.M., and Crosby, C. Quality of life as an evaluative measure in assessing the impact of community care
on people with long-term psychiatric disorders. British
Journal of Psychiatry, 168:210-216, 1996.
Bennett, D.H. The changing pattern of health care in
Trieste. International Journal of Mental Health,
14:70-92, 1985.
Bohlen, C. For young Italians, there's no place like home.
International Herald Tribune, March 14, 1996, p.l.
Faccincani, C ; Mignolli, G.; and Platt, S. Service utilisation, social support and psychiatric status in a cohort of
patients with schizophrenic psychoses: A 7-year follow-up
study. Schizophrenia Research, 3(2): 139-146, 1990.
Fioritti, A.; Lo Russo, L.; and Melega, V. Reform said or
done: The case of Emilia-Romagna within the Italian
psychiatric context. American Journal of Psychiatry,
154(l):94-98, 1997.
Lehman, A.F. The well-being of chronic mental patients:
Assessing their quality of life. Archives of General
Psychiatry, 40:369-373, 1983.
Conclusion
Lesage, A.D. Social factors affecting caseload in Italian
good practice areas. International Journal of Social
Psychiatry, 35:54-61, 1989.
Although some differences could be the result of case
selection bias, the QOL of people with schizophrenia in
our samples appears to be materially better in Bologna
than in Boulder. Some QOL advantages appear to result
from the fact that more patients in Bologna were living
with family. Family living was associated with such
advantages as greater residential stability, more home
ownership, and more contact with relatives. For those living at home, families meet a number of needs such as
accommodation, food, home care, and budgeting. As a
result, it is possible that the treatment service system in
Bologna was not required to invest its resources in meeting these basic needs to the same extent as in Boulder.
This may have made it more feasible for the psychiatric
services in Bologna, as elsewhere in northern Italy, to
develop home-based counseling and comprehensive
employment opportunities for patients than is the case in
Boulder. Thus, even though vocational services in
Boulder were well developed by U.S. standards, work
tenure and earnings were superior for Bologna subjects
compared to Boulder patients.
Lesage, A.D.; Mignolli, G.; Faccincani, C ; and Tansella,
M. Standardized assessment of the needs for care in a
cohort of patients with schizophrenic psychoses.
Psychological Medicine, 19:27-33, 1991.
Marinoni, A.; Boidi, G.; Botto, G.; Ciancaglini, P.;
Guamieri, A.; and Lussetti, M. "Prezentazione dei primi
dati di follow-up a 5 anni della ricerca sulla schizofrenia
in Liguria." Paper presented at II Decorso della
Schizofrenia: Studi sul Follow-up, Genova, Italy, June 6,
1996.
Miller, M., and Caldwell, E. Boulder Citizen Survey:
1995. Boulder, CO: City of Boulder, 1995.
Mosher, L.R., and Burti, L.R. Community Mental Health:
Principles and Practice. New York, NY: W.W. Norton,
1989.
Oliver, J.P.J. The Quality of Life of the Chronically
Mentally Disabled in the Preston/Chorley Area of
Lancashire: Research Progress Report. Manchester,
England: Mental Health Social Work Research Unit,
University of Manchester, 1988.
References
American Psychiatric Association.
Oliver, J.; Huxley, P.; Bridges, K.; and Mohamad, H.
Quality of Life and Mental Health Services. London,
England: Routledge, 1996.
DSM-III-R:
Diagnostic and Statistical Manual of Mental Disorders.
567
Schizophrenia Bulletin, Vol. 24, No. 4, 1998
R. Warner et al.
Organization for Economic Cooperation and Development. Main Economic Indicators. Geneva, Switzerland:
The Organization, April 1995.
Warner, R., and Polak, P. The economic advancement of
the mentally ill in the community: 1. Economic opportunities. Community Mental Health Journal, 31(4):381-396,
1995a.
Savio, A., and Righetti, A. Cooperatives as a social enterprise in Italy: A place for social integration and rehabilitation. Ada Psychiatrica Scandinavica, 88(4):238-242,
1993.
Warner, R., and Polak, P. The economic advancement of
the mentally ill in the community: 2. Economic choices
and disincentives. Community Mental Health Journal,
31(5):477^92, 1995*.
Tansella, M.; de Salvia, D.; and Williams, P. The Italian
psychiatric reform: Some quantitative evidence. Social
Psychiatry, 22:37^*8, 1987.
Acknowledgments
Thornicroft, G.; Bisoffi, G.; de Salvia, D.; and Tansella,
M. Urban-rural differences in the associations between
social deprivation and psychiatric service utilization in
schizophrenia and all diagnoses: A case-register study in
Northern Italy. Psychological Medicine, 23:487^96,
1993.
Thomicroft, G.; Breakey, W.R.; and Primm, A.B. Case
management and network enhancement of the long-term
mentally ill. In: Brugha, T.S. ed. Social Support and
Psychiatric Disorder: Research Findings and Guidelines
for Clinical Practice.
New York, NY: Cambridge
University Press, 1995. pp. 239-256.
The authors acknowledge the assistance and support of
Vittorio Malaga, M.D., Chief of the Department of Mental
Health, Azienda, Bologna, Italy, at the time of the study;
and Francesco Coppa, M.D., Antonella Piazza, M.D., and
Ellen Frank, Ph.D., for comments on an earlier draft.
The Authors
Richard Warner, M.B., D.P.M., is Medical Director,
Mental Health Center of Boulder County, and Clinical
Professor of Psychiatry and Adjunct Professor of
Anthropology, University of Colorado, Boulder, CO.
Giovanni de Girolamo, M.D., is Psychiatrist; Carlo
Bologna, M.D., is Psychiatrist; Angelo Fioritti, M.D., is
Psychiatrist; and Giorgio Rosini, M.D., is Psychiatrist, all
at the Department of Mental Health, Azienda Bologna,
Italy. Gabriella G. Belelli, M.D., is Psychiatrist,
Department of Mental Health, Azienda Bologna Nord,
San Giorgio di Piano, Italy.
Thornicroft, G.; Brewin, C ; and Wing, J. Measuring
Mental Health Needs. London, England: Royal College
of Psychiatrists, 1992.
Ventura, J.; Lukoff, D.; Nuechterlein, K.H.; Liberman,
R.P.; Green, M.F.; and Shaner, A. Brief Psychiatric
Rating Scale (BPRS): Expanded version (4.0). In:
Training and quality assurance with the BPRS.
International Journal of Methods in Psychiatric Research,
3:221-224, 1993.
568