Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
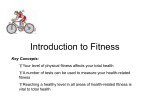
INVITED COMMENTARY Physically Active Subjects Should Be the Control Group FRANK W. BOOTH and SIMON J. LEES Health Activity Center, Departments of Biomedical Sciences and of Medical Pharmacology and Physiology, University of Missouri, Columbia, MO M higher cardiovascular fitness are healthier relative to sedentary/unfit individuals. From such information, The U.S. Centers for Disease Control (CDC) identify physical inactivity as an actual cause of disease (3). The CDC published that heart disease and malignant neoplasm were the two leading causes of deaths in the United States in 2000, whereas the two actual causes of deaths were tobacco, then poor nutrition and physical inactivity (3). Physically inactive lifestyles are an actual contributing cause of Alzheimer’s disease, breast cancer, colon cancer, coronary artery disease, obesity, osteoporosis, sarcopenia, type 2 diabetes, and others (2). Therefore, physical inactivity and chronic disease are not two separate disciplines—they are inevitably linked, and this point seems to have been underemphasized. ost publications with a physical exercise group use sedentary (physically inactive) subjects as the ‘‘control’’ group. Our brief commentary will contend an alternative approach based on the premise that physically active individuals are healthier than sedentary individuals, and therefore, the physically active subjects should compose the control group. The designation of sedentary subjects as ‘‘control’’ has spontaneously happened without premeditated planning. The control group at the beginning of the 1900s was physical education students who were physically active (Fig. 1). These physically active students undertook additional exercise as the treatment group, approaching the fitness level of elite athletes. Sedentary individuals were likely rare in 1900, a time before automobiles, industrial assembly lines with machines, computers, and convenience technologies. During the next 100 years, the treatment group of exercise remained the same, but the control group went from physically active to sedentary. Thus, controls for most exercise studies went from physically active to sedentary during the 20th century. Organizations such as the American College of Sports Medicine have members who have contributed studies proving that subjects with moderate physical activity/ Editor’s Note: In his 2005 Joseph B. Wolffe Memorial Lecture, Dr. Frank Booth, one of ACSM_s most esteemed basic scientists, argued that researchers studying physical activity effects on health-related outcomes should adopt a new perspective when designing their studies. Dr. Booth’s arguments were persuasive, passionate, and, merit our strong consideration. His perspective is summarized in this invited commentary. FIGURE 1—Schematic for the proper designation of experimental groups in 2006. In 1900, almost all individuals were physically active in their daily lifestyles; further physical education students served as controls for exercise studies (shown as the second highest activity state in the closed horizontal box). In 1900, there were few, if any, ‘‘elite athletes,’’ but exercise training moved physically active physical education students toward the top physical activity state (top horizontal line). In 2006, the majority of individuals have less than 30 min of physical activity each day, the generally agreed threshold level for health benefits from physical activity; these individuals are identified as ‘‘sedentary’’ (third activity state). The lowest shown activity state is continuous bed rest (bottom horizontal line). In reality, there is a spectrum of health and activity (up and down arrow to left) states. Overtraining reduces health (suppressed immune system) in the elite athlete (not shown). Address for correspondence: Frank W. Booth, Ph.D., Department of Biomedical Sciences, University of Missouri-Columbia, E102 Veterinary Medical Building, 1600 East Rollins Road, Columbia, MO 65211; E-mail: [email protected]. Submitted for publication November 2005. Accepted for publication November 2005. 0195-9131/06/3803-0405/0 MEDICINE & SCIENCE IN SPORTS & EXERCISEÒ Copyright Ó 2006 by the American College of Sports Medicine DOI: 10.1249/01.mss.0000205117.11882.65 405 Copyright @ 2006 by the American College of Sports Medicine. Unauthorized reproduction of this article is prohibited. Two professions use different criteria for assignment to ‘‘control.’’ The ‘‘control’’ group from the medical profession most often contains the healthier subjects, while the ‘‘control’’ group from the exercise profession usually has unhealthier, sedentary subjects (Fig. 1). We believe that when the sedentary group is used as the control group in exercise studies it facilitates a misinterpretation that exercise experts think sedentary individuals are healthy enough, based upon the common designation in medical journals that the control group is the healthy group. The control/normal condition for the human genome for hundreds of thousands of years was selective to environmental pressures, prominently from infrequent periods of starvation and frequent sessions of moderate physical activity (shown as the second physical activity level in the enclosed box in Fig. 1). According to Neel_s Thrifty Gene Hypothesis (4), genomes of many species were ‘‘fine-tuned’’ to efficiently store and utilize foods over the ages. Since during the majority of human existence on Earth, physical activity was a selective pressure on genes for survival, genes were selected to perfect metabolism to support physical activity. Surprisingly in the absence of physical activity, inherited metabolic pathways produce metabolic chaos (1). The relatively recent (i.e., the last 100 years) dramatic decline of physical activity from daily living has removed the human genome from its expected frequent sessions of moderate physical activity (shown as the sedentary activity level in Fig. 1; (2)). The disorders that accompany sedentary lifestyle are largely disorders of improper food storage and utilization (atherosclerosis, obesity, type 2 diabetes). In contrast, physical activity causes ‘‘metabolic health.’’ Therefore, physical inactivity and metabolic disorders are inevitably linked as one. Major questions in medical sciences should be those that have the highest societal impact. A current major question is ‘‘what causes chronic disease?’’; in many cases, the actual cause can be largely attributed to physical inactivity. Therefore, the best game plan might be to set up a research plan that is aimed at investigating the actual cause(s) of chronic disease as it relates to physical inactivity as the abnormal, unhealthy condition; healthier physically active individuals should be assigned to the control group. REFERENCES 1. BOOTH, F. W., M. V. CHAKRAVARTHY, and E. E. SPANGENBURG. Exercise and gene expression: physiological regulation of the human genome through physical activity. J. Physiol. 543:399–411, 2002. 2. CHAKRAVARTHY, M. V., and F. W. BOOTH. Hot Topics: Exercise. Philadelphia, PA: Hanley and Belfus (Elsevier), 2003. 406 Official Journal of the American College of Sports Medicine 3. MOKDAD, A. H., J. S. MARKS, D. F. STROUP, and J. L. GERBERDING. Actual causes of death in the United States, 2000. JAMA 291:1238–1245, 2004. 4. NEEL, J. V. Diabetes mellitus: a ‘‘thrifty’’ genotype rendered detrimental by ‘‘progress’’? Am. J. Hum. Genet. 14:353–362, 1962. http://www.acsm-msse.org Copyright @ 2006 by the American College of Sports Medicine. Unauthorized reproduction of this article is prohibited.