Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Electrocardiography wikipedia , lookup
Hypertrophic cardiomyopathy wikipedia , lookup
Cardiac surgery wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Mitral insufficiency wikipedia , lookup
Atrial fibrillation wikipedia , lookup
Lutembacher's syndrome wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
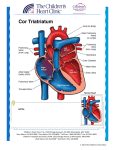
830 lACC Vol. 9 . No. 4 April 19R7:830-3 Pulmonary Venous Obstruction and Atrioventricular Canal Anomalies: Role of Cor Triatriatum and Double Outlet Right Atrium THOMAS J. STARC, MD, FREDRICK Z. BIERMAN , MD, FACC, FREDERICK O. BOWMAN, JR. , MD, CARL N. STEEG, MD, FACC, NK WANG , MD, EHUD KRONGRAD , MD, FACC New York. New York Two-dimensional echocardiographic findings and surgical repair in three infants with atrioventricular (AV) canal and pulmonary venous obstruction are described. The AV canal was complicated by cor triatriatum in two patients and by double outlet right atrium in the other. Atriove ntricular (AV) ca nal type defects are often associated with pulm onary hypertension and the ea rly onset of pulmonary vasc ular ob stru ct ive disease . Anatomic cau ses of obstru ct ion to pulmonary venous return are rare in these patients ( I) . Thi s report describ es the two-d imensional echocardiog raphic findings and surgica l management of three infant s with AV canal and obstruction of pulm onary venous drai nage . The obstructio n was seco ndary to cor triatr iatum in two pat ients and seco ndary to doubl e outlet right atrium in the other. Case Reports Case I . Complete AV Canal and Cor Triatriatum History. A 6 month old boy with failure to thri ve , perioral cya nos is and tach ypnea since the first weeks of life was referred for ev aluatio n of complete common AV canal with " irre versible " pulm onary vasc ular obstructive disease . Cardiac ca theterization at 4 month s of age at the referring institut ion demonstrated complete AV ca nal with a common AV valve . Pulmonary and sys temic arte rial systolic pressures were eq ual. A pulm onary artery wedge pressure was not obtained . There was a small left to right shunt with a pulm onary to sys temic flow ratio of 1.4/ I . Pulm onary artery From the Cardiology Division of the Department of Ped iatrics and (he Card iothorac ic Division o r the Department or Surgery. Co lumbia University. College or Physicians and Surgeons. New York. New York. Manuscript received May 23 . 1986: revised man uscript received October 21. 1986 . acce pted Nove mbe r 17 . 1986 . Add ress for reprints: Thom as J. Stare. MD. Co lumbia University. Co llege of Physicians and Surgeon s. Room BHSI -102A . 630 West 168 Street. New York . New York 10032. © 1987 by the American Collegeof Cardiology In patients with AV canal, anatomic ohstruction of pulmonary venous return should be excluded by detailed cardiac ultrasound examination . () Am ColI Cardiol 1987;9:830-3) pressure and pulmonary artery blood flow did not change administration of oxyge n. The left atrium was not en tered . AT 6 months of age the infant was thin and tachypneic with mild cya nosis . The height and weig ht were less than the fifth percentile for age. Th e precord ium was active. The second heart sound was loud and single. A grade 3/6 holosystol ic murmur was present at the lower left sternal border. There was no diastol ic murmur. The liver was palpabl e 2 em below the right costa l margin. Laboratory findings. The chest X-ray film showed a large heart and increased pulmonary vascular markings. The electrocardiogram (ECG) showed normal sinus rhythm . right superior ax is and right vent ricul ar hypertrophy . The PR interval was 0.14 ms. Two-d imen sional echocardiography confirmed the diagnosis of co mplete AV ca nal. but also demonstrated cor triatriatum . In co ntrast to the normal configuration of the interatrial sept um and left atrium (Fig. I), in this patient a membrane ex tended from the superio r portion of the atrial septum to the lateral left atria l wall inserting above the left atrial appendage (Fig. 2) . The pulmonary veins drain ed into a common pulm onary venous chamber that co mmunicated with the atr ia through a small orifice in the membrane. Surgical findings. Surgery at 7 month s of age dem on strated a large right atrium that led directly throu gh a common AV valve into both right and left ventricles. The AV valve had a divided anterior leaflet and a common poste rior leaflet. A membrane extending from the midportion of the common atrium to the left atrial wall just abo ve the left atrial appendage was ident ified . There was a small opening in the membrane that allow ed pulm onary venous blood to 0 11 0735-1097 /87/$3.50 JACC Vo!. 9. No.4 April 19H7:S30~3 Figure 1. Normal infant. Subxiphoid atrial long-axis projection demonstrating normal configuration of the interatrial septum, left atrium (LA) and left atrial appendage (LAA). The atria are partitioned by the interatrial septum and the leftatrium is continuous with the left ventricular inflow (LVI). I = inferior; L = left; R = right; RA = right atrium; S = superior. enter the common atrium. The atrial membrane was completely excised and the AV canal was repaired using a double patch technique. Pericardium was used to partition the atria. The postoperative course was unremarkableexcept for moderately severe postpericardiotomy syndrome. Case 2. Partial AV Canal and Cor Triatriatum History. A 6 month old girl with oral-facial-digital syndrome and partial AV canal was referred for evaluation of failure to thrive and respiratory distress. On arrival she was intubated and in moderate respiratory distress. Chest examination revealed bilateral ronchi and wheezes. The precordium was active. The first and second heart sounds were normal. A grade 2/6 systolic ejection murmur was heard at the left upper sternal border. There was no diastolic murmur. The liver was palpable 3 cm below the right costal margin. Laboratory studies. The chest X-ray film showed a large heart and increased pulmonary vascular markings. The ECG showed normal sinus rhythm, a left superior axis and right ventricular hypertrophy. The PR interval was O. 10 ms. Two-dimensional echocardiography demonstrated a large ostium primum type defect and cor triatriatum. A membrane separated the common pulmonary venous chamber from the remainder of the left atrium. A small defect was noted in the membrane and pulsed Doppler echocardiography demonstrated restrictive blood flow across the defect (Fig. 3). Surgical findings. Surgery confirmed the diagnosis of partial AV canal and cor triatriatum. In addition, a left superior vena cava was noted. The opening between the common pulmonary venous chamber and the remainder of the atrium was approximately I ern in diameter. Before STARe ET AL. AV CANAL AND PULMONARY VENOUS OBSTRUCTION 831 Figure 2. Patient I. Subxiphoid atrial long-axis projection in a patient with complete AV canal and cor triatriatum. The obstructing membrane extends from the superior portion of the atrial septum and inserts on the lateral left atrial wall, above the left atrial appendage (LAA). *Atrial septal defect; CPV = common pulmonary vein; RVI = right ventricular inflow; other abbreviations as in Figure I. institution of cardiopulmonary bypass, the right ventricular pressure was 35 mm Hg, systemic arterial pressure was 90/50 mm Hg. right superior pulmonary vein pressure was 5 mm Hg (mean) and 10 mm Hg (ac wave) and mean right atrial pressure was 2 mm Hg. The left atrial membrane was resected. Pericardium was used to partition the atria. The postoperative course was unremarkable. Case 3. Complete AV Canal and Double Outlet Right Atrium History. An 18 month old girl with Down's syndrome was referred with cyanosis and congestive heart failure presumed to be secondary to complete AV canal. Symptoms of congestive heart failure were moderately relieved by pulmonary artery banding at 6 months of age. At 18 months of age, the infant was moderately cyanotic, but in no acute respiratory distress. The precordiumwas active. The second heart sound was single. A grade 3/6 holosystolic murmur was heard at the lower left sternal border. There was no diastolic murmur. The lungs were clear to auscultation and the liver was not enlarged. Laboratory findings. The chest X-ray film showed a slightly enlarged heart and a small increase in pulmonary vascular markings. The ECG showed normal sinus rhythm and a right superior axis with severe right atrial and right ventricular enlargement. The PR interval was 0.16 ms. Two-dimensional echocardiography demonstrated situs solitus, normally related great arteries and a complete AV canal. In contrast to the usual findings with complete AV canal, the atrial septum deviated leftward and joined the 832 STA RC ET AL. AV CAN AL AND PULMON ARY VENOUS OBSTRUCTION JACe Vol. 9. No.4 April 1987:83G-3 Figure 3. Patient 2. Left atrial flow profile in infant with primum type atrial septal defect and cor triatriatum . A, Subxiphoid atrial long-axis projection (right) with pulsed Doppler sample volume in the body of the left atrium (LA) at the ostium of the membrane. Turbulent monophasic flow (left) reflects restrictive communication between the common pulmonary venous channel (CPY) andthebody of left atrium. B, Same projection with sample volume placed inthecommon pulmonary venous channel(CPY)(right). Baseline oscillation of flow (left) contrasts with the profile of acceleration in the left atrium (LA) across the ostium of the intraatrial membrane. Other abbreviations as in Figures I and 2. lateral wall of the left atrium , above the plane of the AV groove . The left atrial appendage was proximal to the atrial septum . The left atrium did not communicate directly with the left ventricle (Fig. 4). Cardiac catheterization documented a left to right atrial shunt and a bidirectional shunt at the ventricular level. Left ventricular oxygen saturation was 72%. A 60 mm Hg pressure gradient was present across the pulmonary artery band. The left atrium could not be entered despite multiple attempts to cross the interatrial septum . Surgical findings. Surgery at 18 months of age showed a markedly dilated right atrium. The atrial septum inserted on the lateral wall of the left atrium , above the opening of the common AV valve . The foramen ovale measured 2 to 3 mm in diameter. The coronary sinus was large, secondary to persistence of the left superior vena cava. The pulmonary veins drained normally into the left atrium. The atrial septum was resected from below the level of the foramen ovale, and a new interatrial septum was constructed with pericardium establishing continuity between the left atrium and left ventricle. The remainder of the AV canal was repaired by double patch technique with a Teflon patch closure of the interventricular septum. Cardiac catheterization 6 weeks after surgery showed mild to moderate mitral insufficiency, mild tricuspid insuf- Figure 4. Patient 3. Subxiphoid atrial long-axis projection demonstrating a double outlet rightatrium (RA). The interatrial septum deviates posteriorly and leftward inserting below the left atrial appendage (LAA). Mitral atresia was excluded by ventricular shortaxis projections displaying a " rectangular shaped " common AY valve. *Atrial septal defect; other abbreviations as in Figures I and 2. JACC vot. 9. No.4 STARe ET AL. AV CANA L AND PULMONARY VENOUS OBSTRUCTION April 19H7:8JO--3 ficiency and angiographic evidence of a trivial left to right interventricular shunt. Pulmonary artery pressure was 45/16 mm Hg. Discussion Pulmonary hypertension is a commonproblem in patients with complete AV canal and, when associated with high pulmonary vascular resistance. is a contraindication to surgical repair. AV canal type defects are rarely accompanied by anatomic pulmonary venous obstruction. However, because this combination could possibly mimic irreversible pulmonary vascularobstructivedisease, it must be diligently sought for in any patient with elevated pulmonary artery pressure. Cor triatriatum. In the first two cases, cor triatriatum was the anatomic cause of pulmonary venous obstruction . Cor triatriatum is rarely combined with AV canal defect (1,2). Five patients with cor triatriatum and an ostium primum defect (3-6) and two with complete AV canal ( I) have been previously reported. Symptoms in patients with AV canal and cor triatriatum are variable and relate to the quantity of pulmonary blood flow and the degree of pulmonary venous obstruction. Double outlet right atrium. Our third patient demonstrated an equally rare anomaly, double outlet right atrium. In this lesion, the interatrial septum joins the lateral wall of the left atrium above the orifice of the left AV valve and effectively blocks left atrial blood from entering the left ventricle. Left atrial blood flows into the right atrium and then passes into both the right and the left ventricle. Symptoms are variableand are related to the degree of obstruction of pulmonary venous bloodflow and the associated anatomic defect. Double outlet right atrium is usually associated with an ostium primum defect (7-11) but has also been described in patients with a common AV valve (10-13). an overriding AV valve (13) and three AV valves (14 y. Utility of two-dimensional echocardiography. In the two patients who underwent cardiac catheterization, the diagnosis of anatomic pulmonary venous obstruction was not apparent on cineangiography. The proper diagnosis was ultimately made by two-dimensional echocardiography. Cor triatriatum and double outlet right atrium were identified on two-dimensional echocardiography by the presence of an atrial membrane or the abnormal course of the atrial septum. They were distinguishable by the position of the left atrial appendage. In cor triatriatum, the left atrial appendage was located distal to the atrial membrane-that is. it was part of the low pressure left atrium-whereas in double outlet right atrium, the left atrial appendage was proximal to the interatrial septum-that is, it was part of the high pressure left atrium. Conclusion. Pulmonary vascular obstructive disease is a contraindication to surgical repair in patients with AV 833 canal. It is essential to identify patients with correctable anatomic causes of pulmonary venous obstruction and pulmonary hypertension . Causes of pulmonary venous obstruction include mitral stenosis, supravalvular mitral ring or membrane, double outlet right atrium, cor triatriatum and pulmonary vein stenosis. Two-dimensional echocardiographyhas been useful in identifying each of these obstructive lesions except for isolated stenosis within the pulmonary veins themselves. Although rare, anatomic causes of pulmonary venous obstruction such as cor triatriatum and double outlet right atrium should be considered when elevated pulmonary vascularresistanceis found in patientswith complete AV canal. These defects can be documented by twodimensional echocardiography and are amenable to surgical repair. We thank Rise H. Victor for secretarial assistance. References I. Thilenius OG, Vitullo D. Bharati S. et al. Endocardial cushion defect associated with cor triatriatum sinistrum or supravalve mitral ring. Am J Cardiol 1979:44: 1339--43. 2. Thilenius OG. BharatiS. Lev M. Subdivided left atrium: an expanded concept of cor triatriatum sinistrum. Am 1 Cardiol 1976;37:743-52. 3. Gahagan T. Ziegler RF. Triatrial heart with persistent ostium primum and cleft mitral valve. Ann Thorne Surg 1967:3:231--4. 4. Inoue H. Niitsu K. Iwabushi K. Successful treatmentof cortriatriatum associated with ostium primum defect. Jpn J Thorac Surg 1972;25: 593-6. 5. Nakano S. Kawashima Y. Naito Y. et al. Surgical treatment of cor triatriatum. Jpn J Thorac Surg 1972;25:541--8. 6. Marin-Garcia 1. Tandon R. Lucas RV Jr, Edwards JE. Cor triatriatum: study of 20 cases. Am 1 Cardiel 1975;35:59--66. 7. Corwin RD. Singh AK. Karlson KE. Double-outlet right atrium: a rare endocardial cushion defect. Am Heart J 1983:106:1156--7. 8. Perez-Martinez VM. Garcia-Fernandez F. Oliver-RuizJ. Nunez-Gonzalez L. Double-outlet right atrium with two atrioventricular valves and left atrial outlet atresia. J Am Coli Cardiol 1984:3:375-80. \). Nunez L. Gil Aguado M. Sanz E. Perez Martinez V. Surgical repair of double-outlet right atrium. Ann Thorac Surg 1984;37:164-6. 10. Alivizatos P. Anderson RH. Macartney FJ. ZuberbuhlerJR, Stark J. Atrioventricular septal defect with balanced ventricles and malaligned atrial septum: double outlei right atrium. J Thorac Cardiovasc Surg 1985:89:295--7. II. Utley JR. Noonan JA. Walters LR. Frist RA. Anomalous position of atrial septum with anomalous pulmonary and systemic venous drainage. Correction including ligation of persistent left superior vena'cava. 1 Thorac Cardiovasc Surg 1974;67:730-2. 12. Van Mierop LHS. Pathology and pathogenesis of endocardial cushion defect: surgical implications. In: Davila JC , ed. Second Henry Ford Hospital International Symposium on Cardiac Surgery. New York: Appleton-Century-Croft s , 1977:201-7 . 13. Otero Coio E. Calabro R. Marsico F. Lopez Arranz lS . Right atrial oullet atresia with straddling left atrioventricular valve. A form of double outlet atrium. Br Heart J 1981;45:3 17-24. 14. Buchler1. RabeloR. MarinoR. David I. Van PraaghR. Doubleoutlet right atrium: autopsied case of newly recognized entity (abstr). In: Stone S. ed. WorldCongressof Paediatric Cardiology, London, 1980. Southwick. Sussex, England: Grange Press. 1980:223.