Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
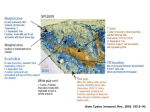
Effective Strategies to Support Families through Reunification Improving Family Drug Courts Family Strengthening Outcomes Partnerships Phil Breitenbucher, MSW Alexis Balkey, BA, RAS June 2, 2016 | NADCP Acknowledgement This presentation is supported by: Strengthening Partnerships Improving Family Outcomes Substance Abuse and Mental Health Services Administration Center for Substance Abuse Treatment and the Administration on Children, Youth and Families Children’s Bureau Office on Child Abuse and Neglect Points of view or opinions expressed in this presentation are those of the presenter(s) and do not necessarily represent the official position or policies of the above stated federal agencies. Learning Objectives Strengthening Partnerships Improving Family Outcomes • Understand the impact of parental substance use on the parent-child relationship and the essential service components needed to address these issues. • Understand family readiness as a collaborative practice issue and why “team” is just as important as any “tool” for assessing readiness. • Learn various case management strategies, including implementation of quality visitation and contact, evidence-based services, coordinated case plans and effective communication protocols across child welfare, treatment and court systems. FDC Practice Improvements Approaches to child well-being in FDCs have changed In the context of parent’s recovery Child-focused assessments and services Familycentered Treatment (includes parent-child dyad) Sacramento County, CAM Project, Children in Focus (CIF) Across all FDC programs, Sacramento is getting ready to admit its 5,000th parent! FDC CIF • Dependency Drug Court (DDC) - Post-File • Early Intervention Family Drug Court (EIFDC) - Pre-File Parent-child parenting intervention Connections to community supports Improved outcomes Sacramento County, CAM Project, Children in Focus (CIF) 100 Treatment Completion Rates 90 80 64.3 70 60 50 53.7 49.2 44 40 30 20 10 0 DDC CIF EIFDC CIF Sacramento County, CAM Project, Children in Focus (CIF) Rate of Positive Court Discharge/Graduate 100 90 80 64.4 70 60 50 50.3 41.8 34 40 30 20 10 DDC 0 CIF EIFDC CIF Sacramento County, CAM Project, Children in Focus (CIF) Remained at Home 100 98 95.1 96 94 92 90 89.9 88 86 84 EIFDC CIF Sacramento County, CAM Project, Children in Focus (CIF) Reunification Rates 97 100 90 87.8 94.9 85.1 80 70 60 53.1 50 40 SAC 30 20 10 0 DDC CIF EIFDC CIF COUNTY Sacramento County, CAM Project, Children in Focus (CIF) No Recurrence of Maltreatment at 12 Months 100 97.9 98 95.7 96 95.6 94 92 90.2 90 88.7 88 SAC 86 84 82 DDC CIF EIFDC CIF COUNTY Sacramento County, CAM Project, Children in Focus (CIF) No Re-Entry at 12 Months 100 100 100 98 96 94 91.8 92 90 89.6 87.7 88 SAC 86 84 82 80 DDC CIF EIFDC CIF COUNTY Improvements in Family Functioning – North Carolina Family Assessment Scale G+R (NCFAS G+R) Overall Domain Items Proportion of Families Rated a Mild/Clear Strength at Intake and Discharge 42.7% Child Well-Being (n=89) 60.7% 43.4% Caregiver/Child Ambivalence* (n=76) 60.5% 31.4% Family Safety (n=86) 55.8% Intake 28.4% Family Interactions (n=88) 51.1% Discharge 18.6% Readiness for Reunification* (n=70) 42.9% 17.6% Parental Capabilities (n=85) 38.8% 12.6% Self-Sufficiency (n=87) 25.3% 0% 10% 20% 30% 40% 50% 60% 70% *For reunification cases only. Caregiver/Child Ambivalence addresses the child’s and caregiver’s desire to reunite and the nature of their relationship with one another. Improvements in Family Functioning – North Carolina Family Assessment Scale G+R (NCFAS G+R) Selected Individual Items Proportion of Families Rated a Mild/Clear Strength at Intake and Discharge 52.3% Child's Relationship with Parent (n=88) 69.3% 45.1% Bonding with Child (n=91) 61.5% 39.3% Communication with Child (n=89) 56.2% 32.8% Parent Understands Child's Needs (n=67) 55.2% 14.9% Child Neglect (n=87) 49.4% 28.1% Disrupted Attachment (n=63) 46.9% 22.5% Supervision of Children (n=89) 46.1% 5.7% Parent Alcohol/Drug Use (n=88) 34.1% 10.8% Resolve CPS Risk Factors (n=74) 33.8% 0% 10% 20% 30% 40% 50% 60% 70% 80% New Ways of Serving Children in Family Drug Courts Lessons Learned and Case Studies from the Children Affected by Methamphetamines Grant Program #5 Develop an Early Identification and Assessment Process FDCs identify participants early in the dependency case process, use screening and assessment to determine the needs and strengths of parents, children and families and identify the most appropriate treatments and other services based on these needs and strengths. Key Component 3: Early identification and immediate placement Screening: Is substance use a factor in the case? • Generally results in a “yes” or “no” • Determines whether a more in-depth assessment is needed • Standardized set of questions to determine the risk or probability of an issue • Brief and easy to administer, orally or written • Can be administered by a broad range of people, including those with little clinical expertise https://www.ncsacw.samhsa.gov/resources/SAFERR.aspx 4 Prong – Screening Tool Signs & symptoms Corroborating reports Drug screen One Yes Proceed to assessment Tool Examples • GAIN-SS (Global Appraisal of Individual Needs Short Screener): Composed of 23 items to be completed by the client or staff and designed to be completed in 5 minutes • UNCOPE: 6-item screen designed to identify alcohol and/or drug substance use and designed to be completed in 2 minutes. • CAGE: 4-item screen designed to identify alcohol and/or drug substance use and designed to be completed in 2 minutes. https://www.ncsacw.samhsa.gov/resources/SAFERR.aspx UNCOPE • 6-item screen • Designed to be completed in 2 minutes and requires less than 1 minute to score • Based on the DSM-IV diagnostic criteria for substance use disorders • Can be administered by the Emergency Response worker or embedded into the standard risk-assessment tool/protocol, etc. • For more information, see www.evinceassessment.com UNCOPE U Have you spent more time drinking /using than intended? (unintended use) N Have you neglected usual responsibilities because of using? Have you ever wanted to cut down on drinking/using? C O P E Has anyone objected to your drinking/use? Have you found yourself thinking a lot about drinking/use? (preoccupied) Have you ever used to relieved emotional distress, such as sadness, anger, or boredom? UNCOPE Substance Sensitivity Specificity Score of 2+ items indicates need for referral for assessment Proportion of individuals (true positives) correctly identified as being positive for substance use disorders Proportion of individuals (true negatives) correctly identified as being negative for substance use disorders Alcohol 91.2% 95.7% Cannabis 91.4% 96.4% Cocaine 96.2% 99.0% 70 PARENTAL AOD AS REASON FOR REMOVAL IN THE US 1998 - 2013 60 50 PERCENT 40 30 U.S. National 20 18.5 10 19.6 21.6 15.8 22.7 23.4 24.9 26.1 26.3 25.8 26.1 28.4 29.3 30.5 31 Great variability across states ranging from <10% to over 60% Source: AFCARS Data, 2013 0 1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 Source: AFCARS Data Files 2013 Signs & Symptoms • Physical • Behavioral • Psychological Corroborating Reports • Police • CWS • Hospital Drug Testing • Drug testing is most frequently used indicator for substance use in CWS practice • Test results may influence decisions on child removal, reunification and Termination of Parental Rights • Courts often order drug testing as a standard protocol for parents in the child welfare system • Lack of standardized recommendations for drug testing in child welfare practice http://www.ncsacw.samhsa.gov/files/DrugTestinginChildWelfare.pdf What Questions Can Drug Testing Answer? …& What Can it Not? • Whether an individual has used a tested substance within a detectable time frame • A drug test alone cannot determine the existence or absence of a substance use disorder • The severity of an individual’s substance use disorder • Whether a child is safe • The parenting capacity and skills of the caregiver Resource: Drug Testing in Child Welfare: Practice and Policy Considerations To download a copy, please visit: http://www.ncsacw.samhsa.gov/files/DrugTestinginChildWelfare.pdf Questions to Consider with a Screening Protocol? • • • • • • • • • • Who is your target population? ‒ Universal or Specific Segment ‒ Screening In vs. Screening Out Does your program address other issues that families are experiencing? What happens with positive screen? How are referrals made for further assessment? How is information communicated with parents? With treatment providers? Are appropriate consents in place and consistently signed? Do providers accept the screening results? What follow-up exists with parents? With treatment providers? Do you screen only when child safety is an issue? Are some “substances” a greater concern than others? What training and support do staff who are conducting the screening need to feel comfortable/confident asking these questions? 4 Prong – Screening Tool Signs & symptoms Corroborating reports Drug screen One Yes Proceed to assessment Assessment: What is the nature and extent of the substance use issue? • Process of information gathering to diagnosis and determine treatment needs • Multidimensional assessment: Standardized set of questions on an individual’s functioning, needs, and strengths to determine the level of care and needed services • Conducted by trained clinicians Diagnosing Substance Use Disorders DSM V Experimental Use NO USE USE/MISUSE MILD MODERATE 2-3 4-5 SEVERE DSM V Criteria (11 total) 6+ Questions to Consider with an Assessment Protocol • • • • • • • • How is the individual referred for assessment? On an average how long does it take to go from referral to assessment? Who conducts the assessment and what tools are used? What additional information from child welfare and other partners would be helpful in understanding the needs of the parent, child and family? How is information communicated to the parent? To the child welfare staff? To the courts? Are the appropriate consents in place and consistently signed? What happens if the parent doesn’t show for assessment? What are the next steps if treatment is indicated? If treatment is not indicated? If the persons/systems/agencies conducting the assessments are not the same as the ones providing treatment, is there a warm hand-off? #6 Address the Needs of Parents FDC partner agencies encourage parents to complete the recovery process and help parents meet treatment goals and child welfare and court requirements. Judges respond to parents in a way that supports continued engagement in recovery. By working toward permanency and using active client engagement, accountability and behavior change strategies, the entire FDC team makes sure that each parent that the FDC serves has access to a broad scope of services. Key Component 2: Using a non-adversarial approach Key Component 4: Access to a continuum of services Key Component 5: Drug testing We know more about The Impact of Recovery Support On Successful Reunification • Recovery Support Specialists • Evidence Based Treatment • Family-Centered Services • Evidence Based Parenting • Parenting Time • Reunification Groups • Ongoing Support “Here’s a referral, let me know when you get into treatment.” “They’ll get into treatment if they really want it.” Missed opportunities “Don’t work harder than the client.” “Call me Tuesday.” Rethinking Treatment Readiness Re-thinking “rock bottom” Addiction as an elevator “Raising the bottom” THE PURPOSE OF RECOVERY SPECIALISTS • Decrease time to assess and enter treatment • Improve outreach and engagement • Increase 12-month permanent placements • Increase family reunification rates • Decrease time in foster care Median Length of Stay in Most Recent Episode of Substance Abuse Treatment after RPG Entry by Grantee Parent Support Strategy Combinations 250 200 200 151 150 100 130 102 50 0 No Parent Support Strategy Intensive Case Management Only Intensive Case Management and Peer/ Parent Mentors Median in Days Intensive Case Management and Recovery Coaches Substance Abuse Treatment Completion Rate by Parent Support Strategies 70% 63% 60% 50% 56% 46% 46% No Parent Support Strategy Intensive Case Management Only 40% 30% 20% 10% 0% Intensive Case Intensive Case Management and Management and Peer/ Parent Mentors Recovery Coaches Median in Days ASAM Definition of Addiction • Addiction is characterized by inability to consistently abstain, impairment in behavioral control, craving, diminished recognition of significant problems with one’s behaviors and interpersonal relationships, and a dysfunctional emotional response • Like other chronic diseases, addiction often involves cycles of relapse and remission • Without treatment or engagement in recovery activities, addiction is progressive and can result in disability or premature death Adopted by the ASAM Board of Directors 4/12/2011 A Chronic, Relapsing Brain Disease • Brain imaging studies show physical changes in areas of the brain that are critical to • Judgment • Decision making • Learning and memory • Behavior control • These changes alter the way the brain works and help explain the compulsion and continued use despite negative consequences Substance Use Disorders are similar to other diseases, such as heart disease. Both diseases disrupt the normal, healthy functioning of the underlying organ, have serious harmful consequences, are preventable, treatable, and if left untreated, can result in premature death. Effects of Drug Use on Dopamine Production • Think of a pleasant experience (a romantic evening, a relaxing vacation, playing with a child). Pleasure is caused by dopamine, a major brain chemical, that is secreted into the amygdala region of the brain causing that pleasure part of the brain to fire. Addictive drugs do the same, only more intense. • When drug use is frequent and causes a surge of dopamine on a regular basis, the brain realizes the dopamine is being provided artificially and it essentially loses its natural ability for pleasure (at least for a period of time). Effects of Drug Use on Dopamine Production • Think about the implications for a child welfare parent who has just stopped using drugs and is trying to resume normal interactions with their child/ren. • If you are tasked with observing this visitation, what conclusions might you draw? • If cues are misread, how might this affect a parent’s ability to keep or obtain custody of their child/ren? • How do we balance compassion, understanding and patience with a parent’s temporarily compromised brain condition while maintaining parent accountability and child safety? A Treatable Disease • Substance use disorders are preventable and are treatable diseases • Discoveries in the science of addiction have led to advances in drug abuse treatment that help people stop abusing drugs and resume their productive lives • Similar to other chronic diseases, addiction can be managed successfully • Treatment enables people to counteract addiction's powerful disruptive effects on brain and behavior and regain areas of life function These images of the dopamine transporter show the brain’s remarkable potential to recover, at least partially, after a long abstinence from drugs - in this case, methamphetamine.9 Addiction and Other Chronic Conditions JAMA, 284:1689-1695, 2000 We know more about Effective Substance Abuse Treatment • Readily available • Attends to multiple needs of the individual (vs. just the substance use) • Engagement strategies to keep clients in treatment • Counseling, behavioral therapies (in combination with medications if necessary) • Co-occurring conditions • Continuous monitoring (National Institute on Drug Abuse, 2012) #7 Address the Needs of Children FDCs must address the physical, developmental, social, emotional and cognitive needs of the children they serve through prevention, intervention and treatment programs. FDCs must implement a holistic and trauma‐informed perspective to ensure that children receive effective, coordinated and appropriate services. Key Component 2: Using a non-adversarial approach Key Component 4: Access to a continuum of services 6.0% AK (N=1,647) AL (N=2,500) AR (N=3,557) AZ (N=8,209) CA (N=45,654) CO (N=17,263) CT (N=12,487) DC (N=917) DE (N=1,754) FL (N=19,014) GA (N=13,211) HI (N=1,383) IA (N=7,663) ID (N=1,878) IL (N=9,163) IN (N=7,724) KS (N=3,699) KY (N=5,923) LA (N=4,086) MA (N= 22,698) MD (N=16,831) ME (N=4,532) MI (16,471) MN (N=13,874) MS (N/A) MO (N=12,012) MT (N=2,090) NC (N=12,660) ND (N=791) NE (N=4,268) NH (N=1,296) NJ (N=11,896) NM (N=333) NV (N=2,455) NY (N=42,004) OH (N=19,164) OK (N=4,851) OR (N=13,245) PA (N/A) RI (N=2,230) SC (N=5,796) SD (N=3,303) TN (N=3,855) TX (N=13,676) UT (N=3,742) VT (N=2,609) VA (6,729) WA (N=10,438) WV (N/A) WI (N=5,702) WY (N=1,366) PR (N=218) PERCENT OF WOMEN OF CHILDBEARING AGE (AGES 15-44), PREGNANT AT TIME OF TREATMENT ADMISSION, 2012 18.0% 16.0% 14.0% 12.0% N=428,867 10.0% 8.0% 5.9% 4.0% 2.0% 0.0% N = Total Number of Women of Childbearing Age (Age 15-44) Entering Treatment Source: TEDS Data, 2012 Family–Centered Approach Recognizes that addiction is a family disease and that recovery and well-being occurs in the context of families TREATMENT RETENTION AND COMPLETION 1. Women who participated in programs that included a “high” level of family and children’s services and employment/education services were twice as likely to reunify with their children as those who participated in programs with a “low” level of these services. (Grella, Hser & Yang, 2006) 2. Retention and completion of treatment have been found to be the strongest predictors of reunification with children for substanceabusing parents. (Green, Rockhill, & Furrer, 2007; Marsh, Smith, & Bruni, 2010) 3. Substance abuse treatment services that include children in treatment can lead to improved outcomes for the parent, which can also improve outcomes for the child. Focusing Only on Parent’s Recovery Without Addressing Needs of Children Can threaten parent’s ability to achieve and sustain recovery and establish a healthy relationship with their children, thus risking: • Recurrence of maltreatment • Re-entry into out-of-home care • Relapse and sustained sobriety • Additional substance-exposed infants • Additional exposure to trauma for child/family • Prolonged and recurring impact on child well-being Challenges for the Parents • The parent lacks understanding of and the ability to cope with the child’s medical, developmental, behavioral, and emotional needs • The child’s physical, developmental needs were not assessed, or the child did not receive appropriate interventions/treatment services for the identified needs • The parent and child did not receive services that addressed trauma (for both of them) and relationship issues Selection of an Evidence-Based Parenting Program • Review publicly available information • Need to have a structure for comparing programs • Pairing the curriculum to your FDC needs and realities • Understand the outcomes you’d like to see, and be able to articulate them and link them to the program of choice Considerations When Selecting a Parenting Program • • • • Understand the needs of Court consumers - What do these families look like? Are there unique struggles? Have realistic expectations of their ability to participate - especially in early recovery Parenting program should include parent-child interactive time, but this should not be considered visitation Child development information needs to be shared with the parent and the parenting facilitator in advance Drug Courts That Offer Parenting Classes Had 68% Greater Reductions in Recidivism and 52% Greater Cost Savings % Reduction in Recidivism 38% 23% PROGRAM PROVIDES PARENTING CLASSES N=44 True in adult, family, juvenile PROGRAM DOES NOT PROVIDE PARENTING CLASSES N=17 Children Need to Spend Time with Their Parents • Involve parents in the child’s appointments with doctors and therapists • Expect foster parents to participate in visits • Help parents plan visits ahead of time • Enlist natural community settings as visitation locations (e.g. family resource centers) • Limit the child’s exposure to adults with whom they have a comfortable relationship Elements of Successful Visitation Plans Parenting time should occur: • Frequently • For an appropriate period of time • In a comfortable and safe setting • With therapeutic supervision Impact of Parenting time on Reunification Outcomes • Children and youth who have regular, frequent contact with their families are more likely to reunify and less likely to reenter foster care after reunification (Mallon, 2011) • Visits provide an important opportunity to gather information about a parent’s capacity to appropriately address and provide for their child’s needs, as well as the family’s overall readiness for reunification • Parent-Child Contact (Visitation): Research shows frequent visitation increases the likelihood of reunification, reduces time in out-of-home care (Hess, 2003), and promotes healthy attachment and reduces negative effects of separation (Dougherty, 2004) Support Strategy — Reunification Group • Begin during unsupervised/overnight visitations through 3 months post reunification • Staffed by an outside treatment provider and recovery support specialist (or other mentor role) • Focus on supporting parents through reunification process • Group process provides guidance and encouragement; opportunity to express concerns about parenting without repercussion Aftercare and Ongoing Support • Ensure aftercare and recovery success beyond FDC and CWS participation: ‒ Personal Recovery Plan – relapse prevention, relapse ‒ Peer-to-peer – alumni groups, recovery groups ‒ Other relationships – family, friends, caregivers, significant others ‒ Community-based support and services – basic needs (childcare, housing, transportation), mental health, physical health and medical care, spiritual support ‒ Self-sufficiency – employment, educational and training opportunities Rethinking Readiness How will we know? Effective FDCs focus on behavioral benchmarks Essential Elements of Responses to Behavior • Addiction is a brain disorder • Length of time in treatment is the key; the longer we keep someone in treatment, the greater probability of a successful outcome • Purpose of sanctions and incentives is to keep participants engaged and motivated in treatment Safe vs. Perfect Stigma & Perceptions Addiction • Once an addict, always an addict • They don’t really want to change • They lie • They must love their drug more than their child • They need to get to rock bottom, before… Collaborative Value Inventory (CVI) What Do We Believe About Alcohol and Other Drugs, Services to Children and Families, and Dependency Courts? • Anonymous web-based survey to be completed by cross-disciplinary teams of professionals • Increase the understanding of the values that guide different disciplines and systems • To assist community members and professional staff in developing common principles for their work together PEOPLE WHO ARE CHEMICALLY DEPENDENT HAVE A DISEASE FOR WHICH THEY NEED TREATMENT 84.4 90 Percent 80 70 60 50 40 15.6 30 20 0.0 10 0.0 0 Strongly Agree Somewhat Agree Somewhat Disagree Strongly Disagree n = 90 Percent IN ASSESSING THE EFFECTS OF THE USE OF ALCOHOL AND OTHER DRUGS, THE STANDARD WE SHOULD USE FOR DECIDING WHEN TO REMOVE OR REUNIFY CHILDREN WITH THEIR PARENTS IS WHETHER THE PARENTS ARE FULLY ABSTAINING FROM THE USE OF ALCOHOL OR OTHER DRUGS 41.1 50 32.2 40 30 15.6 11.1 20 10 0 Strongly Agree Somewhat Agree Somewhat Disagree Strongly Disagree n = 90 Reasonable Efforts to Preserve and Reunify Families • Were services to the family accessible, available, and appropriate? • Were the services specifically relevant to the family's problems and needs? • Were the appropriate services available to the family on a timely basis? Critical Questions • When the parents complete all of the steps on the case plan, will you be comfortable allowing the children to go home? • Is there any step in the case plan that, if not completed, will keep you from allowing the child to go home? Monitoring – What Has Been the Impact? • Staff – what is feedback regarding implementation? What barriers exist? • Referral and treatment access and quality • Outcome monitoring – what is impact key indicators? • Information sharing – how is it collected, shared, and reported? Defining Your Drop off Points (Example) 6,071 Substantiated Cases of neglect and/or abuse due to substance use disorders (60% SUD Avg) Potential participants assessed for treatment (Tx) 25% drop off = 4,553 Number of participants deemed appropriate 50% = 2,276 Number admitted to Tx= 1,593 30% drop off • Substantiated cases pulled from Louisiana AFCARS data files • Drop off percentages estimated based on previous drop off reports • To be used only as an example 638 successfully completed Tx - 60% drop off Payoff 77 We can no longer say “We don’t know what to do.” Building on our Success Q&A and Discussion Resources Join Us! Family Drug Court Learning Academy 2016 Virtual Watch Pre-Recorded Webinar Classroom Series Register and Join Live Virtual Classroom Convenient & Effective Learning Virtual Classroom Webinar Available Classroom Schedule Screening & Assessment Governance & Leadership Parent-Child Relationships Data & Info Systems April 1 April 14, May 12, May 26 April 5 April 19, May 3, May 17 July 1 July 14, July 28, August 18 July 5 July 21, August 11, August 25 • Real-time networking and knowledge sharing • Coaching & mentoring • Applied learning through homework or project assignments • 24/7 access to classroom • Technical assistance and resources Register Now! Space Limited FDC Learning Academy Blog • • • • • Webinar Recordings FDC Resources FDC Video features FDC Podcasts & Interviews Virtual Classroom registration www.familydrugcourts.blogspot.com FDC Guidelines To download a copy today visit our website: http://www.cffutures.org/files/publications/FDC-Guidelines.pdf August 1-3, 2016 | Hyatt Regency | Orange County, California 2015 Special Issue Includes four Family Drug Court specific articles presenting findings on: • Findings from the Children Affected by Methamphetamine (CAM) FDC grant program • FDC program compliance and child welfare outcomes • Changes in adult, child and family functioning amongst FDC participants • Issues pertaining to rural FDCs www.cwla.org Family Drug Court Online Tutorial FDC 101 – Will cover basic knowledge of the FDC model and operations King County, WA Wapello County, IA Jackson County, MO Baltimore City, MD Dunklin County, MO Jefferson County, AL Pima County, AZ Chatham County, GA Miami-Dade, FL FAMILY DRUG COURT PEER LEARNING COURT PROGRAM CONTACT US FOR MORE INFORMATION: [email protected] Resources FDC Discipline Specific Orientation Materials Child Welfare | AOD Treatment | Judges | Attorneys Please visit: www.cffutures.org/fdc/ Resources NCSACW Online Tutorials • Understanding Substance Abuse and Facilitating Recovery: A Guide for Child Welfare Workers • Understanding Child Welfare and the Dependency Court: A Guide for Substance Abuse Treatment Professionals • Understanding Substance Use Disorders, Treatment and Family Recovery: A Guide for Legal Professionals Please visit: http://www.ncsacw.samhsa.gov/ Contact Information Strengthening Partnerships Improving Family Outcomes Phil Breitenbucher, MSW FDC Program Director Children and Family Futures (714) 505-3525 [email protected] Alexis Balkey, BA, RAS FDC Program Manager Children and Family Futures (714) 505-3525 [email protected]