Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
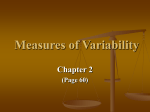
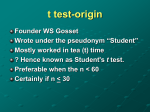
AJH 2002; 15:125–129 Effects of Alcohol Restriction on Ambulatory Blood Pressure, Heart Rate, and Heart Rate Variability in Japanese Men Junichi Minami, Masayoshi Yoshii, Masakatsu Todoroki, Toshio Nishikimi, Toshihiko Ishimitsu, Tatsushige Fukunaga, and Hiroaki Matsuoka We investigated the effects of alcohol restriction on ambulatory blood pressure (BP), heart rate, and heart rate variability in 33 Japanese male volunteers (37 ⫾ 1 years, mean ⫾ SE), who were all habitual drinkers. Subjects were told either to keep their usual drinking habits for 3 weeks (usual alcohol period), or to reduce alcohol intake by at least half of their usual drinking amount (reduced alcohol period). The ambulatory BP, heart rate, and electrocardiographic R-R intervals were measured during a 24-h period with a portable recorder on the last day of each period. A power spectral analysis of R-R intervals was performed to obtain the low-frequency (LF) and highfrequency (HF) components. The percentage of differences between adjacent normal R-R intervals ⬎50 msec (pNN50) was also calculated. The amount of ethanol intake was significantly reduced from 70 ⫾ 5 mL/day in the usual alcohol period to 19 ⫾ 3 mL/day in the reduced alcohol period (P ⬍ .0001). The daytime systolic BP was T he relationship between high alcohol intake (typically three or more drinks per day) and elevated blood pressure (BP) has been reported in a large number of observational studies.1,2 A few trials have also demonstrated that reductions in alcohol intake among heavy drinkers can lower BP in normotensive and hypertensive men.3,4 On the basis of these findings, principal guidelines on the treatment of hypertension support a recommendation to limit alcohol intake to no more than two drinks per day (men) and one drink per day (women) among those who drink.5,6 So far, several studies have documented an association between reduced heart rate variability and risk for cardiac events.7,8 Although a few investigators have reported that acute alcohol intake influenced heart rate variability in healthy subjects9,10 and patients with cardiovascular disReceived June 22, 2001. Accepted September 13, 2001. From the Department of Hypertension and Cardiorenal Medicine (JM, MY, MT, TN, TI, HM), Dokkyo University School of Medicine, Mibu, Tochigi; and Department of Forensic Medicine and Sciences (TF), © 2002 by the American Journal of Hypertension, Ltd. Published by Elsevier Science Inc. significantly lower in the reduced alcohol period than in the usual alcohol period by 4 ⫾ 1 mm Hg (P ⬍ .05). The daytime and nighttime heart rate was significantly lower in the reduced alcohol period than in the usual alcohol (P ⬍ .001 for each). The pNN50 and the HF component were significantly higher in the reduced alcohol period than in the usual alcohol period (P ⬍ .0001 for each). The LF/HF ratio was significantly lower in the reduced period than in the usual period (P ⬍ .01). These results demonstrate that 3-week alcohol restriction produced reductions in ambulatory systolic BP, heart rate, and the index of sympathovagal balance, and augmentations of parasympathetic indices of heart rate variability in Japanese male drinkers. Am J Hypertens 2002;15:125–129 © 2002 American Journal of Hypertension, Ltd. Key Words: Alcohol restriction, ambulatory blood pressure, heart rate, heart rate variability, hypertension. eases,11,12 little is known about the chronic effect of alcohol restriction on heart rate variability in habitual drinkers. In this study, we investigated the effects of 3-week alcohol restriction on ambulatory BP, heart rate, and time- and frequency-domain measures of heart rate variability in Japanese men who were habitual drinkers. Methods A total of 33 Japanese male volunteers were included in the present study. The mean age (⫾ SE) was 36.9 ⫾ 1.1 years and the mean body mass index was 25.0 ⫾ 0.5 kg/m2. Information about drinking habits was obtained using a questionnaire, with an inclusion criterion of ⱖ30 mL/day ethanol consumption. Beer was the most common alcoholic beverage consumed, followed by sake. Other Mie University School of Medicine, Mie, Japan. Address correspondence and reprint requests to Dr. Junichi Minami, Department of Hypertension and Cardiorenal Medicine, Dokkyo University School of Medicine, Mibu, Tochigi 321-0293, Japan; e-mail: [email protected] 0895-7061/02/$22.00 PII S0895-7061(01)02265-8 126 ALCOHOL AND BLOOD PRESSURE AND HEART RATE VARIABILITY alcohol consumed included wine, whiskey, and other spirits. All of the subjects consumed alcohol in the evening, and none drank in the morning or afternoon. No subjects were receiving pharmacologic therapy. All subjects agreed to participate after receiving a detailed explanation of the nature and purpose of the study, and all subjects gave written informed consent. The study protocol was in accordance with the Declaration of Helsinki (Somerset West version, 1996) of the World Medical Association and was approved by the Institutional Review Board of our institute. Using a randomized crossover design, subjects were instructed to either maintain their usual drinking habits for 3 weeks, or to reduce alcohol intake by at least half of their usual drinking amount. Seventeen subjects were assigned first to the usual alcohol period and the other 16 subjects were assigned to the reduced alcohol period. Daily alcohol consumption was recorded by each subject throughout the study. Venous blood samples were obtained on the last day of each period. Serum ␥-glutamyl transpeptidase (GTP) was determined with an autoanalyzer, Hitachi 7170 (Hitachi Ltd. Instruments, Tokyo, Japan). The ambulatory BP was monitored every 30 min by a cuff oscillometric device, TM-2425 (A&D Co., Tokyo, Japan)13 on the last day of each period. The subjects were asked to carry the device for 26 h, and the first 2 h of recordings made at or near the hospital were omitted from the later analysis. The ambulatory monitoring was performed during an average working day. The daytime and the nighttime BP were calculated according to the true waking and sleeping times of the individual subjects. The same recorder was used for each subject for the entire protocol to avoid different BP readings obtained by different recorders. The ambulatory BP recorder used in this study also monitored the R-R interval of the electrocardiogram. The procedures of the power spectral analysis of R-R intervals in this device were previously reported in detail.14,15 Spectral R-R variability was computed as the LF component (0.05 to 0.15 Hz) and HF component (0.15 to 0.40 Hz) using the autoregressive model from every 5-min block during a 24-h period. The LF/HF ratio was calculated as an index of sympathovagal balance.16 We also calculated the time-domain index, pNN50, which is the percentage of differences between adjacent normal R-R intervals ⬎50 msec. The pNN50 is a useful marker of parasympathetic nerve activity.7 Heart rate was calculated on the basis of continuous electrocardiographic recordings. Values are expressed as means ⫾ SE. Comparisons between the usual alcohol and reduced alcohol periods were made using Student paired t test or one-way repeated measures ANOVA as appropriate. Newman-Keul’s tests were used as determined by the ANOVA results. For the comparisons of power spectral data, the naturally logarithmic values, ln (the LF component), ln (the HF component), or ln (the LF/HF ratio), were used to normalize the skewness of the data. Significance was determined as P ⬍ .05. AJH–February 2002–VOL. 15, NO. 2, PART 1 FIG. 1. The 24-h trendgram of blood pressure (BP) and heart rate during the usual alcohol (●) and reduced alcohol (䡩) periods. The daytime systolic BP was significantly lower in the reduced alcohol period than in the usual alcohol period, whereas the nighttime diastolic BP was insignificantly higher in the reduced alcohol period than in the usual period. The daytime and nighttime heart rate values were significantly lower in the reduced alcohol period than in the usual alcohol period. Results All subjects completed the study protocol. The amount of ethanol intake was significantly reduced from 70.1 ⫾ 4.6 mL/day in the usual alcohol period to 19.1 ⫾ 2.5 mL/day in the reduced alcohol period (P ⬍ .0001). Serum ␥-GTP was significantly lower in the reduced alcohol period than in the usual alcohol period (54.2 ⫾ 4.7 U/L v 62.7 ⫾ 6.0 U/L, P ⬍ .01). The subject’s body weight did not differ significantly between the two periods. Fig. 1 depicts the 24-h trendgram of BP and heart rate in each period. Table 1 lists the average values of BP and heart rate for the entire 24-h period, daytime and nighttime. The 24-h and the daytime systolic BP were significantly lower in the reduced alcohol period than in the AJH–February 2002–VOL. 15, NO. 2, PART 1 ALCOHOL AND BLOOD PRESSURE AND HEART RATE VARIABILITY 127 Table 1. Ambulatory blood pressure and heart rate during the usual alcohol and reduced alcohol periods Usual Alcohol Period Reduced Alcohol Period P 24-h Systolic BP (mm Hg) 128.2 ⫾ 1.8 125.0 ⫾ 1.9 ⬍.05 Diastolic BP (mm Hg) 78.5 ⫾ 1.1 78.2 ⫾ 1.1 NS Heart Rate (beats/min) 82.7 ⫾ 1.7 77.4 ⫾ 1.9 ⬍.0001 Daytime Systolic BP (mm Hg) 135.8 ⫾ 2.0 132.4 ⫾ 2.1 ⬍.05 Diastolic BP (mm Hg) 84.8 ⫾ 1.3 83.7 ⫾ 1.2 NS Heart Rate (beats/min) 88.1 ⫾ 1.8 83.9 ⫾ 2.1 ⬍.001 Nighttime Systolic BP (mm Hg) 112.3 ⫾ 1.9 110.4 ⫾ 1.8 NS Diastolic BP (mm Hg) 65.1 ⫾ 1.0 67.2 ⫾ 1.2 .05 Heart Rate (beats/min) 70.7 ⫾ 1.7 63.6 ⫾ 1.8 ⬍.001 BP ⫽ blood pressure; NS ⫽ not significant. Values are expressed as means ⫾ SE. usual alcohol period by 3.2 ⫾ 1.2 mm Hg (P ⬍ .05) and 3.5 ⫾ 1.4 mm Hg (P ⬍ .05), respectively, whereas the nighttime systolic BP did not differ significantly between the two periods. The 24-h and the daytime diastolic BP did not differ significantly between the two periods, whereas the nighttime diastolic BP was insignificantly lower in the usual alcohol period than in the reduced alcohol period by 2.1⫾ 1.3 mm Hg (P ⫽ .05). With regard to the heart rate, not only the daytime heart rate, but also the nighttime heart rate was significantly lower in the reduced alcohol period than in the usual alcohol period by 4.1 ⫾ 0.9 beats/min (P ⬍ .001) and by 7.1 ⫾ 1.1 beats/min (P ⬍ .001), respectively. The difference in the 24-h heart rate between the two periods was 5.2 ⫾ 0.9 beats/min (P ⬍ .0001). The number of total heart beats during 24 h was 119,030 ⫾ 2511 in the usual alcohol period and 111,508 ⫾ 2797 in the reduced alcohol period (P ⬍ .0001). Fig. 2 shows the 24-h trendgram of the LF component, the HF component, and the LF/HF ratio in each period. Table 2 lists the average values of the pNN50, the LF component, the HF component, and the LF/HF ratio for the entire 24-h period, daytime and nighttime. Both the pNN50 and the HF component were significantly higher in the reduced alcohol period than in the usual alcohol period in both the daytime and nighttime, indicating that the alcohol restriction augmented the parasympathetic nerve activity throughout a 24-h period in these subjects. The LF/HF ratio was significantly lower in the reduced period FIG. 2. The 24-h trendgram of the low-frequency (LF) component, the high-frequency (HF) component, and the LF/HF ratio during the usual alcohol (●) and reduced alcohol (䡩) periods. Both the LF and HF components were significantly higher in the reduced alcohol period than in the usual alcohol period in both the daytime and nighttime. The daytime LF/HF ratio was significantly lower in the reduced alcohol period than in the usual alcohol period in both the daytime and nighttime. than in the usual period in both the daytime and nighttime values. Discussion A large number of cross-sectional epidemiologic studies have shown a clear relationship between alcohol consumption, high BP, and the prevalence of hypertension.1,2 Intervention studies have also shown that the cessation of alcohol drinking reduces office BP in normotensive and 128 ALCOHOL AND BLOOD PRESSURE AND HEART RATE VARIABILITY 6.5 5.02 4.00 1.02 ⫾ ⫾ ⫾ ⫾ 1.1 0.14 0.15 0.09 4.6 5.01 3.69 1.32 ⫾ ⫾ ⫾ ⫾ 0.9 7.4 ⫾ 1.2 0.15 5.25 ⫾ 0.15 0.15 4.08 ⫾ 0.17 0.08 1.17 ⫾ 0.09 ⬍.05 ⬍.01 ⬍.001 ⬍.01 3-week alcohol restriction significantly increased the indices of parasympathetic nerve activity and decreased the index of sympathovagal balance throughout a 24-h period in habitual drinkers, suggesting that the disadvantageous effects of alcohol intake on autonomic nerve activity continue after its elimination and that the effects are sustained. In conclusion, 3-week alcohol restriction produced reductions in ambulatory systolic BP, heart rate, and the index of sympathovagal balance, and augmentations of parasympathetic indices of heart rate variability in Japanese male drinkers. Restriction of alcohol intake among moderate-to-heavy drinkers is recommended, specifically from the point of view of an improvement in the autonomic nervous function. 12.1 5.05 4.67 0.37 ⫾ ⫾ ⫾ ⫾ 1.8 0.15 0.19 0.11 ⬍.001 ⬍.001 ⬍.001 ⬍.001 References Table 2. Indices of heart rate variability during the usual alcohol and reduced alcohol periods Usual Alcohol Period 24-h pNN50 (%) LF, ln (msec2) HF, ln (msec2) ln (LF/HF) Daytime pNN50 (%) LF, ln (msec2) HF, ln (msec2) ln (LF/HF) Nighttime pNN50 (%) LF, ln (msec2) HF, ln (msec2) ln (LF/HF) AJH–February 2002–VOL. 15, NO. 2, PART 1 Reduced Alcohol Period 11.1 5.32 4.50 0.82 21.4 5.47 5.40 0.07 ⫾ ⫾ ⫾ ⫾ ⫾ ⫾ ⫾ ⫾ 1.5 0.14 0.16 0.10 2.7 0.17 0.18 0.13 P ⬍.0001 ⬍.001 ⬍.0001 ⬍.01 pNN50 ⫽ the percentage of differences between adjacent normal R-R intervals ⬎50 msec; LF ⫽ low-frequency component; HF ⫽ high-frequency component. Values are expressed as means ⫾ SE. hypertensive men.3,4 However, attempts to reproduce these findings by ambulatory BP monitoring have shown inconsistent results. Recently, Kawano et al17 reported that the restriction of alcohol intake for 4 weeks lowered daytime systolic BP but increased systolic and diastolic nighttime BP without affecting the average 24-h systolic and diastolic BP in Japanese men with hypertension. However, Aguilera et al18 reported that 1-month alcohol abstinence in 42 heavy drinkers significantly decreased systolic and diastolic BP without affecting its circadian pattern. In the present study, the restriction of alcohol intake for 3 weeks significantly lowered the 24-h and daytime systolic BP, but slightly increased the nighttime diastolic BP in Japanese male drinkers. The disparity in these results including ours may be in part explained by differences in study protocol and the subject’s baseline characteristics. Further studies are needed to obtain conclusive information on the chronic effect of alcohol restriction on ambulatory BP in habitual drinkers. In the present study, more marked effects of alcohol restriction were observed on heart rate and time and frequency domain measures of heart rate variability. To date, there have been some reports that acute alcohol intake significantly changed measures of heart rate variability in healthy subjects,9,10 patients with coronary heart disease,11 and patients with a history of alcohol-induced atrial fibrillation.12 However, little is known about the chronic effect of alcohol restriction on heart rate variability in habitual drinkers. To the best of our knowledge, this is the first study in which the chronic effects of alcohol restriction on several measures of heart rate variability were examined during 24 h by intervention and a randomized trial in the same individuals. In the present study, we found that 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. 12. 13. MacMahon S: Alcohol consumption and hypertension. Hypertension 1987;9:111–121. Klatsky AL, Armstrong MA, Friedman GD: Risk of cardiovascular mortality in alcohol drinkers, ex-drinkers and nondrinkers. Am J Cardiol 1990;66:1237–1242. Puddey IB, Beilin LJ, Vandongen R, Rouse IL, Rogers P: Evidence for a direct effect of alcohol consumption on blood pressure in normotensive men: a randomized controlled trial. Hypertension 1985;7:707–713. Puddey IB, Beilin LJ, Vandongen R: Regular alcohol use raises blood pressure in treated hypertensive subjects: a randomised controlled trial. Lancet 1987;1:647–651. Joint National Committee: The sixth report of the Joint National Committee on prevention, detection, evaluation, and treatment of high blood pressure. Arch Intern Med 1997;157:2413–2446. World Health Organization-International Society of Hypertension: 1999 World Health Organization–International Society of Hypertension Guidelines for the Management of Hypertension: Guidelines Subcommittee. J Hypertens 1999;17:151–183. Task Force of the European Society of Cardiology the North American Society of Pacing Electrophysiology: Heart rate variability: standards of measurement, physiological interpretation, and clinical use. Circulation 1996;93:1043–1065. Tsuji H, Larson MG, Venditti FJ, Manders ES, Evans JC, Feldman CL, Levy D: Impact of reduced heart rate variability on risk for cardiac events: the Framingham heart study. Circulation 1996;94: 2850 –2855. Koskinen P, Virolainen J, Kupari M: Acute alcohol intake decreases short-term heart rate variability in healthy subjects. Clin Sci (Colch) 1994;87:225–230. van de Borne P, Mark AL, Montano N, Mion D, Somers VK: Effects of alcohol on sympathetic activity, hemodynamics, and chemoreflex sensitivity. Hypertension 1997;29:1278 –1283. Rossinen J, Viitasalo M, Partanen J, Koskinen P, Kupari M, Nieminen MS: Effects of acute alcohol ingestion on heart rate variability in patients with documented coronary artery disease and stable angina pectoris. Am J Cardiol 1997;79:487–491. Maki T, Toivonen L, Koskinen P, Naveri H, Harkonen M, Leinonen H: Effect of ethanol drinking, hangover, and exercise on adrenergic activity and heart rate variability in patients with a history of alcohol-induced atrial fibrillation. Am J Cardiol 1998;82:317–322. Tochikubo O, Ikeda A, Miyajima E, Ishii M: Effects of insufficient sleep on blood pressure monitored by a new multibiomedical recorder. Hypertension 1996;27:1318 –1324. AJH–February 2002–VOL. 15, NO. 2, PART 1 ALCOHOL AND BLOOD PRESSURE AND HEART RATE VARIABILITY 14. Minami J, Kawano Y, Ishimitsu T, Takishita S: Blunted parasympathetic modulation in salt-sensitive patients with essential hypertension: evaluation by power-spectral analysis of heart-rate variability. J Hypertens 1997;15:727–735. 15. Minami J, Ishimitsu T, Matsuoka H: Effects of smoking cessation on blood pressure and heart rate variability in habitual smokers. Hypertension 1999;33:586 –590. 16. Pagani M, Lombardi F, Guzzetti S, Rimoldi O, Furlan R, Pizzinelli P, Sandrone G, Malfatto G Dell’, Orto S, Piccaluga E, Turiel M, Baselli G, Cerutti S, Malliani A: Power spectral 129 analysis of heart rate and arterial pressure variabilities as a marker of sympatho-vagal interaction in man and conscious dog. Circ Res 1986;59:178 –193. 17. Kawano Y, Abe H, Takishita S, Omae T: Effects of alcohol restriction on 24-hour ambulatory blood pressure in Japanese men with hypertension. Am J Med 1998;105:307–311. 18. Aguilera MT, de la Sierra A, Coca A, Estruch R, Fernandez-Sola J, Urbano-Marquez A: Effect of alcohol abstinence on blood pressure: assessment by 24-hour ambulatory blood pressure monitoring. Hypertension 1999;33:653–657.