Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
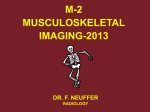
n Case Report Alkaptonuric Ochronosis Mukand Lal, MBBS, MS; Manoj Thakur, MBBS, MS, DNB; Sandeep Kashyap, MBBS, MS abstract Full article available online at Healio.com/Orthopedics Alkaptonuria, with its sequel, ochronosis, is a rare disease, with an incidence of 1:125,000 to 1:1 million worldwide. Reported cases of ochronotic arthropathy and other orthopedic manifestations are mostly limited to a single family tree, and few cases have been reported. This study highlights 9 previously unreported patients with sporadic presentation and varied orthopedic manifestations of alkaptonuria. Patient age ranged from 34 to 50 years. One patient who had severe arthropathy of the right hip joint along with subcutaneous nodules over both knees and Achilles tendons underwent total hip replacement. Another patient had intramedullary calcification of the femur. An additional patient had associated caries of the spine at L3, L4, and L5, with resolution of symptoms after antitubercular chemotherapy. Another patient had associated features of hyperthyroidism, which was an incidental finding. A further patient had nonunion fracture of the neck of the femur and underwent total hip replacement. The remaining 4 patients had typical features of low backache and arthritis of the large joints. The parents were nonconsanguineous, and only 2 patients had affected siblings. The remaining 7 patients had sporadic nonfamilial presentation. Diagnosis was established by typical clinical and radiologic findings and biochemical analysis. At 2 years of follow-up, both patients who underwent total hip replacement were normal, with no radiologic signs of loosening or lysis. Clinicians need a high index of suspicion and awareness to make the diagnosis of ochronosis. The current study is unique because of presentation with subcutaneous nodules in 1 patient and associated caries of the spine in another patient. [Orthopedics. 2014; 37(12):e1141-e1149.] Figure: Anteroposterior radiograph showing fracture nonunion of the neck of the femur 1 year postoperatively. The authors are from the Department of Orthopaedics, Indira Gandhi Medical College, Shimla, India. The authors have no relevant financial relationships to disclose. Correspondence should be addressed to: Sandeep Kashyap, MBBS, MS, Department of Orthopaedics, Indira Gandhi Medical College, Prakash Niwas, Near Chitkara Park, Shimla 171003, India ([email protected]). Received: May 23, 2013; Accepted: April 9, 2014; Posted: December 10, 2014. doi: 10.3928/01477447-20141123-94 DECEMBER 2014 | Volume 37 • Number 12 e1141 n Case Report A lkaptonuria is a rare inherited autosomal recessive metabolic disorder caused by deficiency of homogentisic acid oxidase (homogentisic acid 1, 2 dioxygenase) enzyme.1 The enzyme homogentisic acid oxidase is absent in the liver and kidneys. Consequently, homogentisic acid is excreted in urine and the urine turns dark brown or black on oxygenation and alkalinization.2 This condition is characterized by a triad of manifestations, including homogentisic acid in the urine (alkaptonuria), ochronosis characterized by deposition of homogentisic acid in connective tissue and cartilage, and spondyloarthropathy involving the axial and appendicular skeleton (ie, arthritis of the spine and large joints).1 Less common manifestations include renal, urethral, and prostatic calculi; cardiovascular abnormalities; and valvular disease.3-5 Alkaptonuria was one of the first conditions in which the law of mendelian recessive inheritance was proposed as well as 1 of the conditions in the charter of the group of inborn errors of metabolism. The term ochronosis was first coined by Virchow6 in 1866, when he found pigmentation of tissues that appeared ochre, meaning yellow, when examined microscopically.7 This disorder is rare, with an incidence of 1:125,000 to 1:1 million worldwide.1,4,8,9 However, in certain areas of eastern Europe, chiefly Slovakia, and the Dominican Republic, the incidence is as high as 1:19,000.10 The authors report 9 cases of patients who had alkaptonuria with ochronosis. Most previous studies of alkaptonuria were limited to patients from a single family tree or a few case reports. This study highlights nonfamilial, sporadic presentation and atypical manifestations of alkaptonuria that were not reported before. Patients were informed that data about their cases would be submitted for publication, and they consented. Cases All patients were 34 to 50 years old. Eight patients had a history since child- e1142 B Figure 1: Preoperative anterior photograph showing subcutaneous nodules over the Achilles tendon (A). Preoperative lateral photograph showing subcutaneous nodules over the knees (B). A hood of brownish-black stains of the undergarments and a change in urine color to black when it was left standing for few hours. One patient had a varied presentation that included a history of brownishblack discoloration of the initial 2 to 3 drops of urine for the past 3 years. This manifestation occurred at 47 years of age, which is unusual, and the patient had fracture nonunion of the neck of the femur at 50 years of age, although he underwent closed reduction and internal fixation within 48 hours of injury. He subsequently underwent total hip replacement. Another patient had collapse of the head of the femur with osteoarthritis of the hip joint along with subcutaneous nodules. This patient also underwent total hip replacement. One patient had intramedullary calcification of the femur. Associated caries of the spine was found in 1 patient at L4 and L5 and was managed conservatively with rest and antituberculous chemotherapy. One woman had an incidental finding of associated features of hyperthyroidism. Seven patients initially presented with backache. This group of patients included a brother and sister, although their parents and siblings were normal. Findings on systemic examination of the cardiovascular system, respiratory system, and abdomen were normal in all patients. Findings on neurologic examination were normal, except for 1 patient who had caries of the spine. On local examination, results of Schober’s test were positive in all patients. Initial screening was done by adding alkali (sodium hydroxide) to the urine sample: the color changed to reddish-brown (Figure 1). Similarly, addition of ferric chloride and silver nitrate to the urine sample gave the urine a transient green and black color, respectively, in all 9 patients. Confirmation was done by liquid gas chromatography, and findings were positive in all patients. Findings of other studies, such as electrocardiogram, chest radiograph, and echocardiogram, were normal in all patients. Similarly, results of tests for C-reactive protein, rheumatoid factor, and HLA-B27 were negative. Serum levels of magnesium, calcium, parathyroid hormone, 25-OH vitamin D, vitamin B12, folic acid, and ferritin were within normal levels. Results of all other routine studies were within normal limits. The presenting features, symptoms, and clinical profiles of all of these patients are shown in Table 1. Table 2 shows the test results, radiologic findings, and treatment. Discussion Alkaptonuria, along with its sequela, ochronosis, is a rare disease of aromatic amino acid metabolism. The earliest case was described in an Egyptian mummy, ORTHOPEDICS | Healio.com/Orthopedics n Case Report Harwa dating from 1500 b.c.11,12 The term alkapton was first used by Boedeker13 in 1859 to describe urine discoloration caused by a reducing compound that was identified as homogentisic acid by Wolkow and Baumann14 1891. In his Croonian lectures of 1908, Garrod15 coined the term inborn error of metabolism and proposed that alkaptonuria results from a deficiency of an enzyme that normally splits the aromatic ring of homogentisic acid. The deficient enzyme was identified by La Du16 in 1958. Pollak et al17 located the alkaptonuric gene to 3q2 in a 16-cM region. Joint disease in alkaptonuria was initially reported by Albrecht,18 and later Osler19 clinically diagnosed ochronosis for the first time in 2 brothers with alkaptonuria. A worldwide review showed that approximately 600 cases have been reported since 1962.20 Accumulation of homogentisic acid in various tissues leads to polymerization to an oxidized product, benzoquinone, that causes tissue injury that leads to melaninlike polymers.21 Several theories exist as to how alkaptonuria results in ochronosis, including acting as a chemical irritant that causes inflammation and rapid degeneration of the joints and physically binding to connective tissue and altering the structure and interactions of the macromolecules.3 In most pediatric patients, darkening of the urine is the only feature that suggests alkaptonuria. This reaction is pH-dependent and never occurs in acidic urine. In the current series, 8 of 9 patients had a history of urine discoloration in childhood. One patient who was 47 years old had minimal urine discoloration, although urine pH was normal on examination. The diagnosis in this patient was made intraoperatively during total hip replacement for fracture nonunion of the neck of the femur when the femoral head was found to have black discoloration along with bluish-black discoloration of the soft tissue around the hip. Patients are usually asymptomatic until the third or fourth decade and usually do not seek medical at- DECEMBER 2014 | Volume 37 • Number 12 tention at an early age. The probable reason cited is the decrease in renal clearance with age.22 In the current series, 6 of 9 previously asymptomatic patients presented with low backache in the third to fourth decade. They did not seek medical attention for skin or urine discoloration, and all had a history of urine discoloration since childhood. Results of renal function tests and creatinine clearance were normal. Ochronosis presents as bluish-black or grayish-blue pigmentation of the pinna and outer ocular tissues such as the sclera, cornea, and conjunctiva. Scleral pigmentation (Osler’s sign) starts around the third decade. This sign was found in 2 patients. The effects are most noticeable in areas where the body is exposed to the sun and where sweat glands are located and are best appreciated in regions with thin overlying skin. All patients in the series had bluish-black pigmentation of the pinna. In addition, patients may have widespread dusky discoloration of the cheeks, forehead, axilla, and genitals. Nails may be stained brown.5 Brown nail color was found in only 2 patients in the authors’ series. Initial screening can be done with a simple biochemical test on a urine sample. With this testing, urine color changes to black with the addition of sodium hydroxide and a transient green color appears with the addition of ferric chloride. Other tests include the ammoniacal silver nitrate test, Benedict’s test, and the N-butanol test.23 The diagnosis is usually confirmed by detecting and measuring the amount of homogentisic acid in urine with gas liquid chromatography, thin-layer chromatography, or enzymatic spectrophotometry. In the current series, all patients were initially screened with 2 of the previously mentioned biochemical tests, mainly the addition of sodium hydroxide and ferric chloride. In all patients, the diagnosis was confirmed by thin-layer chromatography. Magnetic resonance imaging was used to establish the diagnosis in the patient with caries of the spine. In ochronosis, radiographs of the lumbar spine show gross calcification, vacuum phenomenon, and loss of height of the intervertebral disks accompanied by fusion (pseudo-block) vertebrae formation, predominantly in the dorsolumbar region.24 This typical presentation of reduced intervertebral disk space, vacuum phenomenon, and wafer calcification of the intervertebral disks on radiographs of the dorsolumbar region was seen in all patients. Although calcification has been seen in the menisci, symphysis pubis, pinnae, nasal cartilage, tendons, kidneys, heart walls, and great vessels,25 1 patient in the authors’ series had unusual intramedullary calcification of the femur. Grossly, the involved tissue usually shows pigmentation that varies from brown to black. Microscopically, the hyaline cartilage shows deposition of ochre-colored granules that is more marked in the deeper layers.4 Brownish-black pigmentation of the femur head, known as black hip, along with degenerate pigmented articular cartilage was found in 2 of the patients during hip replacement (Figure 9). Ochronotic arthropathy is a particularly troublesome feature. Premature arthritis in the large joints develops after the third decade and usually affects the weight-bearing joints, mainly the spine, hips, knees, and later the shoulders. Musculoskeletal manifestations are first noted in the spine. Typically, involvement of the large peripheral joints occurs several years after spinal involvement.20 Usually, involvement of these joints is severe and often requires joint replacement.4,24,26,27 In the authors’ series, 1 patient had severe arthropathy of 1 hip and underwent hip joint replacement. After 4 years of follow-up, he had a good Harris Hip Score of 86 and could perform normal routine activities. In contrast to rheumatoid arthritis, the smaller joints of the hand and feet are unaffected. The sacroiliac joint is also spared, thereby distinguishing this condition from ankylosing spondylitis. In e1143 n Case Report Table 1 Patient Profiles Case No./ Age, y/Sex Presenting Symptoms Family History Local Examination 1/47/M Pain in right groin for 3 y Limping more on right side Pain in left knee Generalized body aches Difficulty in ambulation Parents nonconsanguineous Siblings normal Stooping posture Restricted dorsolumbar spine movements Restricted movements of right hip joint and left knee Scleral pigmentation (Osler’s sign), with slate blue discoloration of skin over dorsum of hands, pinna, and nail bed Subcutaneous nodules over Achilles tendons and both knees (Figure 1) Patchy alopecia Limp with antalgic gait 2/49/M Progressive low backache for 15 y History of discoloration of both eyes for 4 y Pain in both knee, hip, shoulder, and elbow joints for last 12 y Unable to walk without support on admission Parents nonconsanguineous Siblings normal Stooping posture Scleral pigmentation Restricted dorsolumbar spine movements Tenderness in dorsolumbar region Painful and restricted range of motion of both knee joints, both hip joints (right more than left), and bilateral shoulder and elbow joints Scleral pigmentation (Osler’s sign), ochronotic pigmentation of skin over pinna, earlobes, and nail beds 3/34/M Laborer Low backache with radiation to back of thigh Stiffness and difficulty bending forward and doing hard work for last 4-5 y Increased pain intensity for last 6 mo and pain at night History of evening increase in temperature and loss of appetite for last 4-5 mo Severe limitation of activity and difficulty in performing work for gainful employment Brown-black discoloration of both ears for last 5-6 y Parents nonconsanguineous Siblings normal Brown pigmentation of both ears (more marked in right ear) Restricted movements in dorsolumbar region Tenderness in dorsal and lumbosacral spine Tenderness more marked at L3, L4, and L5, with marked tenderness on application of twisting force along base of spinous process; twist tenderness Neurologic examination: Brisk knee and ankle reflexes on presentation with ill-sustained ankle clonus Babinski: Extensor response Normal after 18 mo of antitubercular therapy 4/38/F Housewife Pain in lower back, difficulty bending forward and performing routine household activities for last 10 y Bluish-black discoloration of both ears for last 6-7 y Hyperthyroidism for last 5-6 y, with use of antithyroid drugs for same duration Parents nonconsanguineous Siblings normal Exophthalmos and brownish-black discoloration of cartilage of both pinnae Mild dorsolumbar kyphosis with tenderness and loss of lumbar lordosis 5/42/M Postman Low backache for last 6 y Bluish-black discoloration of both ears for last 5 y Parents nonconsanguineous Siblings normal Restricted movements at dorsolumbar spine, mainly flexion e1144 ORTHOPEDICS | Healio.com/Orthopedics n Case Report Table 1 (cont’d) Patient Profiles Case No./ Age, y/Sex Presenting Symptoms Family History Local Examination 6/38/M Farmer Low backache for last 9 y, initially when rising from sitting position, now constant Difficulty walking and doing moderate to heavy work Pain in both shoulders, knees, and hips for last 1.5 y Bluish-black discoloration of both ears for last 5 y Parents nonconsanguineous Siblings: Sister 4 y younger had similar problems for last 4 y (Case 7) Terminal restriction of internal and external rotation of both hips Restricted movements at dorsolumbar spine 7/34/F Housewife Low backache for last 4 y Pain while doing routine household work Parents nonconsanguineous Siblings: Brother 4 y older had similar problems for last 4 y (Case 6) Bluish-black discoloration of external ears and gums (Figure 2) Painful movements at dorsolumbar spine, mainly flexion 8/36/M Police constable Parents nonconsanguineous Siblings normal Painful movements at dorsolumbar spine, mainly flexion 9/50/M Farmer Presented with fracture Nonunion of neck of femur after primary fixation with partially threaded cancellous screws (Figure 3) Bluish-black discoloration of initial 2-3 drops of urine for last 3 y Pain in both knees for 3 y Parents nonconsanguineous Siblings normal Bluish-black discoloration of external ears Movements of knee joints terminally painful Abbreviations: F, female; M, male. the authors’ series, 7 of 9 patients had low backache primarily as the initial presentation. Associated involvement of the hips and knees occurred in 2 patients in the fifth decade, and the rest of the patients were in the third and fourth decades at the time of the study. Heart problems often start after 50 years of age.2 Patients may have signs of aortic or mitral valvulitis. Pigment deposits that lead to the formation of atherosclerotic plaques and calcification of the coronary arteries may be seen.28,29 Fisher et al20 reported a 69-year-old (seventh decade) patient with cardiovascular involvement who had severe aortic stenosis, calcified valves, and gross aortic pigmentation. The mean age of patients in the authors’ series was 39.7 years. None of the patients had cardiovascular involvement, possibly because they were relatively young. However, all DECEMBER 2014 | Volume 37 • Number 12 of the current patients underwent electrocardiography and echocardiography to rule out cardiovascular complications. The differential diagnosis includes osteoarthritis, ankylosing spondylitis, rheumatoid arthritis, and calcium pyrophosphate arthropathy. Disk calcification in the spine can also mimic hyperparathyroidism, hemochromatosis, amyloidosis, diffuse idiopathic skeletal hyperostosis, or surgical spinal fusion. All patients in this study had normal serum calcium, phosphate, and parathyroid hormone levels; therefore, hyperparathyroidism was excluded from the differential diagnosis. Similarly, in the absence of symmetrical polyarthritis, ruled out by relevant tests and investigations, there was no history of early morning stiffness, the rheumatoid factor finding was negative in all patients, and the erythrocyte sedimentation rate was normal in 7 patients except 1 who had caries of the spine. Rheumatoid arthritis was also ruled out because none of the patients had symmetrical polyarthritis or morning stiffness; rheumatoid factor was negative in all 9 patients; and the erythrocyte sedimentation rate was raised only in 1 patient with caries of the spine and normal in the other 8 patients. The HLA-B27 finding was negative in all patients, excluding ankylosing spondylitis. Serum ferritin levels were normal in all patients; this finding, associated with normal liver and renal profiles in all patients, excluded hemochromatosis. Genetically, alkaptonuria is inherited as an autosomal recessive trait. All of the close and remote relatives of all patients in the current study underwent screening, and there was no familial presentation in 7 patients. Only 2 patients, who were brother and sister, were affected, but their e1145 n Case Report Table 2 Investigations and Treatment Case No. Analyses Radiologic Findings Treatment 1 Normal Calcification of intervertebral disks with vacuum phenomenon at lumbar spine and narrowing of intervertebral disk space Radiographs of right hip showed degenerative changes and collapse of head of femur (Figure 5) Total hip replacement (Figure 4) Vitamin C 2 Normal Dorsolumbar spine radiograph showed wafer-like calcification of intervertebral disks, mainly in lumbar spine, and gas vacuum phenomenon with markedly decreased intervertebral disk space (Figure 6) Radiograph of knee joints showed features of arthritis with degenerative changes Radiograph of pelvis and hip joints showed decreased joint space bilaterally Computed tomography of dorsolumbar spine showed degenerative changes with vacuum phenomenon Radiograph of lower end of left femur showed intramedullary calcification (Figure 7) Vitamin C 3 Erythrocyte sedimentation rate 62 mm first h Radiologic examination of dorsolumbar spine Characteristic pathogenic changes of ochronosis, as in Case 2 At L3-L4, radiographs showed loss of disk space with anterior erosion over L4 Magnetic resonance imaging showed decreased intervertebral disk space, end-plate erosions, and abscess formation anteriorly (Figure 8) Antitubercular chemotherapy for 18 mo Vitamin C 4 Increased triiodothyronine and tetraiodothyronine and decreased thyroidstimulating hormone levels Radiograph showed decreased intervertebral disk space and calcification with osteoporosis Skeletal survey normal Antithyroid drugs Analgesics Symptomatic treatment Physical therapy 5 Normal Radiologic examination of dorsolumbar spine showed waferlike calcification of intervertebral disks, mainly in lumbar spine, and gas vacuum phenomenon with degenerative changes in dorsolumbar spine Vitamin C Analgesics Symptomatic treatment 6 Normal Characteristic wafer-like calcification of intervertebral disks, mainly in lumbar spine, and gas vacuum phenomenon with degenerative changes in dorsolumbar spine Radiograph of both hips showed early degenerative changes Vitamin C Analgesics Symptomatic treatment 7 Normal Characteristic wafer-like calcification of intervertebral disks, mainly in lumbar spine, and gas vacuum phenomenon with degenerative changes in dorsolumbar spine Vitamin C Analgesics Symptomatic treatment 8 Normal Wafer-like calcification of intervertebral disks, mainly in lumbar spine, and gas vacuum phenomenon with degenerative changes in dorsolumbar spine Vitamin C Analgesics Symptomatic treatment 9 Normal Fracture nonunion of neck of femur after fixation with partially threaded cancellous screws at 1 y Dorsolumbar spine radiograph showed wafer-like calcification of intervertebral disks, mainly in lumbar spine, and gas vacuum phenomenon with markedly decreased intervertebral disk space Radiograph of knee joints showed features of arthritis with degenerative changes Total hip replacement Vitamin C Analgesics Symptomatic treatment parents and grandparents had no symptoms. e1146 Compression of the cervical cord as a result of alkaptonuric arthropathy of the atlantoaxial joint has been reported.30 In the current series, 8 of 9 patients had ORTHOPEDICS | Healio.com/Orthopedics n Case Report Figure 3: Anteroposterior radiograph showing fracture nonunion of the neck of the femur 1 year postoperatively. Figure 4: Postoperative anteroposterior radiograph of total hip replacement. A B Figure 2: Photographs showing bluish-black discoloration of the external ears (A) and the gums (B). no neurologic deficit or gait disturbance. Findings on cervical spine examination were normal in all 9 patients. One patient with caries of the spine had exaggerated deep tendon reflexes of the lower limb along with an extensor Babinski response that resolved after 3 months of antitubercular therapy. Osteoporosis associated with alkaptonuria was reported in previous studies.31,32 Fisher et al20 reported low-energy trauma of the distal radius and femoral fracture despite 2 years of alendronate therapy. In the authors’ patients, although none presented with a fracture, 1 patient showed evidence of osteoporosis on radiographs of the lumbosacral spine. This finding was confirmed by bone mineral density analysis (T-score, 1.3). This patient had no risk factors for osteoporosis, such as malnutrition, immobility, smoking, medication (corticosteroids, anticonvulsants), or family history of osteoporotic fractures, although she had thyrotoxicosis. DECEMBER 2014 | Volume 37 • Number 12 A Figure 5: Preoperative anteroposterior radiograph of the right hip showing degenerative changes and collapse of the head of the femur. Tendon ruptures, chiefly of the Achilles tendon, have occurred and have been treated successfully with primary repair. One patient in this series also had subcutaneous nodules around the knees and Achilles tendons that were mobile and were not fixed to underlying structures. He also had patchy alopecia over the scalp. This presentation of ochronosis has not been reported before. Pseudo-ochronosis has been described as a result of argyria,33 which is a localized collection of silver granules in the glands, in the walls of blood vessels, and among elastic fibers. Pseudo-ochronosis is also found after long-term use of L-dopa, methyldopa,34 antimalarial agents, or products containing hydroxychloroquine, phenol, resorcinol, and mercury or picric acid.35 No patient in this study had a history of use of these drugs. It is necessary to obtain a history of drug intake in all patients because mi- B Figure 6: Anteroposterior radiograph of the dorsolumbar spine showing wafer-like calcification of the intervertebral disks, mainly in the lumbar spine, and gas vacuum phenomenon with markedly decreased intervertebral disk space (A). Lateral radiograph of the dorsolumbar spine showing wafer-like calcification of the intervertebral disks, mainly in the lumbar spine, and gas vacuum phenomenon with markedly decreased intervertebral disk space (B). e1147 n Case Report Figure 7: Radiograph of the lower end of the left femur showing intramedullary calcification. B A Figure 8: Coronal magnetic resonance imaging scan showing a patient with caries of the lumbar spine with decreased intervertebral disk space and end-plate erosions at L3, L4, and L5 (A). Sagittal magnetic resonance imaging scan showing a patient with caries of the lumbar spine with decreased intervertebral disk space and end-plate erosions at L3, L4, and L5 (B). A B Figure 9: Intraoperative photographs showing inferior (A) and superior (B) views of black pigmentation of the femur head. nocycline-induced pigmentation36 or intramuscular injection of quinine, leading to bluish-black pigmentation in the buttocks,37 resembles exogenous alkaptonuria. The authors found no such history among their patients. Currently, only symptomatic treatment of complications of alkaptonuria is available, and there is no specific or effective treatment of alkaptonuria. There are anecdotal reports that a diet low in e1148 protein, especially containing tyrosine and phenylalanine, can help to delay or partially reverse late manifestations.38 Vitamin C partially ameliorates the condition by impairing the polymerization of homogentisic acid21 and preventing homogentisic acid oxidase from binding to connective tissue. Wolff et al39 treated 2 adults with a high dose of ascorbic acid. They found that its derivative, benzoquinone, completely disappeared from urine. In the authors’ study, all patients were given vitamin C 500 mg 3 times a day. Six showed some clinical improvement, as assessed by a subjective pain rating score, on subsequent follow-up. Although nitisinone has been approved by the US Food and Drug Administration for the treatment of tyrosinemia type 115, its safety profile and outcome have not been established in alkaptonuria.4 Because alkaptonuria is rare, there is a high likelihood that it will be unnoticed, especially in areas where the incidence is low. Therefore, clinicians need a high index of suspicion and awareness to make the diagnosis of ochronosis. Low backache is common in the general popu- lation and is also the presenting symptom in the third to fourth decade in patients with ochronosis. There is a high probability that ochronosis in a patient who presents with low backache will be diagnosed as a simple case of dorsolumbar spondylosis unless the typical clinical features of urine discoloration and specific radiologic findings are correlated with backache. In developing and tropical countries, a high incidence of bone and joint tuberculosis exists, but its association in a patient with ochronosis confounded the diagnosis. Conclusion The current study is unique because of the presentation of 1 patient with subcutaneous nodules and 1 patient with associated caries of the spine. One patient had nonunion fracture of the neck of the femur and underwent total hip replacement. Although nonunion has not been described in ochronosis, it could be the cause in this case because the patient had no other risk factor for nonunion and underwent closed reduction and internal fixation with minimal manipulation after 48 hours of injury. ORTHOPEDICS | Healio.com/Orthopedics n Case Report At follow-up of 3 years, both patients with total hip replacement are normal. In these patients, morbidity and complications are significantly decreased by early diagnosis and management. Enzyme replacement with recombinant homogentisic acid oxidase enzyme could be a promising future therapy. The association of hyperthyroidism in 1 patient was an incidental finding. References 1. Stanbury JB, Wyngaarden JB, Fredrickson DS: Alkaptonuria. In: The Metabolic Basis of Inherited Disease. 4th ed. New York, NY: McGraw Hill; 1978:268-280. 2.Smith R. Disorders of the skeleton. In: Weatherall D, Ledingham J, Warrell D, eds. The Oxford Textbook of Medicine. Oxford University Press; 1996:3085-3086. 3. Keller JM, Macaulay W, Nercessian OA, Jaffe IA. New developments in ochronosis: review of the literature. Rheumatol Int. 2005; 25:81-85. 4. Phornphutkul C, Introne WJ, Perry MB, et al. Natural history of alkaptonuria. N Engl J Med. 2002; 347:2111-2121. 5. Parikh A, Khubchandani RP, Bharucha BA, Kumta NB, Pandya MB, Naik G. Alkaptonuria: a series of seven cases. J Assoc Physicians India. 1988; 36:565-566. 6. Virchow R. Em Fall von allgemeiner Ochronose der Knorpel und knorpelahnlichen Theile. Archiv fur Pathologische Anatomie und Physiologie und fur klinische Medizin. 1866; 37:212. 7.Vijaikumar M, Thappa DM, Srikanth S, Sethuraman G, Nadarajan S. Alkaptonuric ochronosis presenting as palmoplantar pigmentation. Clin Exp Dermatol. 2000; 25:305307. 8. Konttinen YT, Hoikka V, Landtman M, et al. Ochronosis: a report of a case and a review of literature. Clin Exp Rheumatol. 1989; 7:435444. 9. Janocha S, Wolz W, Srsen S, et al. The human gene for alkaptonuria (AKU) maps to chromosome 3q. Genomics. 1994; 19:5-8. 10. Zatkova A, Chmelikova A, Polakova H, Ferakova E, Kadasi L. Rapid detection methods for five HGO gene mutations causing alkap- DECEMBER 2014 | Volume 37 • Number 12 tonuria. Clin Genet. 2003; 63:145-149. 11. Stenn FF, Milgram JW, Lee SL, Weigand RJ, Veis A. Biochemical identification of homogentisic acid pigment in an ochronotic Egyptian mummy. Science. 1977; 197:566-568. 12. Lee SL, Stenn FF. Characterization of mummy bone ochronotic pigment. JAMA. 1978; 240:136-138. 13. Boedeker C. Ueber das Alcapton; ein neurer Beitrag zur Frage. Welche Stoffe des Harnes konnen Kupferreduction bewirken? Zeitschrift fur rationelle Medizin. 1859; 3(7): 130. 14. Wolkow M, Baumann E. Homogentisic acid. Zeitschrift fur Physiologische Chemie. 1891; 15:288. ochronotic arthropathy. Orthop Rev. 1990; 19:1005-1009. 27.Demir S. Alkaptonuric ochronosis: a case with multiple joint replacement arthroplasties. Clin Rheumatol. 2003; 22:437-439. 28.Dereymaeker L, Van Parijs G, Bayart M, Daenen W, Lauwerijns J, De Geest H. Ochronosis and alkaptonuria: report of a new case with calcified aortic valve stenosis. Acta Cardiol. 1990; 45:87-92. 29. Kragel AH, Lapa JA, Roberts WC. Cardiovascular findings in alkaptonuric ochronosis. Am Heart J. 1990; 120(6 pt 1):1460-1463. 15. Garrod AE. The Croonian lectures on inborn errors of metabolism: Lecture II. Alkaptonuria. Lancet. 1908; 2:73-75. 30. Kusakabe N, Tsuzuki N, Sonada M. Compression of the cervical cord due to alcaptonuric arthropathy of the atlanto-axial joint: a case report. J Bone Joint Surg Am. 1995; 77:274-277. 16. La Du BN. Alcaptonuria. In: Stanbury JB, Wyngaarden JB, Fredrickson DS. The Metabolic Basis of Inherited Disease. 4th ed. New York, NY: McGraw-Hill; 1978:268-282. 31.Savastano AA, Quigley DG, Scala ME. Spontaneous fractures associated with cortisone therapy in a patient with ochronosis. Am J Orthop Surg. 1969; 11:116-120. 17. Pollak MR, Chou Y-H, Cerda JJ, et al. Homozygosity mapping of the gene for alkaptonuria to chromosome 3q2. Nature Genet. 1993; 5:201-204. 32. Millea TP, Segal LS, Liss RG, Stauffer ES. Spine fracture in ochronosis: report of a case. Clin Orthop Relat Res. 1992; 208-211. 18. Albrecht H. Ueber Ochronose. Zeitschrift fur Heilkunde. 1902; 23:366. 19. Osler W. Ochronosis. Lancet. 1904; I:10. 20. Fisher AA, Davis MW. Alkaptonuric ochronosis with aortic valve and joint replacements and femoral fracture: a case report and literature review. Clin Med Res. 2004; 2(4):209-215. 21. Singh R, Mahadevan S, Bhadada S, Bhansali A. Lady with melanuria and arthralgias. J Assoc Physicians India. 2005; 53:1051. 22. Hamdi N, Cooke TD, Hassan B. Ochronotic arthropathy: case report and review of the literature. Int Orthop. 1999; 23:122-125. 23. Pratibha K, Seenappaand T, Ranganath K. Alkaptonuric ochronosis: report of a case and brief review. Indian J Clin Biochem. 2007; 22:158-161. 24.Spencer JMF, Gibbons C-LM, Sharp RJ, Andrew J, Athanasou NA. Arthroplasty for ochronotic arthritis. Acta Orthop Scand. 2004; 75(3):355-358. 25. Justesen P, Andersen P. Radiological manifestations in alkaptonuria. Skeletal Radiol. 1984; 11:204-208. 26. Carrier DA, Harris CM. Bilateral hip and bilateral knee arthroplasties in a patient with 33. Robinson-Bostom L, Pomerantz D, Wilkel C, et al. Localized argyria with pseudo-ochronosis. J Am Acad Dermatol. 2002; 46:222-227. 34. Rausing A, Rosen U. Black cartilage after therapy with levodopa and methyldopa. Arch Pathol Lab Med. 1994; 118:531-535. 35. Levin CY, Maibach H. Exogenous ochronosis: an update on clinical features, causative agents and treatment options. Am J Clin Dermatol. 2001; 2:213-217. 36. Suwannarat P, Phornphutkul C, Bernardini I, Turner M, Gahl WA. Minocycline-induced hyperpigmentation masquerading as alkaptonuria in individuals with joint pain. Arthritis Rheum. 2004; 50:3698-3701. 37. Bruce S, Tschen JA, Chow D. Exogenous ochronosis resulting from quinine injections. J Am Acad Dermatol. 1986; 15:357-361. 38.Morava E, Kosztolanyi G, Engelke UF, Wevers RA. Reversal of clinical symptoms and radiographic abnormalities with protein restriction and ascorbic acid in alkaptonuria. Ann Clin Biochem. 2003; 40:108-111. 39. Wolff JA, Barshop B, Nyhan WL, et al. Effects of ascorbic acid in alkaptonuria: alterations in benzoquinone acetic acid and an ontogenic effect in infancy. Pediatr Res. 1989; 26:140-144. e1149