Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
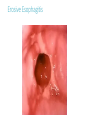
GASTROESOPHAGEAL REFLUX DISEASE (GERD) Summer 2013 Gastroesophageal Reflux Disease (GERD) Gastroesophageal reflux (GER) is defined as the retrograde passage of gastric contents from the stomach into the esophagus. It is primarily the result of transient relaxation of the LES. Gastroesophageal reflux is a normal physiologic phenomenon experienced intermittently by most people, particularly after a meal. Gastroesophageal reflux disease (GERD) occurs when the amount of gastric juice that refluxes into the esophagus exceeds the normal limit, causing symptoms with or without associated esophageal mucosal injury (i.e., esophagitis). High Prevalence of Gastroesophageal Reflux Symptoms 60% 50% 40% 30% 20% 10% 0% 59% 19.8% Weekly Monthly Frequency of heartburn and/or regurgitation Epidemiology GERD is a chronic disease that affects patients across all age groups with equal distribution between men and women. The prevalence of GERD appears to be greater in the Western population with patients presenting with more clinically important disease and complications than in Eastern countries (especially Asian populations) where GERD is uncommon. It has also been estimated that 7% of the U.S. population have complicated GERD associated with erosive esophagitis. Up to 75% of patients who undergo endoscopic procedures due to symptoms associated with GERD have normal esophageal findings. These patients are identified as having functional heartburn, (nonerosive reflux disease) NERD, or endoscopy-negative reflux disease (ENRD). Childhood GERD appears to continue into adolescence and adulthood. Although most infants develop physiological regurgitation, or spitting up, the majority (95%) will have abatement of symptoms by 1.0 to 1.5 years of age. infants with persisting symptoms beyond 2 years of age are at risk of developing complicated GERD. Epidemiology Complications associated with GERD include esophageal erosions (5%), strictures (4%–20%), and Barrett's metaplasia (8%–20%). Male gender and advancing age (men and women) are associated with an increase in the prevalence of esophageal complications, presumably due to refluxed acidic contents damaging the mucosa over time. No sexual predilection exists. The prevalence of GERD increases in people older than 40 years. Approximately 50% of patients with gastric reflux develop esophagitis. Pathophysiology Abnormal gastro-esophageal reflux is caused by the abnormalities of one or more of the following protective mechanisms: 1) Transient Relaxations of the Lower Esophageal Sphincter. The LES, when in a resting state, remains at a high pressure (10–30 mmHg) to prevent the gastric contents from entering into the esophagus. Pressures are lowest during the day and with meals and highest at night. Transient relaxations of the LES are short periods of sphincter relaxation that are different from those that occur with swallowing or peristalsis. They occur due to vagal stimulation in response to gastric distension from meals (most common), gas, stress, vomiting, or coughing and can persist >10 seconds. These transient relaxations of the LES are associated with virtually all GER events in healthy individuals but account for 50% to 80% of occurrences in patients with pathogenic GERD 2) Esophageal Acid Clearance and Buffering Capabilities. Peristalsis is the primary mechanism by which acid refluxate is removed from the esophagus. Other mechanisms include swallowing, esophageal distension in response to refluxate, and gravity (which is only effective when the patient is in an upright position). Saliva plays an important role in the neutralization of gastric acid within the esophagus. Its bicarbonate-rich content buffers the residual acid that remains in the esophagus after peristalsis The reduction of swallowing that occurs during sleep is associated with nocturnal GERD. Patients with decreased saliva production (e.g., elderly, patients taking medication with anticholinergic effects, and those with certain medication conditions such as xerostomia or Sjogren's syndrome) may also be at increased risk of developing GERD 3) Anatomic Abnormalities. 4) Gastric Emptying 5) Mucosal Resistance 6) Aggressive Factors Associated With Esophageal Damage Clinical Presentations of GERD Classic (Typical) GERD Extraesophageal (Atypical) GERD Complicated GERD Extraesophageal Manifestations of GERD Pulmonary Asthma Aspiration pneumonia Chronic bronchitis Pulmonary fibrosis Other Chest pain Dental erosion ENT Hoarseness Laryngitis Pharyngitis Chronic cough Globus sensation Dysphonia Sinusitis Subglottic stenosis Laryngeal cancer Potential Oral and Laryngopharyngeal Signs Associated with GERD • Edema and hyperemia of larynx • Vocal cord erythema, polyps, granulomas, ulcers • Hyperemia and lymphoid hyperplasia of posterior pharynx • Interarytenyoid changes • Dental erosion • Subglottic stenosis • Laryngeal cancer Vaezi MF, Hicks DM, Abelson TI, Richter JE. Clin Gastro Hep 2003;1:333-344. Gastroesophageal reflux disease (GERD) can cause typical (esophageal) symptoms or atypical (extraesophageal) symptoms. However, a diagnosis of gastroesophageal reflux disease (GERD) based on the presence of typical symptoms is correct in only 70% of patients. Therefore, GERD cannot be confirmed solely based on clinical symptoms. When to Perform Diagnostic Tests 1. Uncertain diagnosis 2. Atypical symptoms 3. Symptoms associated with complications 4. Inadequate response to therapy 5. Recurrent symptoms 6. Prior to anti-reflux surgery Diagnostic Tests for GERD Barium swallow Endoscopy Ambulatory pH monitoring Esophageal manometry Barium Swallow A barium esophagogram is particularly important for patients with gastroesophageal reflux disease (GERD) who experience dysphagia due to: Stricture (location, length) Mass (location, length) Bird’s beak Hiatal hernia (size, type). Limitations Detailed mucosal exam for erosive esophagitis, Barrett’s esophagus Endoscopy Indications for endoscopy Alarm symptoms Empiric therapy failure Preoperative evaluation Detection of Barrett’s esophagus Ambulatory 24 hr. pH Monitoring Physiologic study Quantify reflux in proximal/distal esophagus % time pH < 4 DeMeester score Symptom correlation Ambulatory 24 hr. pH Monitoring Normal GERD Wireless, Catheter-Free Esophageal pH Monitoring Potential Advantages • Improved patient comfort and acceptance • Continued normal work, activities and diet study • Longer reporting periods possible (48 hours) • Maintain constant probe position relative to SCJ Esophageal Manometry Limited role in GERD Assess LES pressure, location and relaxation Assist placement of 24 hr. pH catheter Assess peristalsis Prior to antireflux surgery Treatment Goals for GERD Eliminate symptoms Heal esophagitis Manage or prevent complications Maintain remission Step-wise progression of GERD therapy Phase I: Mild/occasional symptoms. Do not seek medical help. Phase II a: Persistent symptoms, mucosal damage. Phase II b: Severe mucosal damage. Phase III: Refractory disease. The following table summarizes the pharmacologic treatments for the different phases. Phase II a: Persistent symptoms, mucosal damage. Cimitidine 400 mg bid, ranitidine 150 mg bid, famotidine 20 mg bid, nizatidine 150 mg bid. Metoclopramide 10-20 mg ac and HS Phase II b: severe mucosal damage. Cimitidine 800 mg bid or 400 mg qid, ranitidine 150 mg qid, famotidine 40 mg bid, nizatidine 150 mg qid Metoclopramide 10-20 mg ac and HS PPI Phase III: refractory disease. Anti-reflux surgery. PPI bid for a short period of time. If no improvement, consider surgery. Approximately 80% of patients have a recurrent but nonprogressive form of gastroesophageal reflux disease (GERD) that is controlled with medications. Identifying the 20% of patients who have a progressive form of the disease is important, because they may develop severe complications, such as strictures or Barrett esophagus. For patients who develop complications, surgical treatment should be considered at an earlier stage to avoid the sequelae of the disease that can have serious consequences. Indications for fundoplication include the following: Patients with symptoms that are not completely controlled by PPI therapy can be considered for surgery. Surgery can also be considered in patients with wellcontrolled gastroesophageal reflux disease (GERD) who desire definitive, one-time treatment. The presence of Barrett esophagus is an indication for surgery. Whether acid suppression improves the outcome or prevents the progression of Barrett esophagus remains unknown, but most authorities recommend complete acid suppression in patients with histologically proven Barrett esophagus. The presence of extraesophageal manifestations of gastroesophageal reflux disease (GERD) may indicate the need for surgery. These include the following: (1) respiratory manifestations (eg, cough, wheezing, aspiration); (2) ear, nose, and throat manifestations (eg, hoarseness, sore throat, otitis media); and (3) dental manifestations (eg, enamel erosion). Young patients Poor patient compliance with regard to medications Postmenopausal women with osteoporosis Patients with cardiac conduction defects Cost of medical therapy Treatment Antacids Over the counter acid suppressants and antacids appropriate initial therapy Approx 1/3 of patients with heartburn-related symptoms use at least twice weekly More effective than placebo in relieving GERD symptoms Antacids: work within 5-15 minutes. Duration of relief 1-3 hours. An adult dose is about 40-80 mEq acid-neutralizing capacity (ANC) taken 4-5 times daily. Sodium Bicarbonate Calcium Carbonate Aluminum Hydroxide Magnesium Hydroxide Magnesium-Aluminum Hydroxides Possible interactions with tetracyclines, quinolone antibiotics, iron supplements, digoxin, azithromycin. Alginic acid: works by forming sodium alginate which is a viscous solution that floats on the surface of gastric contents so that when reflux occurs, sodium alginate rather than acid is refluxed and irritation is minimized. Tablets should be chewed and taken with a full glass of water. Should be taken when patients are in an upright position. NOT at bedtime. Common Alginic Acid Products Treatment: H-2 Blockers Histamine H2-receptor antagonists are the first-line agents for patients with mild to moderate symptoms and grades I-II esophagitis. Histamine H2 receptor antagonists are effective for healing only mild esophagitis in 70-80% of patients with gastroesophageal reflux disease (GERD) and for providing maintenance therapy to prevent relapse. Tachyphylaxis has been observed, suggesting that pharmacologic tolerance can reduce the long-term efficacy of these drugs. Additional H2 blocker therapy has been reported to be useful in patients with severe disease (particularly those with Barrett esophagus) who have nocturnal acid breakthrough. More effective than placebo and antacids for relieving heartburn in patients with GERD Faster healing of erosive esophagitis when compared with placebo Can use regularly or on-demand. Treatment AGENT EQUIVALENT DOSAGE DOSAGES Cimetadine 400mg twice daily 400-800mg twice daily 20mg twice daily 20-40mg twice daily 150mg twice daily 150mg twice daily 150mg twice daily 150mg twice daily Tagamet Famotidine Pepcid Nizatidine Axid Ranitidine zantac Treatment: PPI Proton Pump Inhibitors Better control of symptoms with PPIs vs H2RAs and better remission rates Faster healing of erosive esophagitis with PPIs vs H2RAs Treatment AGENT EQUIVALENT DOSAGE DOSAGES Esomeprazole 40mg daily 20-40mg daily 40mg daily 20mg daily 30mg daily 15-10md daily 40mg daily 40mg daily 20mg daily 20mg daily Nexium Omeprazole Prilosec Lansoprazole Prevacid Pantoprazole Protonix Rabeprazole Aciphex Newest PPI on the market Dexlansoprazole (trade names Kapidex, Dexilant) is a proton pump inhibitor that is marketed by Takeda Pharmaceuticals. Chemically, it is an enantiomer of lansoprazole. The compound was launched in the US for use in the treatment and maintenance of patients with erosive oesophagitis and non-erosive gastro-oesophageal reflux disease. Dexlansoprazole was approved by the U.S. Food and Drug Administration (FDA) on January 30, 2009 OTC PPI Products OTC PPI strengths and dosage forms: Omeprazole 20 mg delayed release tablets. Omeprazole and sodium bicarbonate 20/1100 mg immediate release capsules. Lansoprazole 15 mg delayed release capsules. Treatment H2RAs vs PPIs 12 week freedom from symptoms 48% vs 77% 12 week healing rate 52% vs 84% Speed of healing 6%/wk vs 12%/wk Effectiveness of Medical Therapies for GERD Treatment Response Lifestyle modifications/antacids 20 % H2-receptor antagonists 50 % Single-dose PPI 80 % Increased-dose PPI up to 100 % Summary of Treatment Algorithm for GERD Figure 26-5 Management of gastroesophageal reflux disease. H2RA, H2-receptor antagonist; PPI, proton pump inhibitor. If Initial Treatment Fails, the Following Should be Considered: Improve compliance Optimize pharmacokinetics Adjust timing of medication to 15 – 30 minutes before meals (as opposed to bedtime) Allows for high blood level to interact with parietal cell proton pump activated by the meal Consider switching to a different PPI GERD is a Chronic Relapsing Condition Esophagitis relapses quickly after cessation of therapy > 50 % relapse within 2 months > 80 % relapse within 6 months Effective maintenance therapy is imperative Brain Storming! (2-slides) Can PPIs be co-adminstered with antacids / H2 blockers? What should be the patient’s instructions? Why is omperazole 10 mg capsules Rx only while 20 mg tablets is OTC? Since 95% of the proton pumps will be permanently inactivated within 5 days of single daily use of a full-dose PPI, what is the rationale for twice daily dosing? Several weeks after daily dosing of a PPI, patients usually complain of breakthrough heartburns. Why is that? How can this be managed? A patient did not get a full relief with omeprazole 40 mg daily. Should we increase the dose to 80 mg or change into another PPI? What are the main differences in indications and use instructions between OTC and Rx PPI products? Complications of GERD Erosive/ulcerative esophagitis Esophageal (peptic) stricture Barrett’s esophagus Adenocarcinoma Erosive Esophagitis Peptic Stricture Barium Swallow Endoscopy Esophageal Stricture: Dilating Devices TTS Balloon Dilation of a Peptic Stricture Barrett’s Esophagus Esophageal Cancer Barium Swallow Endoscopy