Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
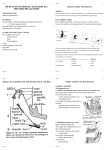
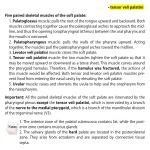
The Laryngoscope C 2012 The American Laryngological, V Rhinological and Otological Society, Inc. How I Do It Total Soft Palate Reconstruction Using the Palatal Island and Lateral Pharyngeal Wall Flaps William E. Karle, BS; Sumeet M. Anand, MD, MSc; Jason B. Clain, BS; Sophie Scherl, BA; Mark L. Urken, MD, FACS Key Words: Reconstructive surgical procedures, palatal island flap, soft palate reconstruction, lateral pharyngeal wall flap. Laryngoscope, 123:929–933, 2013 INTRODUCTION MATERIALS AND METHODS The palatal island flap has been well described for head and neck cancer reconstruction to repair defects in sites such as the soft palate, hard palate, retromolar trigone, cheek, tonsil, and lateral pharyngeal wall.1–6 This flap is particularly versatile; however, when used alone for soft palate repair the technique provides only an adynamic reconstruction. In view of this, the lateral pharyngeal wall flap can be used in conjunction with the palatal island to add a dynamic feature that can help to restore the sphincteric function of the velopharynx. We report the use and advantages of employing the palatal island flap in conjunction with the lateral pharyngeal wall flap in a single-staged reconstruction of large soft palate defects. This operation has been highly successful, with low complication rates, due to the high vascularity of the involved flaps, decrease in surgical complexity, and recreation of mucosal lining to the oral and nasal surfaces of the repair. The latter feature helps to add to the predictability of the results through the prevention of granulation tissue formation. We propose that this procedure be considered more often in the surgical reconstruction of large soft palate defects. In select cases, an elective tracheostomy should be considered at the beginning of the operation for airway protection. Once the resection of the soft palate is performed, an oncologic clearance of the tumor is established by frozen section analysis prior to embarking on the reconstruction (Fig 1). Subsequently, restoring the velopharynx can be undertaken. The nasopharyngeal surface of the soft palate is created with two opposing musculomucosal flaps from the lateral pharyngeal wall. The lateral pharyngeal walls are undermined in a submuscular plane starting at the posterior margin of the resection, usually at the level of the posterior tonsillar pillar (Fig. 2). The myomucosal superior and medial pharyngeal constrictors and pharyngeal mucosa are recruited from the lateral pharynx and advanced to the midline to form the nasopharyngeal surface of the neo-soft palate. Creation and closure of the inner myomucosal tube on itself creates a single dynamic chamber from the nasopharynx to the oropharynx (Fig. 3). Once the nasopharyngeal aspect of the soft palate has been created, attention is directed to the palatal island flap. Harvest of the palatal island is initiated by making an incision around the perimeter of the hard palate mucosa within a 5-mm gingival margin medial to the teeth. The incision is extended posteriorly to the hard and soft palate junction bilaterally. Using a freer elevator, the mucoperiosteum is elevated from the bone in an anterior to posterior fashion. One neurovascular pedicle is preserved, whereas the other is ligated with surgical clips. The flap is rotated 180 on its axis, maintaining the mucosal surface oriented toward the oral cavity. The entire palatal island flap is subsequently sutured directly to the margins of the defect with its deep surface apposing the transposed myomucosal pharyngeal flaps to form the oropharyngeal surface of the neo-soft palate. The suture line usually extends laterally along the anterior tonsillar pillar and helps to ensure the posterior positioning of the palatal island flap. The transposed palatal island flap has a tendency to lift away from the palatal bone along its leading edge. This can be overcome by placing boneanchored sutures that are drilled into the palatal bone along the edge and used to appose the palatal flap to the boney surface (Fig. 4). Tension-free closure is imperative on the nasopharyngeal and oropharyngeal side of the neo-soft palate (Fig. 5). From the Albert Einstein College of Medicine (W.E.K.); Thyroid Head and Neck Cancer Foundation (W.E.K., J.B.C., S.S.); and Department of Otolaryngology–Head and Neck Surgery (S.M.A., M.L.U.), Beth Israel Medical Center, New York, New York, U.S.A. Editor’s Note: This Manuscript was accepted for publication September 19, 2012. The authors have no funding, financial relationships, or conflicts of interest to disclose. Send correspondence to William E. Karle, 9 Ryan Rd., Troy, NY 12182. E-mail: [email protected] DOI: 10.1002/lary.23787 Laryngoscope 123: April 2013 Karle et al.: Soft Palate Reconstruction 929 Fig. 1. Palatal tumor. Preoperative appearance of a carcinoma involving the central soft palate with the proposed lines of resection. Fig. 3. Nasopharyngeal surface of neo-soft palate. The myomucosal constrictor flaps are advanced and sutured together in the midline to resurface the nasopharyngeal surface of the neo-soft palate. This restores the dynamic sphincteric function of the velopharynx and achieves a mucosal-lined conduit as well. RESULTS We report the representative case of a 74-year-old female with a 70 pack-year smoking history who originally presented with odynophagia and was diagnosed with squamous cell carcinoma of the central portion of the soft palate (Fig. 6). Because the tumor crossed the midline, the patient underwent a total soft palatectomy and bilateral cervical lymph node dissections. Pathological analysis demonstrated a 4-cm, moderately differentiated, squamous cell carcinoma with invasion into underlying skeletal muscle. All resection margins were negative. This defect was reconstructed using two lateral pharyngeal wall flaps in conjunction with a palatal island flap in the manner described above. The postoperative course was unremarkable and she was started on a liquid oral diet 7 days postoperatively and discharged on day 10. At her 4-week follow-up visit, the wound was well healed and she did not complain of any discomfort. The anterior palatal bone had remucosalized at this point in time. At this point the patient was not experiencing any difficulties with nasal breathing. Video nasal endoscopy, nasometry, and modified barium swallow examinations showed velopharyngeal closure upon deglutition and an absence of hypernasality and regurgitation (Figs. 7–9). When this article was submitted, the patient was 12 months postoperative with no documented recurrence and was eating a regular diet. It is important to mention that this patient did not receive radiation therapy postoperatively. This decision was made due to the lack of evidence of suspicious adenopathy on preoperative imaging and because the patient was pathologically N0 following bilateral selective neck dissections. DISCUSSION Fig. 2. Raising lateral pharyngeal wall flaps. Following resection of the entire soft palate, the lateral walls of the oropharynx, with the underlying constrictor muscles, are recruited by undermining in the prevertebral plane and advancing those flaps to the midline. Laryngoscope 123: April 2013 930 Today, there are several different procedures available to surgeons for the reconstruction of large soft palate defects. These include, but are not limited to, the use of various tongue, buccal, pharyngeal, palatal, and free flaps as well as the use of prosthetic obturators.2,3,6–9 Faced with this wide variety of options it is important to know what realistic outcomes one can expect and how reliably one can achieve them. The goals for soft palate reconstruction include preserving swallow function and maintaining normal speech, while also minimizing donor Karle et al.: Soft Palate Reconstruction Fig. 4. Transposition of palatal island. The palatal island flap is harvested and transposed through an arc of 180 to resurface the oral side of the neo-soft palate. The palatal island flap is sutured to the edges of the defect as shown, including the free edge of the myomucosal flaps that are lining the nasopharynx. The anterior edge of the palatal island flap is anchored to the bone with the use of bone-anchored screws and attached sutures that achieve adherence of that edge to the palatal bone. site morbidity.7,10,11 One of the pitfalls associated with several reconstructive techniques is the adynamic nature of the newly created soft palate. Although free tissue transfer has become a common practice in head and neck reconstruction, this creates a repair that produces a relatively immobile soft palate. It is a direct result of its adynamic nature that may this approach may cause complications in speech and swallowing function. Although the palatal island flap acts as an adynamic replacement for the soft palate,12 the lateral pharyngeal Fig. 5. Finalized creation of the neo-soft palate. The reconstructed soft palate achieves the goal of a mucosal-lined and dynamic conduit between the oropharynx and the nasopharynx. The hard palate remucosalizes over the course of several weeks through the process of healing by secondary intention. Laryngoscope 123: April 2013 wall maintains its muscular innervation allowing contraction with each swallow, facilitating sphincter closure. The recruitment of constrictor muscles allows closure of a velopharynx, which although smaller in caliber than the native pharyngeal opening, remains dynamic. Of note, suturing the palatal island flap to the transposed lateral pharyngeal wall flaps prevents the anterior migration of the free edge of the neo-soft palate, which occurs in most forms of soft palate reconstruction. Closure of the velopharyngeal sphincter through apposition of the soft palate and superior pharyngeal constrictor muscles separates the nasopharynx from the oropharynx, which is essential for normal deglutition and speech. Previous studies have shown that when used in conjunction with an adynamic flap, the pharyngeal wall flap can also greatly decrease the incidence of nasality.12 Zeitels and Kim13 have also noted success obtaining velopharyngeal competence with a similar superior-constrictor advancement-rotation flap. Fig. 6. Carcinoma prior to resection. Intraoperative planning for soft palate resection marked with purple dye. Carcinoma visualized at 3 cm in diameter at the posterior margin of the soft palate. Karle et al.: Soft Palate Reconstruction 931 Fig. 7. Postoperative sagittal computed tomography (CT). Sagittal CT view of the patient 1 month postoperatively. Arrow points to the neo-soft palate. In our experience, none of our patients undergoing the procedure described have required speech therapy for hypernasality. In our current era of functional reconstruction, a basic premise is to use the simplest and safest technique to accomplish a desired goal. As such, the benefit of using local flaps to ideally restore defects using ‘‘like tissue’’ represents the ideal method in most circumstances, provided it achieves the desired goals and does not disturb the functionality of the region from which the tissue is transferred.3 Although free tissue can be transferred to the head and neck using microvascular techniques, the oral cavity and oropharynx remain ideal donor sites to restore the soft palate without incurring significant secondary morbidity. Although the lateral pharyngeal wall flap has been used in combination with other adynamic flaps for soft palate reconstruction, the palatal island offers the simplest and most resilient option. The palatal island flap is an ideal treatment for oropharyngeal defects because of its thin, pliable, highly vascularized, sensate, and mucous-secreting properties.4 Taking periosteum with the palatal island flap also gives rigidity to the neo-soft palate. Another advantage of employing this flap over others is that the secondary defect overlying bone is able to heal by secondary intention within 4 to 6 weeks, provided that the patient has not been previously treated with radiation therapy, which is a contraindication to the use of this flap. Because healing by secondary intention often leads to contraction of the donor site defect, the use of the palatal island flap is unique in that the remucosalization of the hard palate is not at risk for distortion due to the fact that it is occurring over a boney surface.10 Usually this technique is a great surgical option; however, it has certain contraindications including previous radiation therapy to the palate, ipsilateral external carotid or internal maxillary artery ligation, or previous oral or Laryngoscope 123: April 2013 932 Fig. 8. One month postoperative nasoendoscopy. (a) Patent velopharynx at rest. (b) Complete closure of the velopharynx while the patient is instructed to say ‘‘papapa.’’ oropharyngeal surgery that has significantly disturbed the vascular supply.3,4 In addition, the use of this procedure is not recommended for smaller soft palate defects, where simpler reconstructive options are preferable. Fig. 9. Three months postoperative neo-soft palate. Complete healing of the donor and recipient sites within the oropharynx. Karle et al.: Soft Palate Reconstruction CONCLUSION The benefits achieved by combining these two pedicle flaps are: 1) maintaining dynamic function of the soft palate, 2) maintaining function of the superior and middle posterior wall constrictors, 3) preventing nasality in speech and nasal regurgitation, 4) lowering risks of patient and donor site morbidity, and 5) creating a simplified surgical procedure as compared to microvascular free tissue transfer. Although advancements in microsurgery have driven the expansion in the use of free tissue transfer, this article demonstrates the continued importance and advantages of using local pedicle flaps in soft palate reconstruction. BIBLIOGRAPHY 1. Seckel NG. The palatal island flap on retrospection. Plast Reconstr Surg 1995;96:1262–1270. 2. Gullane PJ, Arena S. Palatal island flap for reconstruction of oral defects. Arch Otolaryngol Head Neck Surg 1977;103:598–599. 3. Genden EM, Lee BB, Urken ML. The palatal island flap for reconstruction of palatal and retromolar trigone defects revisited. Arch Otolaryngol Head Neck Surg 2001;127:837–841. Laryngoscope 123: April 2013 4. Gullane PJ, Arena S. Extended palatal island mucoperiosteal flap. Arch Otolaryngol Head Neck Surg 1985;111:330–332. 5. James R. Surgical closure of large oroantral fistulas using a palatal island flap. J Oral Surg 1980;38:591–595. 6. Ducic Y, Herford AS. The use of palatal island flaps as an adjunct to microvascular free tissue transfer for reconstruction of complex oromandibular defects. Laryngoscope 2001;111:1666–1669. 7. Kimata Y, Uchiyama K, Sakuraba M, et al. Velopharyngeal function after microsurgical reconstruction of lateral and superior oropharyngeal defects. Laryngoscope 2002;112:1037–1042. 8. Komisar A, Lawson W. A compendium of intraoral flaps. Head Neck Surg 1985;8:91–99. 9. Chepeha DB, Sacco AG, Erickson VR, et al. Oropharyngoplasty with template-based reconstruction of oropharynx defects. Arch Otolaryngol Head Neck Surg 2009;135:887–894. 10. Harrid JR, Seikaly H, Urken ML, Okay DJ, Rieger J. Oropharyngeal reconstruction. In: Urken ML, ed. Multidisciplinary Head and Neck Reconstruction: A Defect-Oriented Approach. Philadelphia, PA: Lippincott Williams &Wilkins; 2010:647–688. 11. Moore BA, Magdy E, Netterville JL, Burkey BB. Palatal reconstruction with the palatal island flap. Laryngoscope 2003;113:946–951. 12. Brown JS, Zuydam AC, Jones DC, Rogers SN, David Vaughan E. Functional outcome in soft palate reconstruction using a radial forearm free flap in conjunction with a superiorly based pharyngeal flap. Head Neck 1997;19:524–534. 13. Zeitels SM, Kim J. Soft-palate reconstruction with a ‘‘SCARF’’ superiorconstrictor advancement-rotation flap. Laryngoscope 1998;108: 1136–1140. Karle et al.: Soft Palate Reconstruction 933