Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
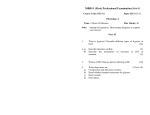
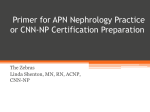
Nephrol Dial Transplant (2006) 21: 488–493 doi:10.1093/ndt/gfi266 Advance Access publication 9 November 2005 Original Article Conversion from calcineurin inhibitors to sirolimus in chronic allograft dysfunction: changes in glomerular haemodynamics and proteinuria Anna Saurina1, Josep M. Campistol2, Carlos Piera3, Fritz Diekmann2, Begoña Campos4, Nieves Campos3, Xavier de las Cuevas1 and Federico Oppenheimer2 1 Nephrology Department, Hospital de Terrassa, 2Renal Transplant Unit, Hospital Clı́nic de Barcelona, Nuclear Medicine Department, Hospital Clı́nic de Barcelona and 4Statistics Department, Universitat de Barcelona, Spain 3 Abstract Background. The study was conducted in order to describe possible intraglomerular haemodynamic changes inducing proteinuria after 14 patients with chronic allograft dysfunction were converted from calcineurin inhibitors (CIs) to sirolimus without changing concomitant immunosuppression or antihypertensive treatment. Methods. Creatinine, glomerular filtration rate (GFR), proteinuria, renal functional reserve (RFR) and effective renal plasma flow (ERPF) were determined before and 8 months after conversion. Intraglomerular pressure (PG), afferent arteriolar resistance (AAR) and efferent arteriolar resistance (EAR) were calculated using Gomez’s formula. Results. Creatinine (1.97 vs 2.075 mg/dl; P ¼ 0.270) and GFR (40 vs 43 ml/min; P ¼ 0.505) remained unchanged, proteinuria increased (338 vs 1146 mg/ 24 h; P ¼ 0.006), RFR decreased (34.84 vs 13.47%; P ¼ 0.019), ERPF (248 vs 310.6 ml/min; P ¼ 0.0625) and PG (42.72 vs 46.17 mmHg; P ¼ 0.0625) tendentially increased and AAR tendentially decreased (14.12 vs 10.28 dyne/s/cm5; P ¼ 0.0625). Conclusion. After conversion, PG shows a tendency to increase and RFR decreases significantly—characteristics of hyperfiltration, which could possibly partially explain the increase of proteinuria. Therefore, the application of angiotensin-converting enzyme inhibitors or angiotensin II receptor blockers seems promising. To avoid hyperfiltration, conversion should be performed early when renal insufficiency is still moderate. Correspondence and offprint requests to: Josep M. Campistol, Unidad de Trasplante Renal, Hospital Clı́nic, Villarroel 170, E-08036 Barcelona, Spain. Email: [email protected] Keywords: calcineurin inhibitors; CAD; hyperfiltration; proteinuria; sirolimus Introduction The clinical phenomenon of chronic allograft dysfunction (CAD) most often finds its histopathologic correlate in chronic allograft nephropathy (CAN) as defined by the BANFF 97 classification. CAN is the most prevalent cause of late transplant failure [1] and is characterized by a slow loss of renal function often in combination with proteinuria and hypertension. None of the clinical manifestations are specific and other causes of graft dysfunction such as acute rejection, drug toxicity or other glomerulopathies must be excluded to diagnose CAN [2]. Although several risk factors have been implicated, the pathophysiology and aetiology of CAN are not completely understood. Both immunological and non-immunological factors play a role in the development of CAN. With the introduction of calcineurin inhibitors (CIs) in the early 1980s, the incidence of acute rejection episodes decreased, and 1-year survival improved. However, the rate of loss of renal function in long-term kidney transplant patients >1 year after transplantation has not significantly changed over the past decades [1]. CI therapy can cause functional and histological renal impairment and has been suggested to be an important cause of the development of CAN [1,3]. The use of these agents at therapeutic doses, sufficient to prevent allograft rejection, generally reduces the glomerular filtration rate (GFR) by 15–25% and may lead to tubulointerstitial fibrosis. A recent publication by Nankivell et al. demonstrated that CI nephrotoxicity is increasingly prevalent and is even virtually universal 10 years after ß The Author [2005]. Published by Oxford University Press on behalf of ERA-EDTA. All rights reserved. For Permissions, please email: [email protected] Proteinuria after conversion from calcineurin inhibitors to sirolimus transplantation. Despite slight to moderate reductions in CI doses, the nephrotoxicity is progressive and is the chief cause of late histological injury and ongoing decline of renal function [3]. Sirolimus (SRL) is a new agent with lymphocytespecific features similar to those of CIs but with a different mechanism of action and side effect profile. SRL does not appear to be nephrotoxic and might protect against chronic rejection and graft vascular disease. The ability of SRL to inhibit cytokine- and growth factor-stimulated proliferation of non-immune cells appears to account for the effects observed in animals. Given the proliferative processes predominant in chronic rejection, the inhibitory effects of SRL might be useful in preventing chronic rejection. In 1983, Bosch and colleagues [4] demonstrated that GFR is submaximal under normal conditions and that the difference between the baseline value and the maximum value after protein load represents the so-called ‘renal functional reserve’ (RFR). The RFR is directly correlated with the number of properly functioning glomeruli and inversely correlated with the number of destroyed glomeruli, and represents the capacity of the kidney to increase its level of activity under demanding conditions. Several studies of conversion from CI-based to SRLbased immunosuppression in patients with CAD have demonstrated that conversion improves renal function. However, in some patients, conversion is associated with a significant increase of proteinuria [5,6]. The exact aetiology of proteinuria is not completely known, but haemodynamic changes may play a significant causative role. The aim of this study was to describe and investigate if substitution of CI with SRL in renal transplant patients with CAD induces changes in glomerular haemodynamics that can explain the increase of urinary protein excretion often accompanied by CI withdrawal and introduction of SRL. Patients and methods Patients Fourteen renal transplant patients were included in our study >1 year after renal transplantation. All patients were treated with CIs and had clinical signs of CAD. In all patients, a transplant biopsy was scheduled to confirm the diagnosis histologically. In six patients, transplant biopsies could be performed, all of them showing signs of CAN. Four patients were classified as Banff grade I, and the remaining two patients were classified as Banff grade II and III, respectively. Inclusion criteria were: transplantation performed >1 year previously, moderate renal insufficiency (creatinine level: 1.5–2.5 mg/dl) without an increase of >25% in the previous year, and proteinuria <1.5 g/24 h. Patients with other causes of renal dysfunction, diabetes or hypertension due to renal artery stenosis were excluded from the study. All patients provided written informed consent, and the ethics committee of our hospital approved the protocol. 489 Study design Serum creatinine, proteinuria/24 h, effective renal plasma flow (ERPF) and GFR before and after a protein infusion to calculate RFR were determined. After these studies, the CI was withdrawn in all patients and was replaced with SRL. Co-adjuvant immunosuppressive treatment was maintained throughout the study period. On day 1 of conversion, SRL was introduced at a dose of 2 mg/day and changed according to SRL target trough concentrations of 8–12 ng/ml. Simultaneously, the CI dose was reduced by 50%. After achieving the SRL target trough concentration, CIs were progressively eliminated within 6 weeks. Eight months after withdrawal of CIs, the above-mentioned studies were repeated. In order to study proteinuria, the mean of three independent measurements separated by 4 weeks each both before and after conversion was calculated. In order to avoid other influences on glomerular haemodynamics, no changes were made to baseline antihypertensive treatment nor angiotensin-converting enzyme inhibitor (ACEI) or angiotensin II receptor blocker (ARB) treatment during the study period. Measurement methods Measurements of serum creatinine, total protein (TP), haematocrit (Hct), 24 h proteinuria and urine electrophoresis were performed by routine techniques. SRL blood trough concentrations were measured using a high-performance liquid chromatography assay with double mass spectrometry. GFR and ERPF were studied using the open bicompartmental method of Sapirstein and Blaufox [7] with [99mTc]DTPA and [131I]orthoiodohippurate, respectively. After 48 h, GFR was determined again during an amino acid infusion (Aminoplasmal L-10 without electrolytes, B. Braun Medical SA, Rubı́, Barcelona). To study RFR, saline alone was administered intravenously during the first hour to compensate for osmotic diuresis after the beginning of the amino acid infusion. In the second hour, the amino acid infusion was started at 4.5 mg/kg/min and the application of intravenous saline was maintained at 20% of the total volume/h of amino acid infusion. The volume of saline infusion during the first hour is the total saline and amino acid volume of 1 h. At the beginning of the third hour, we started the study of GFR and ERPF with infusion of [99mTc]DTPA and [131I]orthoiodohippurate. Gomez’s equations were used to calculate glomerular hydrostatic pressure (PG), afferent arteriolar resistance (AAR) and efferent arteriolar resistance (EAR) [8]. The filtration coefficient (KFG) of glomerular capillaries was assumed to be 0.0812 (ml/s)/mmHg and the PG in Bowman’s space (HT) to be 10 mmHg. Measurements such as mean arterial pressure (MAP), GFR, ERPF, renal blood flow (RBF), Hct and TP were used to estimate the intrarenal haemodynamics quantitatively. RBF was calculated as RBF (ml/min) ¼ ERPF/(1 – Hct). The filtration fraction (FF) was calculated as FF ¼ (GFR/ERPF) 100. Statistical analysis Values before and after conversion were compared with a Wilcoxon signed rank test. SPSSÕ (version11) software was used to make the calculations. Asymptomatic P-values <0.05 490 A. Saurina et al. Table 1. Patients Age Sex Aetiology of renal disease Transplant Origin Time after transplantation Treatment before (months) conversion Follow-up 32 44 55 56 55 72 31 47 66 30 68 67 34 42 Second First First First First First First First First First First First First First 78 50 92 25 145 78 204 175 103 94 162 84 101 192 Yes Yes Yes Yes Yes Yes Lost Yes Yes Lost Yes Yes Yes Yes M F M F F M F M M M M F M F Unknown FSGN Unknown Chronic GN Interstitial nephropathy IgA nephropathy Membranoproliferative GN Unknown Nephroangiosclerosis Membranoproliferative GN Nephroangiosclerosis FSGN IgA nephropathy Unknown Cadaveric Cadaveric Cadaveric Cadaveric Cadaveric Cadaveric Living donor Cadaveric Cadaveric Cadaveric Cadaveric Cadaveric Cadaveric Cadaveric CsA þ AZA þ steroids Tacrolimus þ MMF þ steroids CsA Tacrolimus þ MMF þ steroids CsA CsA CsA CsA þ steroids CsA CsA CsA CsA þ steroids CsA þ AZA CsA AZA ¼ azathioprin; CsA ¼ cyclosporin A; MMF ¼ mycophenolate mofetil; FSGN ¼ focal segmentary glomerulonephritis; GN ¼ glomerulonephritis. were considered to be significant, except in the case of n<6 where an alpha error of <10% was applied according to critical values tables [9]. All analyses of significance were based on a two-tailed distribution. GFR (mL/min) 80 p=n.s. Proteinuria (mg/day) 2500 RFR (%) p=0.006 p=0.019 60 2000 Results 60 1500 Fourteen kidney transplant recipients were included in this study, but only 12 completed it: one patient decided to terminate SRL treatment due to clinical intolerance and another presented a rapid decline of renal function and lost the graft before the end of the study (Table 1). Of the 12 patients who finished the study, there were seven men and five women aged between 32 and 72 years. All patients received a cadaveric graft. The follow-up period after transplantation was 25–192 months (mean: 107 months). All patients had been treated with CIs before conversion to SRL (Table 1). Renal function No significant differences were found in serum creatinine before and after conversion (1.97 vs 2.075 mg/dl; P ¼ 0.270). GFR showed a slight but non-significant increase (40 vs 43 ml/min; P ¼ 0.505). The results of renal function are shown in Figure 1. After withdrawal of CI and the introduction of SRL, proteinuria increased significantly (338 vs 1146 mg/24 h; P ¼ 0.006) and RFR decreased significantly (34.84 vs 13.47%; P ¼ 0.019). Urine electrophoresis was performed after conversion in five patients. In these patients, mean total urinary protein excretion was 1621±758 mg/day and mean albumin excretion 1304±800 mg/day (76%). Mean percentages in the a1, a2, b and g fractions were 3.98, 2.94, 7.22 and 9.88%, respectively; the IgG/albumin ratio was 0.15. This corresponds to proteinuria of a predominantly glomerular source. 40 40 1000 20 20 500 0 0 0 before conversion after conversion Fig. 1. This figure depicts functional parameters (n ¼ 12). The glomerular filtration rate (GFR) remained unchanged after conversion from calcineurin inhibitor to sirolimus. However, after conversion, proteinuria significantly increased while renal functional reserve (RFR) significantly decreased. Haemodynamic data The results of functional studies are shown in Figure 2. Data on intrarenal haemodynamics were obtained in five patients. ERPF (248 vs 310.6 ml/min; P ¼ 0.0625) and RBF (337.71 vs 455.63 ml/min; P ¼ 0.0625) are suggestive of an increase after conversion. A tendency towards a decrease of AAR was observed (14.12 vs 10.28 dyne/s/cm5; P ¼ 0.0625), whereas EAR remained unchanged (1.83 vs 1.84 dyne/s/cm, P ¼ 0.68), leading to a trend towards an increase in PG (42.72 vs 46.17 mmHg; P ¼ 0.0625). Furthermore, the filtration fraction (FF) also remained unchanged (14.65 before vs 14.80 after conversion; P ¼ 0.686). Proteinuria after conversion from calcineurin inhibitors to sirolimus RBF (ml/min) 600 GP (mm Hg) p=0.0625 p=0.0625 50 AAR 491 (dyne.sec.cm-5) 18 p=0.0625 EAR 3 (dyne.sec.cm-5) p=n.s. 16 14 500 40 12 2 400 30 300 8 20 200 100 10 10 6 1 4 2 0 0 0 0 before conversion after conversion Fig. 2. Haemodynamic parameters (n ¼ 5). After conversion, afferent arterial resistance (AAR) significantly decreased, leading to a significant increase in renal blood flow (RBF) and intraglomerular pressure (GP). Efferent arteriolar resistance (EAR) remained unchanged. SRL trough concentrations after conversion The mean SRL trough concentration 8 months after conversion was 9.59±3.58 ng/ml. Safety profile Analysis of MAP before and after conversion showed no differences during the study period (98±5 before vs 96±7 mmHg after conversion; P ¼ 0.9). The systolic (135±9 vs 136±7 mmHg; P ¼ 0.9) and the diastolic pressure (80±7 vs 76±9 mmHg; P ¼ 0.2) did not show any differences. Five patients were treated with an ARB, three with an ACEI. During the study period, no changes of ACEI or ARB, or any other antihypertensive treatment were made. There was no correlation between ACEI or ARB treatment on the one hand and increase in proteinuria or change of RFR on the other hand. After withdrawal of CI, plasmatic lipid levels (cholesterol and triglycerides) increased (cholesterol, 176.5 mg/dl before vs 228.83 mg/dl after conversion; P ¼ 0.0001; triglycerides, 124.5 mg/dl before vs 176 mg/dl after conversion; P ¼ 0.019), but only two patients required addition of a new lipid-lowering agent. The Hct level decreased non-significantly (33.4 vs 30.5% before and after conversion, respectively; P ¼ 0.088), and five patients started treatment with darbepoetin. Discussion This is the first study that describes a loss of renal functional reserve and possible haemodynamic changes simultaneously with the increase of urinary protein excretion that accompanies the conversion from CI to SRL treatment in patients with CAD. This suggests these changes to be a possible pathophysiological factor contributing to an increase of proteinuria in these patients. The changes have the potential to explain at least partially the increase of proteinuria after conversion in these patients. Although our study lacks the proof due to failure of achieving allograft biopsies in the majority of patients, we assume that chronic graft dysfunction in our patients is closely linked with the histological changes proprietary to CAN. Recently, in a not perfectly comparable, but similar group of patients with CAD (n ¼ 59, all with graft biopsies), we could show that all but one had signs of CAN [6]. The causes of the development of CAN are multifactorial, immunological and non-immunological. CI-related nephrotoxicity is one of the major causes. In a recent article, Nankivell and colleagues [3] describe the natural course of CAN. In this study, nephrotoxicity, implicated in late ongoing injury, was almost universal after 10 years [3]. As early as 1981, Hostetter and colleagues showed that reduced nephron mass in rats was associated with hyperfiltration [10]. In a recent study, Estorch and colleagues [11] showed that hyperfiltration is prevalent in a considerable number of transplant patients, is associated with proteinuria and can be measured using [51Cr]EDTA and o-[131I]iodohippurate. It is already known that hyperfiltration in association with proteinuria is seen in chronic graft dysfunction and acts as an additional progression factor [12]. Conversion from CI to SRL was accompanied by an increase of urinary protein excretion without significant changes of serum creatinine or GFR. An increase of proteinuria in conversion patients with CAN has also 492 been observed in other studies in adult patients who were converted for CAD, as well as in paediatric kidney transplant patients converted as part of a rescue therapy [6,13]. Butani describes that his patients react favourably to ARB treatment. The present study shows that the change from CI to SRL with a consequent increase of urinary protein excretion is associated with a significant decrease of RFR. Loss of RFR with maintained GFR is observed in states of glomerular hyperfiltration. In order to investigate whether loss of RFR was accompanied by changes of glomerular haemodynamics ERPF, RBF and PG were determined and demonstrated to have a tendency to increase after conversion, whereas AAR decreased. This corresponds to the characteristics of hyperfiltration in the remnant kidney mass model described by Hostetter and colleagues [10]. Cyclosporin produces vasoconstriction in the afferent glomerular arteriole, which increases AAR. The observed decrease of AAR and increase in PG and RBF can be attributed to CI withdrawal. As already stated, CAN patients have reduced functional nephron mass and severe glomerular and tubulointerstitial damage. If AAR decreases in this pathophysiological condition, then PG increases, leading to hyperfiltration and increased urinary protein excretion. Urinary electrophoresis data collected post-conversion suggest that the proteinuria in our patients is of predominantly glomerular origin. An observational study by Ruiz et al. confirms that the proteinuria observed after conversion from CI to SRL is glomerular, which also supports the concept of its glomerular and possibly haemodynamic origin [14]. The therapeutic benefits of CI (cyclosporin and tacrolimus) are limited by acute and chronic nephrotoxicity. Whereas CI treatment for the prevention of rejection alters glomerular haemodynamics and leads to fibrosis and scarring, SRL has a different mechanism of action and exhibits antiproliferative properties [15] without deleterious effects on GFR or RBF [16,17]. Therefore, conversion to SRL treatment is a promising concept in patients with CAD and CI treatment, as shown in a previous study by our group [6], which demonstrated that conversion is only successful in terms of stabilized or improved renal function after 1 year in patients with moderate renal insufficiency and low proteinuria at the time of conversion as a parameter for the degree of structural damage. Therefore, cautious evaluation of patients is required. The data that were collected in this study do not allow any conclusion on the clinical benefit of conversion for the patients reported here. However, long-term outcome beyond 3 years after conversion has not become available yet. Thus, it still remains a field for future studies to determine if short-term improvement of renal function also translates into the long-term benefit of improved graft survival. The study is limited by the fact that direct haemodynamic data are only available in five patients, which renders careful statistical evaluation difficult. However, the data on RFR—available in all patients that completed the study—also support the concept of A. Saurina et al. haemodynamic changes. This study was not designed to evaluate the influence of ACEIs or ARBs on the process of proteinuria in conversion patients. This needs to be determined in another study. The study design does not permit the gathering of long-term data in a large number of patients in order to study the overall safety of conversion to SRL. A large international conversion study is under way and will be published shortly. This study was not designed to exclude that other pathophysiological mechanisms contribute to SRLassociated proteinuria. There are experimental as well as clinical data showing that high lipid levels might be associated with the development or progression of proteinuria [18,19]. Thus, a potential influence of SRL-induced hyperlipidaemia on proteinuria cannot be excluded. In conclusion, the present study describes an association between conversion from CI to SRL treatment in patients with CAD and possible haemodynamic glomerular changes. These changes could explain hyperfiltration and a certain increase in proteinuria after CI withdrawal in patients with CAD. We suggest that—at least until further evidence is available— conversion be performed early and with extreme caution in patients with CAD and pre-existing proteinuria, when glomerular and tubulointerstitial damage is still limited, in order to avoid hyperfiltration, increase of urinary protein excretion and further decline of renal function. Acknowledgements. This study was partially financed by ‘Redes Tematicas de Investigación cooperativa: V-2003-REDC03’ and by ‘Marató TV3 TV 3610’. Conflict of interest statement. None declared. References 1. Pascual M, Theruvath T, Kawai T, Tolkoff-Rubin N, Cosimi B. Strategies to improve long-term outcomes after renal transplantation. N Engl J Med 2002; 346: 580–590 2. Paul LC. Chronic allograft nephropathy: an update. Kidney Int 1999; 56: 783–793 3. Nankivell BJ, Borrows RJ, Chir B et al. The natural history of chronic allograft nephropathy. N Engl J Med 2003; 349: 2326–2333 4. Bosch JP, Saccaggi A, Lauer A, Ronco C, Belledonne M, Glabman S. Renal functional reserve in humans. Effect of protein intake on glomerular filtration rate. Am J Med 1983; 75: 943–950 5. Letavernier E, Péraldi MN, Kreis H, Legendre C. Proteinuria following switch from calcineurin inhibitors to sirolimus: a retrospective study. American Transplant Congress, May 14–19, 2004, Boston 6. Diekmann F, Budde K, Oppenheimer F, Fritsche L, Neumayer HH, Campistol JM. Predictors of success in conversion from calcineurin inhibitor to sirolimus in chronic allograft dysfunction. Am J Transplant 2004; 4: 1869–1875 7. Sapirstein LA, Vidt DG, Mandel MJ, Hanusek G. Volumes of distribution and clearances of intravenously injected creatinine in the dog. Am J Physiol 1955; 181: 330–336 Proteinuria after conversion from calcineurin inhibitors to sirolimus 493 8. Gomez DM. Evaluation of renal resistances with special reference to changes in essential hypertension. J Clin Invest 1951; 30: 1143–1155 9. Fisher Ll, van Belle G. Biostatistics: A Methodology for the Health Sciences. Wiley, 1993 10. Hostetter TH, Olson JL, Rennke HG, Venkatachalam MA, Brenner BM. Hyperfiltration in remnant nephrons: a potentially adverse response to renal ablation. Am J Physiol 1981; 241: 85–93 11. Estorch M, Tembl A, Antonijoan R et al. Evaluation of renal graft haemodynamia by 51Cr-EDTA and o-[131I]iodohippurate: its use in the early diagnosis of glomerular hyperfiltration. Nucl Med Commun 2003; 24: 679–682 12. EBPG Expert Group on Renal Transplantation. European best practice guidelines for renal transplantation. Section IV: longterm management of the transplant recipient. IV.2.3 Chronic graft dysfunction. Non-immune factors. Nephrol Dial Transplant 2002; 17 [Suppl 4]: 11–15 13. Butani L. Investigation of pediatric renal transplant recipients with heavy proteinuria after sirolimus rescue. Transplantation 2004; 78: 1362–1366 14. Ruiz JC, Diekmann F, Campistol JM et al. Evolution of Proteinuria after Conversion from Calcineurin Inhibitors (CNI) to Sirolimus (SRL) in Renal Transplant Patients. A Multicenter Study. American Transplant Congress, Seattle, WA, 2005 15. Kahan BD. The role of rapamycin in chronic rejection prophylaxis: a theoretical consideration. Graft 1998; 1: 93–96 16. Ryffel B, Weber E, Mihatsch MJ. Nephrotoxicity of immunosuppressants in rats: comparison of macrolides with cyclosporin. Exp Nephrol 1994; 2: 324–333 17. Golbaekdal K, Nielson CB, Djurhuus JC, Pedersen EB. Effects of rapamycin on renal haemodynamics, water and sodium excretion and plasma levels of angiotensin II, aldosterone, atrial natriuretic peptide, and vasopressin in pigs. Transplantation 1994; 58: 1153–1157 18. Joles JA, van Goor H, van Der Horst MLC. High lipid levels in very low density lipoprotein and intermediate density lipoprotein may cause proteinuria and glomerulosclerosis in aging female analbuminemic rats. Lab Invest 1995; 73: 912–921 19. Tozawa M, Iseki K, Oshiro C, Ikemiya Y, Takishita S. Triglyceride, but not total cholesterol or low-density lipoprotein cholesterol levels, predict development of proteinuria. Kidney Int 2002; 62: 1743–1751 Received for publication: 3.3.05 Accepted in revised form: 17.10.05