Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
elationship of the Southern
Ca ifornia Sensory Integration Tests,
the Southern California Postrotary
NystagOlus Test, and Clinical
Observations AccoDlpanying
TheOl to Evaluations in
Otolaryngo ogy, Ophtha lllology,
and Audiology: Two Descriptive
Case Studies
(auditory sequential memory, research, sensory integration, testing procedures,
vestibular system)
Charlotte Brasic Royeen
George Lesinski
Sharon Ciani
A prelzmmary investzgation was
conducted into the relatlOnshzp of
the Southern Califorma Sensory
Integration Tests (SCSIT), the
Southern Californza Postrotary
Nystagmus Test (SCPNT), and
c/imcal obsenmtions accompanymg these tests to evaluations in
otolaryngology, ophthalmology,
and audiology. The subjects were
Iwo children with vestibularly
based sensory integratme dysfunction. The results revealed that
David Schneider
there was no agreement between
the results of the SCPNT and the
otolaryngologzcal evaluation.
There was some agreement
between the ophthalmology evaluatzon and the clzmcal observaizons
accompanying the SCSIT. Both
subiects scored poorly m two areas
of auditory process mg. Possible
reasons for these results are discussed as well as implicatzons for
occupational therapy research and
practice.
The Amerzcan Journal of Occupational Therapy
Downloaded From: http://ajot.aota.org/pdfaccess.ashx?url=/data/journals/ajot/930553/ on 06/12/2017 Terms of Use: http://AOTA.org/terms
443
heSouthern California Sensory
Integration Tests (SCSIT), the
Southern California Poslrotary
Nystagmus Test (SCPNT), and
clinical observations accompanying these tests have been developed
by Ayres as a method of evaluating
sensory integrative dysfunction in
learning-disabled children (I, 2).
These diagnostic procedures are
derived from Ayres' theory of sensory integration as proposed in her
book, Sensory Integration and
Learning Disorders (3). A few researchers, such as Ottenbacher (4, 5)
and DeGangi (6) have attempted to
clarify and identify characteristics
of sensory integrative dysfunction
in children.
Other researchers have begun
empirical examinations by correlating the SCSIT to other tests (7).
Kimball (8), correlating the SCSIT
to the Bender-Gestalt, found that,
T
Charlotte Brasic Royeen, M.S.,
OTR, was a Graduate Fellow in
Occupational Therapy, Program
in Occupational Therapy,
Washington University, School of
Medlcme, St. Louis, Missouri,
when this investigation was conducted. She IS now an instructor,
Howard Umversity, Washington,
DC.
George Lesinski, M.D., is Associate Professor of Otolarynology
and Maxillofanal Surgery, UniverSIty of Cincinnati Medical Center, Cincinnati, 0 hlO.
Sharon Ciam, M.A., is Assistant
Professor of Cllmcal Audiology,
University of Cmcinnal1 Medical
Center, Cincmnati, Ohio.
DaVId Schneider, M.D., IS an ophthalmologist, Resident, University
of Cmcmnati Medical Center,
Cincmnati, Ohio.
444
since the Bender-Gestalt could predictchildren's performance only for
certain components of the SCSIT,
the Bender-Gestalt might effectively
serve as a screening device for sensory integrative dysfunction if observations of the child's postural
mechanisms were included. Some
investigators have related the
SCSIT, or components of it, to particular disabilities (7). To ill ustrate,
Stilwell and others, studied postrotary nystagmus (measured by a procedure based upon the SCPNT) as a
function of communication disorders (9). It was found that hyporeactive nystagmus related to disorders of articula tion and language.
Other researchers, using the SCSIT
as a basis for occupational therapy
procedures, compared the relationship between occupational therapy
and physical therapy test scores (10).
They concluded that each discipline's evaluation was important.
With regard to the SCSIT, however, there is an apparent lack of
cooperative research among disciplines interested in the learningdisabled child. Consequently, it is
often difficult to relate characteristics of sensory integrative dysfunction, measured by the SCSIT, the
SCPNT, and clinical observations
accompanying these tests, to data
from other professionals. Moreover,
areas for further research may be
defined more clearly with an interdisciplinary approach to the evaluation of sensory integrative dysfunction in the learning-disabled
child. Therefore, researchers need
to investigate the relationship of
results of the SCSIT, the SCPNT,
and clinical observations accompanying these tests to the results of other
evaluations.
Ayres (II, 12) concl uded tha t particular forms of vestibular system
dysfunction, characterized by hyporeactive nystagmus, could be ameli-
orated by sensory integrative treatment. In consideration of the
importance of a diagnosis of vestibularly based sensory integrative
dysfunction (as revealed by the
SCSIT, the SCPNT, and clinical
observations), the medical specialty
of otolaryngology should be incl uded in an interdisciplinary evaluation. Otolaryngologists have
long been involved in testing of the
vestibular system, particularly since
Baranay first introduced the spinning test in 1907 (13).
More recently, otolaryngologists
use caloric testing with electronystagmography during evaluation of
the vestibular system (14). A study by
Mathog compared normal and abnormal adult male's performance
during caloric and sinusoidal evaluation of the vestibular system (14).
He found that use of the sinusoidal
test, in addition to caloric testing,
revealed a more complete understanding of the vestibular system
than caloric testing alone. Therefore, in order to further examine
occupational therapy procedures
that theoretically examine vestibular system function, the SCPNT
and clinical observations of hypersenitivity to movement and gravitational insecurity will be compared
to results obtained from an otolaryngological examination.
Rotational stimulation of the
horizontal semicircular canal. which
occurs during any spinning test,
excites neurons in the eat's hypoglossei nuclei and nuclei within the
reticular formation near the abducens nucleus; these regions are
thought to be important in oculormotor control (15). Since components of the SCSIT evaluate visual
perception and somE' of the clinical
observations accompanying the
SCSIT evaluate visual-motor integration, ophthalmology could be
used to further examine the SCSIT.
July 1981, Volume 35, No.7
Downloaded From: http://ajot.aota.org/pdfaccess.ashx?url=/data/journals/ajot/930553/ on 06/12/2017 Terms of Use: http://AOTA.org/terms
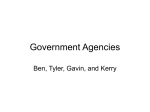
Table 1
SCSIT Standard Scores (s.s.) for Subjects
Subject 1
Age: 6 yr, 11 mo, 21 days
Test
Subject 2
Age: 10 yr, 1 mo, 24 days
5.5.
Test
5.S.
Manual Form Perception
-1.5
Standing Balance: Eyes Closed
Crossing Midline
-1.3
Localization of Tactile Stimuli'
below -4.0
Crossing Midline: Crossed
-1.3
Standing Balance: Eyes Open'
-2.5
Localization of Tactile Stimuli
-1.1
Space Visualization
-2.5
Motor Accuracy: Left
-0.9
Design Copy
-1.6
Standing Balance: Eyes Closed
-0.9
Imitation of Postures'
-1.2
Finger Identification
-0.5
Crossing Midline'
-1.1
G raphesthesia
-0.5
Finger Identification'
-1.1
Standing Balance: Eyes Open
-0.2
Graphesthesia'
-0.8
unable!O perform
Position in Space
-0.1
Motor Accuracy; Left"
-0.7
Motor Accuracy: Right
+0.0
Bilateral Motor Coordination'
-0.7
Kinesthesia
+0.0
Crossing Midline; Crossed'
-0.5
Bilateral Motor Coordination
+0.0
Figure Ground
-0.4
Space Visualization
;-0.0
Kinesthesia'
-0.2
Imitation of Postures
+0.3
Manual Form Perception'
-0.1
Double Tactile Stimuli
+0.5
Right Left Discrimination'
+0.0
Design Copy
+0.9
Motor Accuracy; Right'
...0.1
Figure Ground
;-1.2
Double Tactile Stimuli'
+0.2
Position in Space
+1.0
'Indicates that the score was reported according to how a child aged 8 years-11 months
(the ceiling age on these tests) would score; such scores falling in the low average range
or below suggest deficit areas in a child aged 10 years-1 month.
Tht>refore, results dt>rived from tht>
SCSIT and clinical observations
will be compared toresultsobtained
during an ophthalmological exam.
Audiology is a third area particulelrly relevant to theSCSIT, SCPNT,
and the clinical observations accompanying the tests. Ayres (16)
used an audiologic test, dichotic lis-
tening. with the SCSIT to study ear
advantage in learning-disabled
children. Sht> found that children
with Imv right-left t>ar ratios were
more likely to have language difficulty elnd Jess likely to have ~omat
osensory problems (16). In additional. Ayres routinely used the
dichotic listening test as a diagnos-
tic tool to supplement the SCSIT.
the SCPNT, and clinical observations accompanying these tests (17).
Consequently. audiology was the
third discipline chosen to assess the
results of a sensory integrative
evaluation.
Initial investigation into therelationship of the SCSIT. the SCPNT,
and tht> clinical observations accompanying thest> tests to evaluations in otolaryngology, ophthalmology. and audiology will bt>
explored by studying' two descriptive case studies.
Methods
SubJects. Two leelrning-disabled
children were subjects. Subject I
was referred to occupational therapy because his first grade teacher
felt he was distractible, with problems in visual tracking and language skills. Subject 2 was referred
to occupational therapy because a
psychological evaluation revealed
possible sensory integrillive dysfunction. The parents, who had
initially sought help wht>n informed
that ht> would not pass fifth grade;
felt him to be distractible, passive,
and immature.
An occupational therap) t>valuation indicating vestibularly based
sensory integrative dysfunction WelS
a criterion for subject sekctjon. The
subjt>cts' scores on tht> SCSIT are
presentt>d in Tablt> 1. Finally, parental consent toallow their child to
participate in extensivt> and somewhat time-consuming testing was
another critt>rion for subject se]ection.
Procedure. Subjects were scheduled for evaluations in otolaryngology. ophthalmology, and audiology. EXCt>PI [or occupational
therapy. testing occurred over a 2week period. Occupational therapy
evaluations occurred 5 months
(subject I) and 2 months (subject 2)
The American Ioumal of Occupational Therapy
Downloaded From: http://ajot.aota.org/pdfaccess.ashx?url=/data/journals/ajot/930553/ on 06/12/2017 Terms of Use: http://AOTA.org/terms
445
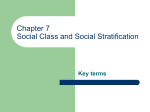
before the testing period. Table 2
presents the specialty area, apparatus used, and method of eval ua tion.
Limitations of the Study. Since
the current study merely initiates
preliminary investigation into the
SCSIT, the SCPNT, and the clinical observations accompanying
these tests, two subjects were used.
As such, only tentative conclusions
can be made.
Inter-rater reliability was not
computed on the more subjective
testing procedures employed by the
different examiners. However. each
occupational therapy evaluation
was performed by a therapist certified in sensory integration, and each
of the other disci pltne's eva Iuations
were performed by licensed professionals.
Analysis of the Data
involvement such asjerky eye tracking, relatively gross tracking and
midline cogwheeling. The right eye
has a persistent pupillary membrane, which has created a mild
amblyopia. Consequently, the subject cannot use both eyes together
well.
Audiology (8/14/79): During 60
trials of the Berlin Dichotic Consonant Vowel Test presented in the
simultaneous condition, the subject
answered correctly 44 times with 29
right ear responses and 15 left ear
responses. The Staggered Spondaic
''''ord Test, the Speech-in-Noise
Test, and the test of Impedance
Audiometry were within normal
limits. However, the subject displayed LOtal inability to perform
during; the Wepman and Morency
Test of Auditory Sequential
Memory.
Results (Subject 1)
Occupational therapy (3127/79):
Inadequate specialization of the
cerebral hemispheres was indicated
by Space Vi'iualization Contralateral Hand Use Score of 27, lack of
agreement for preferred hand and
eye. and marginal skill in the preferred hand. Vestibular system dysfunction was indicated by hyporeactive nystagmus (SCPNT S.s. ::
-1.8), coupled with poor prone extension, and bilaterally involved
postural mechanisms. Evidence indicates poor tactile discrimination
and poor bilateral integration as
well as poor ocular-motor control.
Otolaryngology (8/1/79): There is
no significant spontaneous or
horizontal gaze nystagmus. DixHallpike and position testing were
entirely normal. Hot and cold
caloric testing shovvs no significant
reduced vestibular response or
directional preponderance. This is
essentially a normal ENG.
Ophthalmolog:v (8/1/79): There
are signs of minimal neurological
446
Results (Subject 2).
Occupat1Onai therapy (6/23/79):
Developmental dyspraxia was indicated by a below normal score on
Imitation of Postures, Design Copy
S.s. of -1.6, and marginal skill in use
of both hands on Motor Accuracy.
Such dyspraxia originated from
poor integration of tactile and vestibular information evidenced by
the following. Three of the five tactile tests were significantly low and
the other two were questionable.
Difficulty in processing vestibular
information was evidenced by gravitational insecurity, intolerance to
spinning during the SCPNT (he
would not complete the test after
spinning to the left), inability to
perform Standing Balance wi th Eyes
Closed, and duration of nystagmus
on the SCPNT of 6 seconds after
spinning to the left. The subject
was tactually defensive, had poor
bilateral motor coordination, poor
visual spatial skills, poor ocular
motor control, and inadequate
hemIspheric specialization indicated by a Contralateral Hand Use
'icore on Space Visualization of 26.
Otolaryngology (8/9/79): ENG
testing shows no significant spontaneous horizontal gaze nystagmus.
St<:lndard position testing and Dix
H llpike position testing were negative. Optokinetics and pendular
tracking were symmetrical. Hot and
cold caloric testing demonstrated
no significant reduced vestibular
response or directional preponderance. This was essentially a normal
ENG.
Ophthalmology (8/1179): Normal
ocular pursuits were observed. Some
skipping of the midline while
tracking wi th the eyes was eviden t,
but this was within normal limits.
Mild esophoria was noted, also
within normal limits. Difficulty
with visual acuity was noted with
the Snellen Eye Chart.
Audiology (8/7/79): During 60
trials of the Berline Dichotic Consonant Vowel Test in the simultaneous condition, the subject answered correctly 48 times with 22
right ear responses and 26 left ear
responses, indicating a left ear advantage. The subject could not perform the Staggered Spondaic Word
Test, which indicates a problem
with competing type stimuli. He
performed twice as poorly with his
left ear <:IS he did with his right.
Speech-in-Noi.'ie Test and Impedance Audiometry were within
normal limits. The subject was definitely lacking in the ability LO perform the Wepman and Morency
Auditory Memory Test.
Discussion
Relationship of the SCPNT and
Clmlcal Observations to the OtoLaryngology EvaluatIOn. Inspection
of the data from the evaluations in
occupational therapy and oLOi<:lryng010gy reveals contradictory infor-
July 1981, Volume 35, No.7
Downloaded From: http://ajot.aota.org/pdfaccess.ashx?url=/data/journals/ajot/930553/ on 06/12/2017 Terms of Use: http://AOTA.org/terms
Table 2
Specialty Area, Apparatus Used and Method of Evaluation
Specially Area
Apparatus Used
Method of Evaluation
Occupational Therapy (1, 2, 3, 17)
SCSIT Test Kit
SCPNT Spinning Board
SCPNT Angle Guide
stop watch
Southern California Sensory Integration Tests
Southern California Postrotary Nystagmus Test
Clinical observations of muscle tone, reflex development, ocular and oral motor contrOl,
eyes and hand preference and movement
through space
Developmental history
Otolaryngology (18,19,20)
Electronystagmographic equipment
Film projector and films for
optokinetic testing
Irrigation equipment and temperature
controlled water reservoir for caloric
stimulation
Lights mounted in the ceiling for
eye tracking for calibration
Spontaneous nystagmus (eyes open and eyes
closed)
Standard position testing.
Dix Hallpike position testing
Pendular tracking
Optokinetic nystagmus
Warm and cold caloric testing
Ophthalmology (21)
Snellen Eye Chart
Ophthalmoscope
Snellen Chart of Visual Acuity
Ophthalmoscopic examination
Clinical observations of eye tracing and convergence
History of visual performance
Audiology (20, 22)
Grason Stadler Sudiometer 1701
Berlin Dichotic Consonant Vowel Test
Staggered Spondaic Word Test
Speech in Noise Test
Impedance Audiometry
Wepman and Morency Auditory Memory Span
Test
mation. The SCPNTevaluation on
subject I revealed hyporeactive nystagmus (-1,8 s,s,), whereas the otolaryngology evaluation determined
the subject'S nystagmic response as
within normal limits, Similarly. the
SCPt\'T and clinical observations
revealed Subject 2 as hypersensitive
to movement. gravitationally insecure and demonstratll1g a questionable nystagmic response (6 ,ec).
whereas the oLOlaryng'o)ogy eval uation found the nystagmic response
within normal limits, Consideration of the tests may give insight
ect I) and 2 months (subject 2)
before the testing period, Table 2
presents the specialty area, apparatus used, and method of evaluation,
LzmitatlOns of the Study, Since
the current study merely initiates
preliminary investigation into the
SCSI ,the SCPt fT, and the clinical observations accompanying
these tests. two subjects were used,
As such, only tentatiVt' conclusions
c<ln be made,
Differences in test mechanics
should be considered. The SCPNT.
like the Baranay spinning tesL.
stimulates both of the subject's edrs
simultaneously, but limits caloric
stim ula tion to one ear at a time (20),
The SCPt\'T illlows for visual fixation ,,,ith the subject's eyes opt'n
and the subject positioned in a light
room, Conversely, ENG recorded
nystagmus during caloric stimulation allows for removal of visual
fixation by having the subject close
his eyes while positioned in a dilrkened room; th is allows for a greil ter
and more easily measured nystagmus (20). The SCPNT has the subjecl perform no concentration task
a nd therefore allows for cen tra I
suppression of n) stagmus, During
oto]aryngologicill examination, in
The American Journal of Occupational Thempy
Downloaded From: http://ajot.aota.org/pdfaccess.ashx?url=/data/journals/ajot/930553/ on 06/12/2017 Terms of Use: http://AOTA.org/terms
447
order to minimize central suppression of nystagmus, the subject is
instructed to perform a concentration task aloud (20). Consequently,
the combination of differences in
test mechanics may account for the
discrepant results between evaluations in occupational therapy and
otolaryngology.
The SCPNT measures duration
of nystagmus, whereas electronystagraphy during caloric stimulation
measures amplitude of nystagmus.
During occupational therapy clinical observations, the subjEct's physiological and emotional responses
to movement are monitored. These
aspects are not monitored during
the otolaryngological examination.
Thus, it may be thatduring occupational therapy clinical observations
of a subject's emotional and physiological responses to movement, different aspects of vestibular system
functioning are considered which
are as important as the nystagmic
response for diagnosis of vestibular
dysfunction (23).
Differences in the normative
sample must also be considerEd as
possible reasons for differences in
the occupational therapy and otolaryngology test results. The results
of the occupational therapy Evaluation were com pared to norms developed by Ayres and replicated by
Royeen for children aged five
through nine. (2, 24). Inspection of
some of the research from which
otolaryngology derives normatiVe'
data revealed the youngest subject
to be 19 (25). ConsequEntly. the
otolaryngological evaluation uses
adult norms as a rderence, whereas
the occupational therapy evaluation uses children's norms. This
difference may account for thE discrEpancy bet ween the eval ua tion
results in occupational therapy and
otolarvngology.
Finally, the following statemEnt
448
implies the possibility of caloricrota tional dissocia tion.
Occasionally, the calonc and
rotational test results do not agree.
For example, there may be a rotational directional preponderance
but not a caloric directional preponderance; or there may be a caloric
bilateral weakness but normally intense rota.tional nystagmus. Animal
experiments suggest that such
caloric-rotational dissociation may
b(' a central sign. However, this possibility has not been systematzcally
studied in humans. (25, p 750)
M. H. Stroud found that caloric
abnormalities persisted longEr than
postrotary abnormalities (caloricrotational dissociation) when brainstem lesions were performed on cats
(26).
It is provisionally hypothesized
that a similar phenomenon, dissociation or lack of agreement between
caloric and spinning tests, may also
occur in learning-disabled children
and hence, explain why the results
were discrepant between the otolaryngology and occupational therapyevaluations.
In additional. it should be noted
that the duration of nystagmus as
measured by the SCPNT may, in
fact, have no direetcorrelation with
the vestibular system. Rather, it
may reflect the subject's state of central alerting. anxiety, visual acuity,
and ability to visually fixate and
suppress nystagmus more accura tel y
than it directly measures vestibular
system integrity.
The need for continued research
in this area is the major conclusion
drawn from this discussion regarding the discrepancy betWEen the
evaluation results in occupational
thera py and otolaryngology. A study
with a large enough sample toallow
for statistical analysis investigating
the correlation between caloric test-
ing and the SCPNT is needed. Also,
research investigating the reliability of the SCPNT with a learningdisabled population needs to be
conducted in order to determine if
central alerting and anxiety of the
subject significantly affeer the
SCPNT's reliability. In conjunction
with otolaryngologists, occupational therapy researchers may develop normative data and operationally define procedurES for
measurement of hypersensitivity to
movement (physiological response)
and gravitational insecurity (emotional response) to movemen t.
Finally, norms for children teqed
by caloric stimulation may be
further developed
Relationship of the SCS1T and
Clinica.l ObseriJatzons to the Ophthalmology Eva luations. Genera]] y,
there was agreement between the
occupational therapy and ophthalmology evaluation concerning
Subject I, and disagreement between the evaluations concerning
Subjecr 2. Occupational therapy
clinical observations of Subject I
revealed poor ocular motor control
as evidenced by his inability to
smoothly cross the midline with his
eyes. In addition, the ophthalmological Evaluation revealed that the
subject could not smoothly track an
object across the horizontal plane
with his eyes, and that the subject
was probably ambloyopic due to a
persistant pupillary membrane in
his right eye.
However, consideration of the
evaluation results of Subject 2 disclosed the following discrepancies
between the occupational therapy
and ophthalmology evaluations.
First, occupational therapy clinical
observations revealed that the subJect frequently manifested a midline skip while tracking an object
with his eyes. Ophthalmology evaluation revealed that the subject
July 1981, Volume 35, No.7
Downloaded From: http://ajot.aota.org/pdfaccess.ashx?url=/data/journals/ajot/930553/ on 06/12/2017 Terms of Use: http://AOTA.org/terms
manifested a midline skip but
judged the problem to be within
normal limits. Second, the occupationaltherapy clinical observations
found poor overall quality of the
subject's eye tracking. The ophthalmology evaluation found the subject's eye tracking ability within
normal limits. Third, occupational
therapists clinically observed that
Subject 2 had difficulty with eye
convergence. Conversely, the ophthalmologist determined that the
subject's eye convergence was within
normal limits. Of additional interest was the tentative finding by the
ophthalmologist that Subject 2's
visual acuity was depressed; a full
eye examination was prescribed.
Upon hearing this, the subject's
mother commented. ''I'm surprised,
he is always the first one to read the
road signs." It ma y be tha t the su bject's very poor visual spatial skills,
as indicated during occupational
therapy evaluation of a Space Visualization s.s. of -2.5, affected his
ability to perform visual acuity tasks
as tested by the ophthalmologists.
One explanation for the discrepancies in evaluations by the
opthalmologist and occupational
therapist can be testing error by the
occupational therapist. Or, it may
be that the lack of standardized
norms and consequent use of clinical judgment by the occupational
therapist and the ophthalmologist
allowed them to view the phenomenon differently. What one professional considers abnormal may
be considered normal by the other.
Thus, it may be that in working
with a population of learningdisabled children, occupational
therapists are evaluating and judging very subtle problems, whereas,
the ophthalmologist may be evaluating from a reference point of
pathology and disease. Additionally,
many learning-disabled children are
inconsistent in their responses and
rna y vary in performance from da y
to da y. Such fl uctua tion in performance migh t accoun t for the discrepancy.
Unfortunately, none of these explanations can be appraised empirically due to the lack of experimental data on the subject. Instead,
opera tiona II y defined proced ures of
ocular performance in children may
offer more objective and meaningful information.
Relationship of the SCSIT, the
SCPl\ T, and Clzmcal Observations
Accompanyzng These Tests to the
Audzology EvaluatlOn. Among the
auditory tests administered, both
subjects performed poorest during
the Wepman and Morency test of
Auditory Sequentiall\1emory. Subject I could not perform the task at
all and Subject 2 scored well below
minus I standard deviation. In considera tion of this, and in consideration of the possible vestibular system dysfunction common to each
subject, the correlation between vestibular system functioning and
auditory sequential memory abilities needs further investigation. The
possibility of such a correlation is
especially important in consideration of recent research by Fishbein
(27). He discovered that young,
learning-disabled children with
relatively strong auditory memory
skills benefited most from an intervention program using braille as a
tactual modality for language instruction. Those learning-disabled
children not benefiting from such
an in terven tion program migh t
display signs of possible vestibular
system dysfunction in conjunction
with poor auditory sequenlJal
memory.
The other auditory test that was
atypical for both subjects was the
Berlin Dichotic Consonant Vowel
Test, which is a form of a dichotic
listening test. Subject one obtained
a righ t to left ear ra tio of 1.9. This is
a very high score tha t can be considered abnormal (28). Subject 2 obtained left to right ear ratio of l.l,
which indicated atypicallateralization of language (17). Results of the
Berlin Dichotic Consonant Vowel
Test on Subject 2 are similar to the
findings of Pettit and Helms, who
reportedthatchildren with language
disorders do not have lateralized
cerebral dominance for language
(29).
In spite of these findings, the
experimental nature of the dichotic
listening test must be remembered;
however, its possible value as a clinical tool must not be underestimated.
This sentiment is summarized as
follows:
Although the dzchotlc listening
testzs primarzly a research tool with
lillie practical application, limited
longitudinal testing, and considerable controversy regarding its interpretation, theoretically it provides a measure of assymetry of ear
perception. Dichotzc lzstemng represents a new approach for investigating hemispheric specialization
and its development in children.
(30, p 28)
Again, consideration of the possible
vestibular system dysfunction common to both subjects, the correlation between vestibular system
functioning and the dichotic listening test, reflecting lateralization of
language, needs to be further
investiga ted.
Implications for Occupational
Therapy
In reflecting upon the results of the
two descriptive case studies. twO
implications for occupational therapists are evident. First. occupational reports delineating the results
The Amerzcan Journal of Occupational Therapy
Downloaded From: http://ajot.aota.org/pdfaccess.ashx?url=/data/journals/ajot/930553/ on 06/12/2017 Terms of Use: http://AOTA.org/terms
449
of evaluations must necessarily incl ude the speci fica tion of the procedures used. Therapists should
understand the tests and clinical
observations they use, as well as
somewhat understand tests used by
those in other disciplines. Therefore, when our findings do not corroborate with the findings of other
disciplines, therapists can begin to
understand why.
Second, therapists need todevelop
continued collaborative research
with other disciplines. Many of the
areas targeted for future research
may be best investigated by an interdisciplinary team. Only by dfec-
REFERENCES
Ayres AJ: Southern California Sensory
Integration Test Manual, Los Angeles:
Western Psychological Services, 1972
2. Ayres AJ: Southern California Postrotary Nystagmus Test Manual, Los
Angeles: Western Psychological Services, 1975
3. Ayres AJ: Sensory Integration and
Learning Disorders, Los Angeles:
Western Psychological Services, 1973
4.0ttenbacher K: Identifying vestibular
system processing in the learning-disabled child. Am J Oceup Ther 32: 217221,1978
5. Ottenbacher K, Watson PJ. Short MA:
Association between nystagmus and
hyporesponsivity and behavioral problems In learning-disabled children.Am
JOccup Ther33:317-322, 1979
6. DeGangi GA, Berk RA, Larsen LA: The
measurement of vestibularly based
functions in pre-school children. Am J
Occup Ther 34:452-459,1980
7. Price A, Gilfoyle E, Myers C (Editors):
Research in Sensory Integration,
Rockville, MD: American Occupational
Therapy Association, 1976
8. Kimball JG: The Southern California
Sensory Integration Tests (Ayres) and
the Bender-Gestalt: A correlative study.
Am J Oceup Ther 31 : 294-298, 1977
9 Stilwell JM, Crowe TK, McCallum L W:
Postrotary nystagmus duration as a
function of communication disorders.
Am J Oceup Ther 32: 222-228, 1978
10. Foppe KB, Brooks C, Gersten JW,
Maxwell S: The relationship between
occupational therapy and physical
therapy test scores in children with
learning disabilities Am J Occup Ther
30 163-166,1976
450
tive communication and research
with other disciplines can occupational therapists achieve their maximum potential.
Summary
This preliminary study investigated
the relationship between the results
of two SCSIT's with the results of
evaluations in the areas of otolaryngology, ophthalmology, and
audiology. Generally. there was little agreement between the evaluation results of otolaryngology and
occupational therapy. Occupational
therapists and ophthalmologists
were in partia I agreement over the
11. Ayres AJ: The Effect of Sensory Integrative Therapy on Learning Disabled
Children: The Final Report of a Research Project, Los Angeles: Center
for the Study of Sensory Integrative
Dysfunction and University of Southern California, 1976
12.Ayres AJ: Learning disorders and the
vestibular system Learning Disabi/11'
18-29, 1978
13 Krynycky A, Mattuci KF: Electronystomography in the examination of the
dizzy patient. Ear, Nose Throat J 58:
41-51, 1979
14. Mathog RH: Testing of the vestibular
system by sinusoidal ang ular acceleration.Acta Otolaryngol74: 96-103, 1972
15. Fukushima Y, Igusa Y, Yoshida K:
Characteristics of responses of medial
brain stem neurons to horizontal head
angular acceleration and electrical
stimulation of the labyrinth in the cat.
Brain Res 120: 564-570, 1977
16. Ayres AJ: Dichotic listening performance in learning disabled children. Am J Occup Ther 31' 441-446,
1977
17. Ayres AJ: Interpreting the Southern
California Sensory Integration. Tests,
Los Angeles: Western Psychological
Services, 1976
18 Ransome J, Holden H, Bull TR (Editors): Recent Advances il1 Otolaryngology, Edinburgh and London: Churchill Livingston, 1973, Chapters 7 and 8
19. Ballinger JJ (Editor): Diseases of the
Nose, Throat and Ear, Philadelphia:
Lea and Febiger, 1977, Chapter 43
20 Bradford LJ (Editor): Physiologic
Measures of the Audio-Vestibular System, New York: Academic Press, 1975,
Chapter 3
results. Considering the results of
audiology and occupational therapy evaluations, particular tests in
audiology were atypical for both
subjects. Reasons for the lack of
agreemen t bet ween eva I ua tions 'were
discussed. Areas of future research
to help resolve the discrepancies
were delineated. Finally, implications for occupational therapy were
presented.
Acknowledgmen ts
Appreciation is extended to Elizabeth NewcombeI', OTR, M.Ed., for
assistance in testing and data analYSIS.
21. Walsh T J: Neuro-ophthalmology: Clinical Signs and Symptoms, Philadelphia: Lea and Febiger, 1978, Chapters
9,10 and 23
22. Keith RW (Editor): Central Auditory
Dysfunction, New York: Grune and
Stratton, 1977, Chapters 1,4,6, and 7
23. Katz J (Editor): Handbook of Clinical
Audiology, Baltimore: Williams and
Wilkins, 1972, pp 480-490
24. Royeen C B: Investigation of the testretest reliability of the Southern California postrotary nystagmus test. Am J
Occup Ther 34: 37 -39: Addendum 34:
215,1980
25. Coats AC: Vestibulometry. In Diseases
of the Nose, Throat and Ear, JJ Ballinger (Editor). Philadelphia: Lea and
Febiger, 1977, pp 725-755
26.Stroud MH, Marovitz WF, Ley ton OC:
Vestibular dysfunction after midline
lesions in the b rai n stem of the cat. Ann
Otolaryngol80: 750-758, 1971
27. Fishbein HD: Braille-phonics: A new
technique for aiding the reading disabled, J Learning Disabil 12: 69-73,
1979
28. Ayres AJ: Cluster analysis of measu res
of sensory integration. Am J Occup
Ther31: 362-366, 1977
29. Pettit JM, Helms SB: Hemispheric language dominance of language-disordered, articulation disordered, and
normal children. J Learning Disabil 12:
12-17,1979
30. Kawar M: The effects of sensorimotor
therapy on children with learning disabilities. In Research in Sensory Integrative Development, A Price, E Gilfoyle,
C Myers, Editors. Rockville, MD: American Occupational Therapy Association, 1976
July 1981, Volume 35, No.7
Downloaded From: http://ajot.aota.org/pdfaccess.ashx?url=/data/journals/ajot/930553/ on 06/12/2017 Terms of Use: http://AOTA.org/terms