Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
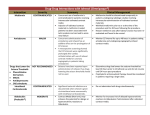
Arch Cardiovasc Imaging. 2014 August; 2(3): e20708. DOI: 10.5812/acvi.20708 Research Article Published online 2014 August 5. Effects of Contrast Media Selection upon Heart Rate and Heat Sensation During Coronary Computed Tomographic Angiography 1 1 1 1 Timothy Roche, MD ; Tyler Kaster, MD ; Rachel Green, BSc ; Yeung Yam, BSc ; Benjamin JW 1,2,* Chow, MD 1Division of Cardiology, Department of Medicine, University of Ottawa Heart Institute, Ottawa, Canada 2Department of Radiology, University of Ottawa, Ottawa, Canada *Corresponding author: Benjamin JW Chow, Division of Cardiology, Department of Medicine, University of Ottawa Heart Institute, Ottawa, Canada, Tel: +1-6137614044, Fax: +16137614929, E-mail: [email protected] Received: May 27, 2014; Accepted: July 26, 2014 Background: Coronary computed tomographic angiography (CCTA) image quality is dependent on heart rate (HR). Beta blockers are commonly administered before CCTA to lower HR and minimize variability. However, contrast media may also impact upon HR and image quality. Since iso-osmolar contrast media induce less vasodilation, this may decrease a patient’s sensation of heat, minimizing patient discomfort and improving HR control and variability. Objectives: The aim of the study was to compare the impact of contrast media selection in CCTA upon HR and image quality. Patients and Methods: A total of 173 patients undergoing CCTA between February and April 2011 were allocated to different contrast media (Iodixanol, Iohexol, and Iopamidol) in 2-week blocks. The groups were analyzed for differences in baseline characteristics, imaging parameters, image quality, HR, and HR variability. Patients were also surveyed for perception of heat. Results: Baseline HR was similar across the patients assigned to Iohexol, Iopamidol, and Iodixanol (65.3 ± 9.7, 66.9 ± 10.9, and 65.3 ± 13.3, respectively; P = NS). Compared to Iohexol and Iopamidol, Iodixanol use was associated with lower HR at the time of image acquisition and immediately after CCTA (53.2 ± 8.0 bpm, 56.3 ± 7.8 bpm, and 56.8 ± 6.5 bpm; P = 0.069 and P = 0.032). A greater proportion of patients achieved HR ≤ 55 beats per minute (bpm) with Iodixanol (63%) than with Iohexol (42%; P = 0.025) and Iopamidol (39%; P = 0.011). As was expected, Iodixanol (2.34 ± 2.02) was associated with a lower perception of heat than Iohexol (6.13 ± 1.89; P < 0.001) and Iopamidol (5.22 ± 2.10; P < 0.001). Image quality was similar in all three groups. Conclusions: Compared to Iohexol and Iopamidol, Iodixanol use was associated with a lower patient perception of heat and lower HR while maintaining similar contrast-to-noise and signal-to-noise ratios. Keywords:Tomography; Coronary Angiography; Contrast Media; Heart Rate; Sensation 1. Background Coronary computed tomographic angiography (CCTA) is a useful noninvasive tool for the detection and exclusion of coronary artery disease (CAD). However, CCTA image quality is dependent on heart rate (HR) control, therefore requiring the use of beta-blockers to target HR ≤ 60 beats per minute (bpm) (1, 2). Beta blockers are not fully effective in all patients; therefore, patients who may barely meet HR control prior to CCTA may be more vulnerable to contrast-induced increases on HR (3, 4). HR may also be influenced by patient discomfort during contrast injection. Though many contrast agents share the same toxicities, some have been associated with less arterial vasodilation (5-7). A heat or warming sensation experienced during intravenous injection of contrast media is common and may cause patient discomfort and anxiety (8). This in turn could increase HR during image acquisition. The sensation of heat varies with differing contrast media, with iso-osmolar media (Iodixanol) producing less heat than low-osmolar me- dia (Iohexol and Iopamidol) (5). Previous studies have documented HR changes with various contrast media during invasive coronary angiography and pulmonary CT angiography (9, 10). However, there are limited studies examining contrast-mediated HR variability and image quality with CCTA (11, 12). 2. Objectives The objective of this study was to compare the impact of contrast media selection in CCTA upon HR and image quality. 3. Patients and Methods 3.1. Study Design As part of an institutional quality assurance evaluation, 197 patients who underwent CCTA over a 6-week period Copyright © 2014, Iranian Society of Echocardiography. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Roche T et al. were screened. A total of 173 patients who were eligible to receive any contrast media were prospectively enrolled in the CT registry and voluntarily completed a heat sensation survey. Over the 6-week study period, the three contrast agents were randomly assigned to 2-week blocks. Both patients and nurses (who administered beta blockers) were blinded to contrast allocation. Patients consented to the cardiac CT registry, and retrospective analysis of CT registry data was approved by the local institutional review board. 3.2. Heart Rate Monitoring Patient history was taken prior to CCTA. Patient vitals were recorded at baseline, immediately prior to CCTA with ECG monitor, during CCTA (imaging HR), and immediately after CCTA (30 sec after CT completion) on ECG monitor. 3.3. Computed Tomography Coronary Angiography Before CCTA, Metoprolol (oral or intravenous) was administered according to a clinical protocol, targeting HR of 55 bpm (1, 13). Additional doses of oral and intravenous Metoprolol were administered according to each patient’s HR response. Nitroglycerin (0.8 mg) was also given sublingually. A biphasic timing bolus method was used for contrast, and a triphasic protocol was used to acquire the final CCTA dataset as previously described by our center (14). Prospective ECG-gated data sets were acquired using a single-source GE Lightspeed Volume CT (GE, Milwaukee, WI) with 64 × 0.625 mm slice collimation, a gantry rotation of 350 ms, and a single-segment temporal resolution of 225 msec. 3.4. Contrast Agents Glomerular filtration rate (GFR) was calculated using the Cockcroft-Gault formula (15). All contrast agents were pre-warmed to the same temperature and administered via 18-G needles. Iodixanol (Visipaque 320, GE Healthcare, Princeton, NJ), Iohexol (Omnipaque 350, GE Healthcare, Princeton, NJ), or Iopamidol (Isovue 370, Bracco Diagnostics, Princeton, NJ) were used as the contrast agents. 3.5. Image Quality CCTA images were post-processed using the iNtuition software (TeraRecon Inc., Foster City, CA), and attenuation values (Hounsfield units [HU]) and standard deviations (SD) were measured to analyze image quality. Signal-to-noise (HUaorta/SDHUaorta) and contrast-to-noise ([HUaorta–HUconnective tissue]/SDHUaorta) ratios for each patient were calculated using a standardized region-of-interest (ROI) method. A ROI was manually drawn in the aortic root (2.0 cm²) and connective tissue immediately outside the left main artery (0.10 cm²). Care was taken in order to avoid the vessel walls, which are known to cause partial volume effects (16, 17). The number of non2 evaluable segments and the amount of CAD per contrast group on CT scans were analyzed as an additional image quality influence. 3.6. Patient Questionnaire Patients were blinded to the contrast media used, and all patients over the course of the 6-week study period were anonymously and voluntarily offered a survey for “heat sensation” using a visual analogue scale (18). The patient marked, on a 10 cm line, their sensation of warmth ranging from “no heat sensation” to “extreme heat sensation” during the IV contrast administration. 3.7. Statistical Analysis A “per-protocol” analysis was performed using SPSS version 19.0 (SPSS Inc, Chicago, IL), and statistical significance was defined as P < 0.05 two-tailed. Continuous variables are presented as means and SDs, and categorical variables are presented as frequencies with percentages. The normality of imaging parameters, image quality, HR, and HR variability was examined using the Quantile-Quantile plot. The one-way ANOVA with the Tukey honestly significance (HSD) post-hoc test was used to compare continuous variables between the three contrasts. The Pearson χ² was used to compare categorical variables. 4. Results 4.1. Patient Demographics A total of 173 patients (49% men, mean age = 58.2 ± 12.2 years, body mass index [BMI] = 30.2 ± 5.6 kg/m², and GFR = 94.2 ± 31.6 mL/min) underwent CCTA and were enrolled in the study (Table 1). Patients with atrial fibrillation or arrhythmia were excluded. Between the three groups, there were no statistically significant differences in age, sex, BMI, GFR, cardiac risk factors, baseline HR, baseline blood pressure, obstructive CAD, and history or prior percutaneous coronary intervention (PCI) or coronary artery bypass graft (CABG). 4.2. Beta-Blocker Administration Chronic and pre-CT beta-blocker use was similar across all three groups (Tables 1 and 2). The dose required per patient receiving IV beta-blockers and the baseline and pre-CT HR were not significantly different between the three groups. 4.3. Computed Tomography Imaging Parameters Although there were significant differences in CT imaging parameters identified between the three contrast media, there were no significant differences in CT imaging parameters between Iodixanol and the other two contrast media using the Tukey HSD post-hoc tests (Table 3). Arch Cardiovasc Imaging. 2014;2(3):e20708 Roche T et al. Table 1. Baseline Patient Characteristics a,b,c All Patients (n = 173) Age, y Iodixanol (n = 56) Iohexol (n = 60) Iopamidol (n = 57) Overall P Value 58.2 ± 12.2 57.8 ± 13.0 55.9 ± 12.4 60.9 ± 10.7 0.608 85 (49) 29 (52) 32 (53) 24 (42) 0.428 30.2 ± 5.6 30.1 ± 4.8 30.2 ± 6.0 30.5 ± 5.9 0.905 83.6 ± 20.5 85.8 ± 24.0 80.0 ± 17.1 85.3 ± 19.9 0.239 94.2 ± 31.6 93.4 ± 27.2 99.5 ± 33.8 89.4 ± 32.9 0.211 86 (50) 28 (50) 31 (52) 27 (47) 0.897 Smoker/Ex-smoker 91 (53) 35 (63) 29 (48) 27 (47) 0.197 Hypertension 105 (61) 38 (68) 32 (53) 35 (61) 0.277 Hyperlipidemia 104 (61) 35 (63) 32 (53) 37 (65) 0.402 Diabetes 22 (13) 6 (11) 6 (10) 10 (18) 0.409 Family History of CAD 77 (45) 20 (36) 30 (50) 27 (47) 0.247 25 (14) 9 (16) 7 (12) 9 (16) 0.750 48 (28) 17 (31) 16 (27) 15 (27) 0.869 33 (19) 11 (20) 9 (15) 13 (23) 0.559 Male Body Mass Index , kg/m² Creatinine, umol/L GFR, mL/min Chronic β-Blocker Use Cardiac Risk Factors Prior Revascularization Obstructive CAD, ≥ 50% b Obstructive CAD , ≥ 70% b a Abbreviations: CAD, Coronary Artery Disease; GFR, Glomerular Filtration Rate. b Based on CT scan results. c Data are presented as mean ± SD or No. (%). Table 2. Pre-Computed Tomography Protocol a,b Iodixanol (n = 56) Iohexol (n = 60) 65.3 ± 13.3 65.3 ± 9.7 66.9 ± 10.9 0.671 132.5 ± 25.6 135.4 ± 19.3 136.9 ± 20.8 0.555 76.7 ± 10.6 78.4 ± 11.0 77.9 ± 9.7 0.667 34 (61) 39 (65) 42 (74) 0.252 62.5 ± 31.1 71.3 ± 36.0 70.1 ± 42.7 0.578 8.3 ± 2.9 19.0 ± 12.9 16.4 ± 9.9 0.339 55 (98) 58 (97) 56 (98) 0.810 Baseline Heart Rate, beats/min Baseline BP Systolic, mmHg Baseline BP Diastolic, mmHg Oral and IV Metoprolol Oral Metoprolol Dose, mg IV Metoprolol Dose, mg Sublingual Nitroglycerin Iopamidol (n = 57) Overall P Value a Abbreviation: BP, Blood Pressure; IV, Intravenous. b Data are presented as mean ± SD or No. (%). Table 3. Computed Tomography Imaging Parameters a Iodixanol (n = 56) P Value b P Value c Iohexol (n = 60) P Value c Iopamidol (n = 57) Overall P Value Average Rate, cc/sec Contrast Volume, cc Tube Current, mA Tube Voltage, kVp 5.8 ± 0.43 0.418 0.199 5.9 ± 0.48 0.008 5.7 ± 0.51 0.011 114.1 ± 19.8 0.557 0.287 117.7 ± 21.5 0.031 108.7 ± 13.3 0.039 687.0 ± 112.3 - - 684.5 ± 105 - 660.6 ± 129.6 0.407 116.1 ± 8.0 0.685 0.180 117.3 ± 6.9 0.024 113.3 ± 9.5 0.029 a Data are presented as mean ± SD. b Compared to Iohexol. c Compared to Iopamidol. Arch Cardiovasc Imaging. 2014;2(3):e20708 3 Roche T et al. 4.4. Heart Rate HR at baseline and after beta-blocker administration was similar in all 3 groups (Table 4). HR at the time of CCTA image acquisition was lower with Iodixanol (53.2 ± 8.0 bpm) than with Iohexol (56.3 ± 7.8 bpm; P = 0.069) or Iopamidol (56.8 ± 6.5 bpm; P = 0.032). Similarly, HR 30 seconds after image acquisition was significantly lower with Iodixanol (58.9 ± 7.1 bpm) than with either Iohexol (64.4 ± 7.8 bpm; P < 0.001) or Iopamidol (62.9 ± 7.2; P = 0.012). The proportion of patients in each group that achieved an imaging HR ≤ 55 bpm was significantly greater with Iodixanol (63%) than with Iohexol (42%; P = 0.025) or Iopamidol (39%; P = 0.011). The difference in achieving HR ≤ 60 with Iodixanol (84%), Iohexol (75%), and Iopamidol (70%) was not significant. HR variability between the three contrast media was similar during image acquisition (Table 4). 4.5. Heat Sensation Since the heat questionnaire was voluntary, the response rate was incomplete but similar between all three groups (Iodixanol [85%], Iohexol [83%], and Iopamidol [88%]). Patients experienced less heat with Iodixanol (2.34 ± 2.02) Table 4. Heart Rate a,b Heart Rate than with Iohexol (6.13 ± 1.89; P < 0.001) or Iopamidol (5.22 ± 2.10; P < 0.001). Moreover, Iopamidol was associated with lower sensation of heat than Iohexol (P = 0.037). 4.6. Image Quality Attenuation of the aorta, signal-to-noise, and contrastto-noise was similar between all contrast media (Table 5). However, noise in the aorta appeared to be lower with Iodixanol (35.6 ± 8.4 HU) when compared to Iopamidol (40.1 ± 10.3 HU; P = 0.039), but no statistically significant difference was observed between Iodixanol and Iohexol. There was no difference in non-evaluable coronary artery segments (P = 0.481) in the groups that received Iodixanol (4.8% [44/919 segments]), Iohexol (5.8% [57.976 segments]), and Iopamidol (8.2% [76.930 segments]). Similarly, no differences were observed in the three groups when patients with history of PCI or CABG were excluded from analysis. On a per-patient analysis (patients without revascularization), patients with ≥ 1 non-evaluable segment appeared to be fewer in Iodixanol group (17.0%; 8.47 patients) than in Iohexol (26.4%; 14.53 patients; P = 0.373) and Iopamidol (31.2%, 15.48 patients; P = 0.169) groups, but statistical significance was not achieved. Iodixanol (n = 56) P Value c P Value d Iohexol (n = 60) P Value b Iopamidol (n = 57) Overall P Value Baseline HR, beats/min 65.3 ± 13.3 - - 65.3 ± 9.7 - 66.9 ± 10.9 0.671 Pre-CT HR, beats/min 57.7 ± 12.2 - - 59.9 ± 8.2 - 59.6 ± 8.7 0.426 Imaging HR, beats/min 53.2 ± 8.0 0.069 0.032 56.3 ± 7.8 0.938 56.8 ± 6.5 0.024 ≤ 55 35 (63) 0.025 0.011 25 (42) 0.736 22 (39) 0.022 ≤ 60 47 (84) - - 45 (75) - 40 (70) 0.221 Post-CT HR, beats/min 58.9 ± 7.1 < 0.001 0.012 64.4 ± 7.8 0.562 62.9 ± 7.2 < 0.001 Image Acquisition 3.3 ± 3.9 - - 3.2 ± 2.6 - 4.7 ± 7.3 0.916 Between Imaging HR and Post-CT HR 6.5 ± 3.0 - - 8.3 ± 4.2 - 6.5 ± 4.9 0.140 HR Variability a Abbreviation: HR; Heart Rate. b Data are presented as mean ± SD. c Compared to Iohexol. d Compared to Iopamidol. Table 5. Image Quality Measures a,b Attenuation Aorta, HU Noise (SD Aorta), HU Signal-to-Noise Contrast-to-noise, aorta Iodixanol (n = 56) P Value c P Value d Iohexol (n = 60) P Value c Iopamidol (n = 57) Overall P Value 443.4 ± 101.1 - - 456.4 ± 111.5 - 471.4 ± 111.6 0.388 35.6 ± 8.3 0.320 0.039 38.2 ± 10.6 0.544 40.1 ± 10.3 0.050 13.0 ± 3.7 - - 12.7 ± 3.8 - 12.3 ± 3.7 0.620 14.6 ± 4.2 - - 14.0 ± 4.0 - 13.4 ± 3.9 0.279 a Abbreviation: HU; Hounsfield Units. b Data are presented as mean ± SD. c Compared to Iohexol. d Compared to Iopamidol. 4 Arch Cardiovasc Imaging. 2014;2(3):e20708 Roche T et al. 5. Discussion Our study demonstrates that Iodixanol, compared to Iohexol and Iopamidol, is associated with lower HR during image acquisition while maintaining image quality with similar contrast-to-noise and signal-to-noise ratios. The lower HR observed with Iodixanol may be due to the decreased perception of heat associated with iso-osmolar contrast agents. Although the discomfort caused by contrast-mediated heat sensation seems harmless, it may impact upon CCTA image quality by increasing HR and thus the likelihood of cardiac motion. As was expected, due to differences in iodine flux between the agents, the perception of heat was much lower with the iso-osmolar contrast medium (Iodixanol) and had lower HR with more patients achieving the target HR ≤ 55 bpm. This is important because studies have found that lower HR improves image quality (13). This improvement in HR control occurred while maintaining image quality despite lower iodine content in Iodixanol. Due to the dependence of CCTA on low and steady HR, effective control of HR is needed. Currently, beta blockers are the preferred medication for lowering HR in CCTA patients (19). Pannu et al. (4) showed that oral beta blockers (Metoprolol) given before CT were effective in lowering HR in 79.4% of patients, but the other 20.6% of patients had no change or an increase in HR during CT. They concluded that beta blockers were ineffective in a proportion of patients. de Graaf et al. (3) found that 16% of patients had contraindications to beta blockers and 27% were unable to achieve target HR despite beta-blocker administration. Given that some patients requiring HR control for CCTA do not respond to beta-blocker administration, identification of other methods such as selection of contrast media that minimize HR variability may improve the diagnostic accuracy of CCTA in these patients. The safety profile of the contrast media is important when selecting the ideal agent for different study populations. Both Iodixanol and Iopamidol, as well as non-ionic agents, are commonly used in patients with renal insufficiency due to their lower risk of nephrotoxicity (20). However, the impact of contrast media selection may affect CCTA in other ways. Previous studies comparing Iodixanol to other contrast media have shown fewer cardiovascular and renal adverse effects, while maintaining diagnostic equivalency (5, 21, 22). Similarly, HR with Iodixanol is lower, but studies have focused on patients undergoing invasive coronary angiography or pulmonary embolism studies, which are less dependent on HR (9, 10, 23). HR is an important factor in CCTA image quality, and minimizing patient-dependent factors such as anxiety and discomfort is desirable. By reducing heat sensations, one may be able to minimize HR changes and patient motion, which are relevant to single-source CT scanners with limited temporal resolution. Therefore, selection of the ideal contrast agent may involve more than considering its safety profile and also include its effects on HR and patient comfort. Previous intra-arterial studies have examined HR variability with difArch Cardiovasc Imaging. 2014;2(3):e20708 ferent contrast media (11, 12). Becker et al. (12) showed no difference in HR when Iomeprol-400 and Iodixanol-320 were used. Conversely, Svensson et al. (11) demonstrated that HR was lower with Iodixanol-320 and was associated with less arrhythmia and heat sensation. Our study differs by demonstrating that Iodixanol was associated with lower HR and heat sensation when compared to Iohexol and Iopamidol while maintaining similar image quality and signal-to-noise ratios. 5.1. Limitations This was a small single-center study and further validation is required. Patients were not randomized to the different agents but the use of contrast agents was allocated in 2-week blocks. Although this design exposes the population to selection biases, there was no significant difference in baseline characteristics between the groups. Furthermore, since the heat sensation questionnaire was voluntary, not all patients responded; however, the response rate was similar across the three groups. HR < 60 is optimal for single-source scanners since it permits the use of prospective ECG triggering, thereby minimizing patient radiation dose. Though HR may be lower with Iodixanol use, its impact upon diagnostic accuracy and at centers with access to dual-source CT scanners is unknown. Although the study examined contrast:noise and signal:noise ratios associated with the different agents, the study did not assess the impact of the contrast agent type on diagnostic accuracy. Compared to Iohexol and Iopamidol, Iodixanol use was associated with a lower patient perception of heat and lower HR while maintaining similar contrast-to-noise and signal-to-noise ratios. Choice of contrast agents may be important in studies requiring low HR. Authors' Contributions All authors have read and approved the manuscript. Timothy Roche and Benjamin Chow: conception and design, acquisition of data, analysis and interpretation of data, drafting of the manuscript, critical revision of the manuscript for important intellectual content, statistical analysis. Timothy Roche had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analyzed. Tyler Kaster and Rachel Green: analysis and interpretation of data, critical revision of the manuscript for important intellectual content, technical support. Yeung Yam: analysis and interpretation of data, critical revision of the manuscript for important intellectual content, statistical analysis, administrative, technical, or material support. Yeung Yam had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analyzed. Financial Disclosure Benjamin Chow receives research support from GE Healthcare and educational support from TeraRecon Inc. 5 Roche T et al. Funding/Support Benjamin Chow is the Saul and Edna Goldfarb Chair in Cardiac Imaging. This study was supported in part by the Ontario Research Fund: Imaging for Cardiovascular Therapeutics. References 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. 6 Abbara S, Arbab-Zadeh A, Callister TQ, Desai MY, Mamuya W, Thomson L, et al. SCCT guidelines for performance of coronary computed tomographic angiography: a report of the Society of Cardiovascular Computed Tomography Guidelines Committee. J Cardiovasc Comput Tomogr. 2009;3(3):190–204. Leschka S, Wildermuth S, Boehm T, Desbiolles L, Husmann L, Plass A, et al. Noninvasive coronary angiography with 64-section CT: effect of average heart rate and heart rate variability on image quality. Radiology. 2006;241(2):378–85. de Graaf FR, Schuijf JD, van Velzen JE, Kroft LJ, de Roos A, Sieders A, et al. Evaluation of contraindications and efficacy of oral Beta blockade before computed tomographic coronary angiography. Am J Cardiol. 2010;105(6):767–72. Pannu HK, Sullivan C, Lai S, Fishman EK. Evaluation of the effectiveness of oral Beta-blockade in patients for coronary computed tomographic angiography. J Comput Assist Tomogr. 2008;32(2):247–51. Spencer CM, Goa KL. Iodixanol. A review of its pharmacodynamic and pharmacokinetic properties and diagnostic use as an x-ray contrast medium. Drugs. 1996;52(6):899–927. McCullough PA, Bertrand ME, Brinker JA, Stacul F. A meta-analysis of the renal safety of isosmolar iodixanol compared with low-osmolar contrast media. J Am Coll Cardiol. 2006;48(4):692–9. Shahbazian H. A comparison between ionic and nonionic contrast nephropathy among high risk patients candidate dor coronary angiography. Jundishapur J Nat Pharm Prod. 2006;1:53–6. Singh J, Daftary A. Iodinated contrast media and their adverse reactions. J Nucl Med Technol. 2008;36(2):69–74. Chartrand-Lefebvre C, White CS, Bhalla S, Mayo-Smith WW, Prenovault J, Vydareny KH, et al. Comparison of the effect of lowand iso-osmolar contrast agents on heart rate during chest CT angiography: results of a prospective randomized multicenter study. Radiology. 2011;258(3):930–7. Tveit K, Bolz KD, Bolstad B, Haugland T, Berg KJ, Skjaerpe T, et al. Iodixanol in cardioangiography. A double-blind parallel comparison between iodixanol 320 mg I/ml and ioxaglate 320 mg I/ ml. Acta Radiol. 1994;35(6):614–8. Svensson A, Ripsweden J, Ruck A, Aspelin P, Cederlund K, Brismar BT. Heart rate variability and heat sensation during CT coronary 12. 13. 14. 15. 16. 17. 18. 19. 20. 21. 22. 23. angiography: Low-osmolar versus iso-osmolar contrast media. Acta Radiol. 2010;51(7):722–6. Becker CR, Vanzulli A, Fink C, de Faveri D, Fedeli S, Dore R, et al. Multicenter comparison of high concentration contrast agent iomeprol-400 with iso-osmolar iodixanol-320: contrast enhancement and heart rate variation in coronary dualsource computed tomographic angiography. Invest Radiol. 2011; 46(7):457–64. Cademartiri F, Mollet NR, Runza G, Belgrano M, Malagutti P, Meijboom BW, et al. Diagnostic accuracy of multislice computed tomography coronary angiography is improved at low heart rates. Int J Cardiovasc Imaging. 2006;22(1):101–5. Chow BJ, Wells GA, Chen L, Yam Y, Galiwango P, Abraham A, et al. Prognostic value of 64-slice cardiac computed tomography severity of coronary artery disease, coronary atherosclerosis, and left ventricular ejection fraction. J Am Coll Cardiol. 2010;55(10):1017–28. Cockcroft DW, Gault MH. Prediction of creatinine clearance from serum creatinine. Nephron. 1976;16(1):31–41. Ferencik M, Nomura CH, Maurovich-Horvat P, Hoffmann U, Pena AJ, Cury RC, et al. Quantitative parameters of image quality in 64-slice computed tomography angiography of the coronary arteries. Eur J Radiol. 2006;57(3):373–9. Pflederer T, Rudofsky L, Ropers D, Bachmann S, Marwan M, Daniel WG, et al. Image quality in a low radiation exposure protocol for retrospectively ECG-gated coronary CT angiography. AJR Am J Roentgenol. 2009;192(4):1045–50. Price DD, McGrath PA, Rafii A, Buckingham B. The validation of visual analogue scales as ratio scale measures for chronic and experimental pain. Pain. 1983;17(1):45–56. Mahabadi AA, Achenbach S, Burgstahler C, Dill T, Fischbach R, Knez A, et al. Safety, efficacy, and indications of beta-adrenergic receptor blockade to reduce heart rate prior to coronary CT angiography. Radiology. 2010;257(3):614–23. Rutten A, Prokop M. Contrast agents in X-ray computed tomography and its applications in oncology. Anticancer Agents Med Chem. 2007;7(3):307–16. Aspelin P, Aubry P, Fransson SG, Strasser R, Willenbrock R, Berg KJ, et al. Nephrotoxic effects in high-risk patients undergoing angiography. N Engl J Med. 2003;348(6):491–9. Jo SH, Youn TJ, Koo BK, Park JS, Kang HJ, Cho YS, et al. Renal toxicity evaluation and comparison between visipaque (iodixanol) and hexabrix (ioxaglate) in patients with renal insufficiency undergoing coronary angiography: the RECOVER study: a randomized controlled trial. J Am Coll Cardiol. 2006;48(5):924–30. Bergstra A, van Dijk RB, Brekke O, Buurma AE, Orozco L, den Heijer P, et al. Hemodynamic effects of iodixanol and iohexol during ventriculography in patients with compromised left ventricular function. Catheter Cardiovasc Interv. 2000;50(3):314–21. Arch Cardiovasc Imaging. 2014;2(3):e20708