Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
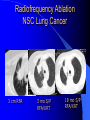
SPNs and the Early Detection of Lung Cancer George Erbacher D.O., FAOCR Chair imaging/interventional radiology OSUMC Radiology residency program director DEFINITION OF SOLITARY PULMONARY NODULE (SPN) Single round water density mass < 3 cm Completely surrounded by lung parenchyma Incidental finding 0.2% CXRs, 1% CT MIMICS OF SPN Chest wall lesion Healing rib fracture AVN Abscess Pneumonia Immune-RA/Wegeners granulomatosis etc. MIMICS OF SPN Hematoma Lung infarct/atelecatasis Pleural plaque Bronchial atresia/Sequestration Inhaled FB MOST COMMON: BENIGN GRANULOMA/HAMARTOMA PATIENT FEATURES INCREASING RISK OF MALIGNANCY SMOKING ESPECIALLY >20 PK/YEAR Older age Personal history of malignancy First degree relative with lung cancer Asbestos/uranium/radon exposure Other workplace exposure- some aromatic hydrocarbons, coal mines etc. IMAGING FEATURES BENIGN VS. MALIGNANT Smaller less risk of malignancy Well defined borders tend to be benign If a cavity –thin walls-favor benign Popcorn like calcification –benign – characteristic of hamartoma Density (HU) < 15-20 benign Very fast and very slow growing lesions are likely benign-PREVIOUS COMPARISON IMAGES ARE CRITICAL Epidemiology Lung Cancer in the World Most frequently diagnosed cancer (1.04M in 1990) Leading cause of cancer mortality – 921K deaths Most common cancer in males and #1 cause of cancer death Incidence Lung Cancer in U.S. 171,600 cases diagnosed in 1999 (94K M; 77.6K F) Leading cause of cancer death M & F (158.9K) Kentucky highest mortality rate – 67.9/100K (37% above avg.) Utah lowest mortality rate – 21.6/100K (56.4% below avg.) U.S. Lung Cancer “Lung cancer is the leading cause of cancer mortality in the U.S. among both men and women surpassing totals from breast, colon, and ovarian cancers combined.” [1] 1Dupuy, DE. Percutaneous radiofrequency ablation of pulmonary malignancies: combined treatment with brachytherapy. Am J Roentgenol. 2003;181(3):711-5. Survival 5 years – 14% 50% survive if diagnosed in early stage (small size IA 85 – 100% survival Only 15% diagnosed in early stage Tobacco Smoke “Cigarette smoking is causally related to lung cancer…the magnitude of the effect far outweighs all other factors.” Is leading cause of avoidable mortality in US, w/ about 434K preventable deaths per year Cost to US economy $200 billion/year US surgeon general CXR Screening Revisited Analysis of the 4 RCT from 20 years ago (Mayo, Czech, Sloan-Kettering, JohnsHopkins) Czech & Mayo studies found increase in mortality in screened vs. controls (6% increase in Mayo) however 29% MORE lung cancer in screening vs. controls CXR Screening Revisited Screened had 34% living @ 5yrs vs. 15% control (Sloan-Kettering, Johns-Hopkins similar results) “Analysis of the randomized trials strongly suggests CXR screening is superior to no screening whatsoever” Low Dose CT (LD CT) Screening vs. CXR Rationale:LD CT greatly increases detection of small non-calcified nodules and of lung cancer at an earlier/more curable stage LD CT showed non-calcified nodules 3x more commonly LD CT showed malig. tumors 4x more commonly LD CT showed stage 1 tumors 6x more commonly LD CT Indication (ELCAP) > 60 y.o.a. > 10 pk/y smoker & no previous cancer Medically fit to undergo thoracic surgery Baseline LD CT, then annuals ELCAP Technique – Helical CT 140 kVp, 40 mA 2:1 Pitch, 10 mm slice thickness Scan entire lung in 1 breath hold @ end inspiration after hyperventilation Reconstruct images with bone algorithm in overlapping 5 mm increments Only lung windows (W1500, L-650) reviewed ELCAP Scoring 1-6 non-calcified nodules = positive If no non-calcified nodules = negative > 6 non-calcified nodules, diffuse bronchiectasis, ground glass opacities or combinations = diffuse disease ELCAP Nodule Description Size (L & W/2) Location (lobe & distance from pleura) peripheral if w/in 2 cm costal margin Benign calcifications Shape (round, non-round) Edge (smooth, non-smooth) ELCAP “Benign Nodule” Benign calcifications Smooth edges < 20 mm size Guideline for Diagnostic Intervention ELCAP Non-benign nodule on LD CT goes to diagnostic CT w/ high resolution imaging of abnormalities. If not benign per above criteria: – < 5mm : F/U high res CT 3 mo, 6 mo, 12 mo, 24 mo; no growth over 3 yrs=benign – 6-10 mm : bx, if not possible F/U per above – > 11mm : bx Fleishner Recommendations do NOT apply to patients: <35 Y.O.A. with low risk of lung cancer Who have fever/signs of infection Fleishner Nodule CT Reassessment Recommendations NONCONTRAST THIN COLLIMATION LIMITED COVERAGE-JUST REGION OF INTEREST LOW DOSE Nodule Enhancement and metabolism Cancer/Infection/inflammation- CT neovascularity- malignant nodules enhance > 20 Hounsfield Units (HU), benign < 15 HU Cancer/Infection/inflammation- increased glucose turnover- PET- SUVmax < 2.5 benign PET/CT HAS SENSITIVITY AND SPECIFICITY CLOSE TO 90% FOR NODULES 10 MM OR GREATER DIAMETER PET/CT vs. Helical dynamic CT for SPN PET/CT MORE SENSITIVE (96% vs. 81%) and MORE ACCURATE (93% vs. 85%) than helical dynamic CT Caveats for PET/CT: NO STANDARIZATION FROM ONE MACHINE TO ANOTHER AND POOR STANDARDIZATION OFTEN BETWEEN EXAMINATIONS ON THE SAME MACHINE. EXPERIENCE OF TECHNOLOGISTSRADIOLOGISTS VARIES WIDELY Benign? NM in Lung Cancer Role of PET in Lung Cancer Improves staging by ruling out mediastinal/distant disease Useful in evaluating response to therapy Useful in early detection recurrent disease Rad Clinics N.A. May 2000 p. 523 False Positive and Caveats PET/CT Active necrotizing granulomas and some chronic inflammatory conditions are + ANY PROCESS THAT HAS INCREASED UPTAKE OF GLUCOSE IS PET POSITIVE What to do with Indeterminant CT W/U of SPN Serial radiographic F/U? CT alone to decide to surgerize or not? PET/CT Surgery for pts w/ + or indeterminant CT? Cost Effectiveness Radiographic F/U cost effective when probability of malignancy is low (<0.14) CT alone F/U cost effective when probability of malignancy is high (.71 - .91) Surgery alone is most cost effective when probability of malignancy is very high > .90 Over greatest range of probability .14 - .71 CT and PET/CT cost effective Rad Clinics N.A. May 2000 p. 521-522 PRINCIPLES OF IMAGING IN ONCOLOGY Imaging justified only if results will change therapy with patient benefit “Where there is an issue get tissue”-biopsy when imaging is inconclusive (imaging guided?) Positive studies are more valuable/reliable than negative studies The diagnostic plan should progress logically from least to most invasive studies Accurate assessment of initial disease extent is vital to selecting and sequencing appropriate treatment Staging lung cancer Stage 1A-T1N0MO= tumor < 3cm with no positive nodes and no metastasis Stage 1B-T2N0M0- tumor > 3cm, no nodes, no metastasis RFA in Pulmonary Applications Lung 25% of patients are candidates for lung resection. [1] RT and chemotherapy together have a combined 5 year survival rate of 5%. [1] RF ablation can potentially provide direct cytoreduction, which could make RT and chemotherapy more effective. [1] 1Dupuy, DE. Percutaneous radiofrequency ablation of pulmonary malignancies: combined treatment with brachytherapy. Am J Roentgenol. 2003;181(3):711-5. Lung Cancer Assessment of malignancy has required invasive diagnostic methods – Needle biopsy (10% sampling error; 15% pneumothorax) – Bronchoscopy (low sensitivity; occ. pneumothorax – Mediastinoscopy (surgical procedure; limited to anterior mediastinum) – Thoracotomy (open surgery; 1-3% mortality) FDG-PET expensive and not widely available Lung Cancer “The overall 5-year survival rate for all stages combined is only 15%.” [1] “Radiofrequency ablation of lung tumors may be a promising option for nonsurgical candidates given the suboptimal outcomes with current treatment options.” [1] 1Dupuy, DE. Percutaneous radiofrequency ablation of pulmonary malignancies: combined treatment with brachytherapy. Am J Roentgenol. 2003;181(3):711-5. Radiofrequency Ablation NSC Lung Cancer 3 cm RFA 3 mo S/P RFA/XRT 18 mo S/P RFA/XRT KEYS Excellent H&P Find Comparisons Send the above to your radiologist then call and discuss the case-have the radiologist lay out the work up as local resources dictate what will be done IF PATIENT CANDIDATE FOR TREATMENT TISSUE DIAGNOSIS IS NEEDED We at Diagnostic Imaging Associates are happy to help FOR TULSA REFERRAL AREA CALL 918 599 5050/5094 TO TALK TO RADIOLOGIST FOR OUTSIDE TULSA REFERRAL AREA CALL CHRISTA -918 599 5031 and ask for radiologist at site nearest you Thank You