Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Remote ischemic conditioning wikipedia , lookup
Saturated fat and cardiovascular disease wikipedia , lookup
Electrocardiography wikipedia , lookup
Cardiovascular disease wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Drug-eluting stent wikipedia , lookup
Cardiac surgery wikipedia , lookup
History of invasive and interventional cardiology wikipedia , lookup
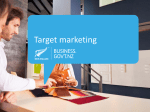
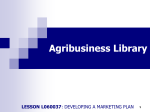
533 Recovery-Phase Patterns of ST Segment Depression in the Heart Rate Domain Identification of Coronary Artery Disease by the Rate-Recovery Loop Peter M. Okin, MD, Olivier Ameisen, MD, and Paul Kligfield, MD Downloaded from http://circ.ahajournals.org/ by guest on June 11, 2017 Although the time course of ST segment depression after exercise has been related to the presence and severity of coronary artery disease, recovery-phase patterns of ST segment depression with reference to changing heart rate have not been quantified. We have found distinct recovery loop patterns of ST segment depression that distinguish subjects without coronary disease from patients with coronary artery disease when ST segment depression is examined in the heart rate domain. Continuous plots of ST segment depression and heart rate were constructed throughout treadmill exercise and recovery in 100 clinically normal subjects, in 124 patients with coronary artery disease proven by catheterization, and in 17 patients with no significant coronary disease at catheterization. Among clinically normal subjects, 95% (95 of 100) had normal (clockwise) rate-recovery loops, and 5% (five of 100) had abnormal (counterclockwise) rate-recovery loops. In these normal subjects, the resulting 95% specificity of a normal rate-recovery loop was similar to the 93% (93 of 100) specificity of standard end-exercise ST segment depression criteria. Among patients with coronary disease proven by angiography, 93% (115 of 124) had abnormal (counterclockwise) rate-recovery loops, and 7% (nine of 124) had normal rate-recovery loops. In contrast was the significantly lower 74% (92 of 124) sensitivity of standard ST segment criteria (p<0.001 vs. the rate-recovery loop). Specificity of a normal rate-recovery loop (71%, 12 of 17) and standard ST segment depression criteria (71%, 12 of 17) were similar in the patients with normal coronary arteries at angiography. We conclude that the pattern of ST segment depression as a function of heart rate during exercise and recovery can markedly enhance the accuracy of the exercise electrocardiogram for the identification of coronary artery disease. (Circulation 1989;80:533-541) E a xercise electrocardiography remains the most widely used method for assessing the presence and severity of coronary artery disease.'-4 Because of the poor sensitivity of standard ST segment depression criteria at end exercise alone for the identification of coronary disease,5,6 additional diagnostic information has been sought from the time course and magnitude of ST segment depression during the postexercise recovery phase.2,7-14 Simple evaluations of the duration of ischemic ST segment responses into recovery,8-12 as well as complex algorithms that depend on the magnitude, slope, and duration of ST segment depression throughout exercise and recovery,2,7,13'14 have been reported to enhance test accuracy. From the Division of Cardiology, Department of Medicine, The New York Hospital-Cornell Medical Center, New York, New York. Address for correspondence: Dr. Okin, Division of Cardiology, Department of Medicine, The New York Hospital-Cornell Medical Center, 525 East 68th Street, New York, NY 10021. Received January 26, 1989; revision accepted May 2, 1989. Recent work has also shown the ability of heart rate-adjusted indexes of ST segment depression during exercise to improve the accuracy of the exercise electrocardiogram for identifying coronary disease and assessing its severity.'5-23 Although patterns relating ST segment depression to heart rate during exercise and recovery were described in early reports from Bruce and colleagues,24-28 the potential diagnostic value of heart rate-dependent behavior of ST segment depression during recovery has not been quantified.29 Based on these observations, we examined whether or not distinct recovery-phase patterns of ST segment depression, in relation to heart rate rather than time, could separate patients with and without coronary disease more accurately than standard end-exercise criteria or time-dependent ST segment changes during recovery. Methods Study Population The records of 241 patients who underwent exercise electrocardiography at The New York Hospital- 534 Circulation Vol 80, No 3, September 1989 Downloaded from http://circ.ahajournals.org/ by guest on June 11, 2017 Cornell Medical Center were reviewed. Clinical data and exercise-phase electrocardiographic findings of a smaller subset of these patients have previously been reported in detail.21,23 The first group (clinically normal) consisted of 100 consecutive, asymptomatic, unmedicated subjects referred by their physicians for exercise electrocardiography as part of a comprehensive screening evaluation or as a precautionary evaluation before beginning an exercise program.23 There were 81 men and 19 women whose mean age was 47±+13 (SD) years. Each had normal findings on cardiac examination and resting electrocardiogram before exercise; no subject was included in this group if exercise systolic blood pressure exceeded 210 mm Hg or if exercise was limited by chest pain. The second group (stable angina) consisted of 141 consecutive patients with effort-related chest pain referred to The New York Hospital-Cornell Medical Center for diagnostic coronary arteriography, who underwent exercise testing at the time of hospital admission as part of a prospective evaluation of the ST segment/heart rate slope for the identification of anatomically extensive coronary obstruction.21 Patients with coexisting valvular heart disease, left bundle branch block on the resting electrocardiogram, myocardial infarction within 8 weeks of arteriography, or unstable angina were excluded from this group. There were 111 men and 30 women in this group whose mean age was 57±9 years; 124 had coronary disease, and 17 had no significant coronary disease (by 50% luminal obstruction criteria). In this group, 28% (40 6f 141) had a history of remote myocardial infarction, and 16% (23 of 141) had electrocardiographic evidence of a previous Q wave myocardial infarction. There were 23 patients in this group who were not receiving medications; among the remaining 118 patients, 92 were taking /3-blocking drugs, 79 were taking nitrates, 76 were taking calcium channel blocking drugs, and only five were taking a digitalis preparation at the time of exercise evaluation. Exercise Electrocardiography Exercise electrocardiograms were performed on a treadmill with a Computer Assisted System for Exercise (CASE II) (Marquette Electronics, Milwaukee, Wisconsin), modified by the addition of a bipolar CM5 lead to the standard 12-lead recording system. All patients exercised according to the Cornell protocol, our more gently graded modification of the Bruce protocol that produces small heart increments between stages, with alternate stages of the Cornell protocol directly comparable with standard Bruce protocol workloads.30 Age-adjusted target heart rates were sought as the exercise endpoint for all studies, but tests were terminated when necessary because of limiting chest pain, dyspnea, or fatigue. As is customary in our laboratory, all patients walked at 1.7 mph at 0% grade for the first 3 minutes of recovery and remained upright through- out the remainder of the period. postexercise recovery Exercise tests were evaluated with standard electrocardiographic criteria measured from the raw intraexercise tracings in each study.9 The test was considered positive in the presence of either 0.1 mV or more of additional downsloping or horizontal ST segment depression, or 0.15 mV or more of additional upsloping ST segment depression, measured between 60 and 80 msec after the J point, at the end of exercise. ST Segment Depression in Relation to Heart Rate and Time In addition to standard electrocardiographic output during exercise, the CASE II provides continuously updated, computer-based measurement of ST segment levels in each lead, based on incremental averaging of normal complexes during exercise. Computer-calculated ST segment amplitudes (both depression and elevation), measured to the nearest 10 ,uV at a point 60 msec after the J point with the end of the PR segment as a reference, were obtained in each lead after each stage of exercise, at peak effort, and after each minute of recovery. Accuracy of this measurement has been previously validated in our laboratory.30 The recovery-phase patterns of ST segment depression with reference to changing heart rate were examined by constructing continuous plots of absolute ST segment deviation and heart rate throughout treadmill exercise and recovery, with both ST elevation and depression values used for analysis. Analysis was performed in the lead with the most ST segment depression at end exercise, but leads aVR, aVL, and V1 were ignored. When no ST segment depression was present, the lead with the least amount of ST segment elevation at end exercise was selected for analysis. ST segment depression was plotted in the upward direction, and ST segment elevation was plotted in the downward direction (Figure 1). The behavior of ST segment depression during recovery with reference to time was evaluated by constructing similar plots of ST segment deviation as a function of the time (in minutes) before and after peak exercise (Figure 2). The time-dependent behavior of ST segment depression in recovery was further analyzed for the presence of persistent ST segment depression 0.1 mV or more at 1 minute into recovery.8-10 Definition of Recovery-Phase Patterns of ST Segment Depression Preliminary observations revealed that clinically normal subjects with ST segment depression at end exercise often exhibited a distinct pattern of recovery-phase ST segment depression as a function of heart rate (Figure 1). Because ST segment depression was lower at early recovery-phase heart rates than at corresponding exercise heart rates, Okin et al Recovery Phase ST Segment Depression CLOCKWISE RATE-RECOVERY LOOP COUNTERCLOCKWISE RATE-RECOVERY LOOP -150 ST DEPRESSION Ji -100 -50_ ST SEGMENT LEVEL 0 (AV) 50k If Exercise 1° Recovery 100 Clinical normal 133-43-74 ST ELEVATION 80 100 120 140 HEART RATE (bpm) 60 Downloaded from http://circ.ahajournals.org/ by guest on June 11, 2017 80 100 120 140 HEART RATE (bpm) there was a clockwise loop of ST segment depression as a function of the heart rate during exercise and recovery. This pattern was defined as a normal rate-recovery loop. In contrast, patients with coronary artery disease often exhibited the opposite pattern of ST segment depression in relation to heart rate: ST segment depression was greater at recovery-phase heart rates than at corresponding exercise heart rates, producing a counterclockwise loop of ST segment depression as a function of the heart rate during exercise and recovery. This pattern was defined as an abnormal rate-recovery loop (Figure 1). As a function of time, rather than heart rate, the recovery-phase pattern of ST segment depression in clinically normal subjects was also generally in a clockwise pattern (Figure 2). This pattern was defined as a normal time-recovery loop. As will be shown, no distinct behavior of ST depression in the time domain emerged for patients with coronary CLOCKWISE TIME-RECOVERY LOOP -150 7 ST DEPRESSION I, -100 -50 ST SEGMENT LEVEL - I Coronary Angiography Selective coronary cineangiography was performed by means of the Judkins technique in all stable angina patients. Multiple views were obtained in all patients, with the left anterior descending and left circumflex coronary arteries visualized in at least four views and the right coronary artery in at least two views. The results were interpreted separately from the original report, specifically for the purpose of our exercise test studies, by a single experienced angiographer using calipers, without knowledge of clinical or exercise test data as previously reported in detail.21'23 CLOCKWISE TIME-RECOVERY LOOP -100F '. I \1 .64 0 o (MV) 50 501 | Exercise t Recovery 100l 100 Clinical normal 132-43-74 ST ELEVATION 6 4 TIME (min) 2 0 FIGURE 1. Plots of STsegment deviation plotted as a function of heart rate during exercise and recovery, with STsegment depression shown in the upward direction and STsegment elevation shown in the downward direction. Typical rate-recovery loops are shownfor a clinically normal subject (left panel) andfor a patient with coronary artery disease (right panel). Despite similar heart rates and magnitude of ST segment depression at peak exercise, the clinically nornal subject had a clockwise pattem of ST segment depression relative to heart rate during recovery, whereas the patient with coronary disease has the opposite, counterclockwise pattern of recovery. 2v-CAD, two-vessel coronary artery disease. disease. Patients with coronary disease exhibited both clockwise and counterclockwise loops of ST segment depression as a function of the time in exercise and recovery (Figure 2). For comparison with findings in the heart rate domain, counterclockwise time-recovery loops were defined as abnormal. -50k I ' -150r 535 2v-CAD 202-50-08 6 4 2 TIME (min) 0 FIGURE 2. Plots of ST segment deviation plotted as a function of time before and after peak exercise in the same clinically normal subject (left panel) and patient with coronary artery disease (right panel) in Figure 1. Although the clinically normal subject had clockwise behavior of recovery-phase ST segment depression in relation to time, the patient with coronary disease also showed a similar clockwise timerecovery loop. 2v-CAD, two-vessel coronary artery disease. 536 Circulation Vol 80, No 3, September 1989 TABLE 1. Group Characteristics and Exercise Performance Clinically normal Characteristic (n = 100) p Age (yr) 47+12 <0.001 Sex (male/female) NS 81/19 <0.001 18+3 Exercise duration Downloaded from http://circ.ahajournals.org/ by guest on June 11, 2017 (min) 93+7 <0.001 Proportion of target rate achieved (%) 164±16 <0.001 Maximum heart rate (beats/min) <0.001 177±21 Maximum systolic pressure (mm Hg) 29+5 <0.001 Maximum double product (xlO 3) (mm Hgx [beats/mini) Data are mean±SD. CAD, coronary artery disease. *Clinically normal subjects vs. CAD by catheterization; catheterization vs. clinically normal subjects. CAD by catheterization (n = 124) 58+9 103/21 9+4 pt NS <0.05 NS No CAD by catheterization (n = 17) 54+10 9/8 11+4 pt <0.05 <0.05 <0.001 66+10 <0.001 76+ 15 <0.001 112±18 <0.001 132+28 <0.001 157±22 NS 161+19 <0.05 18±4 <0.05 21+6 <0.001 tCAD by catheterization Degree of stenosis was defined as the greatest percent reduction of luminal diameter in any view compared with the nearest normal segment. For classification of the number of obstructed coronary arteries, disease was considered significant when 50% luminal obstruction was present. Left main narrowing of 50% or greater was scored as the equivalent of two-vessel disease.1718,21,23 According to these criteria, there were 17 patients with no significant disease, 34 with one-vessel disease, 43 with two-vessel disease, and 47 with three-vessel coronary disease. Ten patients had left main coronary disease, including four with additional twovessel disease and six with additional three-vessel disease. Of note, 96% (119 of 124) of the patients with coronary disease defined by 50% stenosis also had at least 75% luminal obstruction of one or more major vessels. Data Analysis Sensitivity and specificity were calculated accord- ing to standard definitions.31 Test specificity was tested separately in the 100 clinical normal subjects and in the 17 patients with no significant coronary disease at angiography. Test sensitivity was assessed in the 124 patients with angiographically proven coronary disease. Comparison of test performance of standard exercise test criteria and the timerecovery loop with outcome based on the raterecovery loop was performed in each group by McNemar's modification of the x2 method for paired proportions. In addition, sensitivity of each method was compared for patients with demonstrated coronary disease subgrouped by the number of obstructed coronary arteries. Sensitivity of the raterecovery loop was further assessed with patients subgrouped by medication usage and by a history of or electrocardiographic evidence of previous myocardial infarction. vs. no CAD by catheterization; tno CAD by Statistical Analysis Mean values for all findings are reported with the standard deviation (SD) as the index of dispersion. Comparison of mean values among groups was performed by one-way analysis of variance, with post hoc testing of individual group differences by Scheffe's method. Comparison of subgroup proportions was performed by x2 analysis with correction for continuity. For tests of proportion and for post hoc testing of mean values, ap value less than 0.05 was required for rejection of the null hypothesis. Results Group Characteristics and Exercise Perfornance Group characteristics and exercise performance are shown in Table 1. Patients with coronary disease were similar to clinically normal subjects with respect to sex distribution, but there was a higher proportion of women among the catheterized patients with no significant coronary obstruction. Maximum predicted heart rate achieved, peak exercise heart rate, and maximum double product were higher in clinically normal subjects than in the patients without coronary disease, and these were higher in patients with no demonstrated disease at angiography than in those with coronary disease. Patients with coronary disease were older and exercised for a shorter period of time and to lower peak systolic pressures than clinically normal subjects, but they were similar to stable angina patients shown to have no coronary disease by these findings. Test Performance of the Rate-Recovery Loop Test performance for the rate-recovery loop is compared with performance of standard test criteria and time-dependent recovery-phase criteria in Table 2. Among clinically normal subjects, 95% (95 of Okin et al Recovery Phase ST Segment Depression 537 TABLE 2. Sensitivity and Specificity of the Rate-Recovery Loop, Time-Recovery Loop, and Standard ST Segment Criteria Sensitivity CAD by catheterization (n = 124) 93% (115/124) 74% (92/124)t 35% (44/124)t 51% (63/124)t Specificity Clinically normal (n = 100) 95% (95/100) 93% (93/100) 96% (96/100) 99% (99/100) Criteria* Rate-recovery loop Standard ST segment Time-recovery loop ST depression at 1 min recovery CAD, coronary artery disease. *See text for definitions of test criteria. tp<0.001 vs. rate-recovery loop. Downloaded from http://circ.ahajournals.org/ by guest on June 11, 2017 100) had normal (clockwise) rate-recovery loops, and 5% (five of 100) had abnormal (counterclockwise) rate-recovery loops. Of the 95 subjects with clockwise rate-recovery loops, 51 had end exercise ST segment depression ranging from 10 to 180 gV, and 44 had no ST segment depression in any lead at end exercise. Despite the absence of end exercise ST segment depression, all 44 of these subjects had a clockwise pattern of absolute ST segment deviation when changing amounts of ST segment elevation were examined as a function of heart rate during exercise and recovery. In these normal subjects, the resulting 95% specificity of a normal rate-recovery loop was similar to the 93% specificity of standard test criteria, the 96% specificity of a normal (clockwise) time-recovery loop, and the 99% specificity of ST depression persisting at least 1 minute into recovery. Specificity of the rate-recovery loop was 71% (12 of 17) in patients with stable angina who had normal coronary arteries at angiography; specificity was similarly low in this subgroup for both standard and time-dependent recovery criteria (Table 2). In patients with angiographically proven coronary disease, 93% (115 of 124) had abnormal (counterclockwise) rate-recovery loops (Table 2), and all nine patients with false-negative rate-recovery loops had clockwise loops. In contrast was the significantly lower 74% sensitivity of standard test crite- No CAD by catheterization (n = 17) 71% (12/17) 71% (12/17) 82% (14/17) 76% (13/17) ria, 35% sensitivity of an abnormal (counterclockwise) time-recovery loop, and 51% sensitivity of an abnormal test persisting at least 1 minute into recovery (allp<0.001 vs. the rate-recovery loop). Test Sensitivity in Relation to Extent of Coronary Artery Disease Test sensitivities of the rate-recovery loop pattern, standard test criteria, the time-recovery loop pattern, and abnormal ST depression persisting at least 1 minute into recovery are shown in relation to anatomic extent of coronary disease in Table 3. Of note, the rate-recovery loop identified 98% of patients with three-vessel disease, and 93% (84 of 90) of patients with multivessel disease. In contrast, standard test criteria identified only 83% of patients with three-vessel disease and only 82% (74 of 90) of patients with multivessel disease (p <0.05 vs. raterecovery loop). For each test, there was a trend toward increased sensitivity with increasing numbers of obstructed arteries. However, this trend was only modest for the rate- and time-recovery loop criteria. Within each subgroup defined by extent of obstruction, detection of coronary disease by the rate-recovery loop was significantly greater than by the other test criteria, except for similar sensitivity of standard test criteria in patients with two-vessel disease. TABLE 3. Sensitivity of the Rate-Recovery Loop, Time-Recovery Loop, and Standard ST Segment Criteria According to the Extent of Coronary Disease One vessel Criteria* 91% (31/34) Rate-recovery loop 53% (18/34)t Standard ST segment 35% (12/34)§ Time-recovery loop ST depression 24% (8/34)§ at 1 min recovery CAD, coronary artery disease. *See text for definitions of test criteria. Extent of CAD Three vessel Two vessel 88% (38/43) 98% (46/47) Total CAD 93% (115/124) 81% (35/43) 83% (39/47)t 74% (92/124)§ 30% (13/43)§ 40% (19/47)§ 35% (44/124)§ 58% (24/43)t 64% (30/47)§ 51% (63/124)§ tp<0.05 vs. rate-recovery loop; tp<0.01 vs. rate-recovery loop; §p<0.001 vs. rate-recovery loop. 538 Circulation Vol 80, No 3, September 1989 TABLE 4. Effect of Medications on Sensitivity of the RateRecovery Loop for Coronary Disease Medication Medication /3-Blockers Nitrates Calcium blockers present 95% (84/88) 93% (69/74) 94% (66/70) Medication absent 86% (31/36) 92% (46/50) 91% (49/54) Downloaded from http://circ.ahajournals.org/ by guest on June 11, 2017 Effect of Medications and Previous Infarction on Sensitivity of the Rate-Recovery Loop Test sensitivity of the rate-recovery loop in relation to medications used, presence of a Q wave infarction on the resting electrocardiogram, and history of a remote myocardial infarction are shown in Tables 4 and 5. There was no significant difference in the ability of the rate-recovery loop to identify coronary disease among patients who were taking or were not taking ,3-blockers, long-acting nitrates, or calcium channel blockers. Neither electrocardiographic evidence of previous Q wave myocardial infarction nor a history of infarction had a significant effect on the sensitivity of the raterecovery loop, whereas there was a trend toward lower test sensitivity of standard ST segment criteria among patients with a previous infarction. Of note, among patients with coronary disease and negative standard exercise tests, the rate-recovery loop identified 92% (12 of 13) of patients with a history of a myocardial infarction and 100% (seven of seven) of patients with a previous Q wave infarction. Discussion Early observations by Bruce and colleagues24-29 suggest that different heart rate-related postexercise patterns of ST segment depression may occur in individuals with and without coronary disease. Our present data provide quantitative evidence of improved diagnostic performance of these patterns for identifying coronary artery disease. TABLE 5. Effect of Previous Myocardial Infarction on Sensitivity of the Rate-Recovery Loop and Standard ST Segment Criteria for Coronary Disease Electrocardiographic Q wave infarction Present (n=22) Absent (n 102) History of remote infarction Present (n=39) Absent (n=85) *p<0.05 loop. Rate-recovery loop Standard ST criteria 95% (21/22) 92% (94/102) 68% (15/22) 75% (77/102)t 90% (35/39) 67% (26/39)* 94% (80/85) 78% (66/85)t vs. rate-recovery loop; tp<0.01 vs. rate-recovery Recovery-Phase Behavior of ST Segment Depression in the Heart Rate Domain Physiologic correlates of rate-recovery loop patterns can be found in previous observations that compare myocardial ischemia during exercise and recovery. Detry and colleagues28 found a close linear relation of ST segment depression during exercise to myocardial oxygen demand, as reflected by tension-time index, in patients with coronary disease. During recovery, however, this relation was nonlinear, with similar ST segment depressions observed at lower tension-time indexes than during exercise. Also, exercise- or pacing-induced subendocardial ischemia has been well recognized to continue into the recovery phase as shown by persistent ST segment depression associated with continued abnormal lactate production,32,33 regional wall motion abnormalities,34 and diminished subendocardial blood flow to the affected area.35,36 Although these electrocardiographic, metabolic, performance, and perfusion abnormalities may be less severe during early recovery than at peak pacing or exercise,32-36 they remain greater relative to heart rate during early recovery than during the development of ischemia.32,33,36 Although the magnitude of ST segment depression during exercise can be directly related to the level of myocardial workload (as reflected by heart rate) in patients with myocardial ischemia, ST segment depression during early recovery remains greater than expected for the rapidly decreasing myocardial oxygen demand that results from an abrupt lowering of exercise load. In effect, relative to heart rate, recovery-phase resolution of ST segment depression lags behind its exercise-phase development when coronary disease is present. This results in the counterclockwise pattern of ST segment depression in the heart rate domain found in our patients with coronary obstruction. In contrast, rate-related resolution of repolarization change exceeds its exercise phase development in normal subjects, resulting in a clockwise pattern despite ST segment depression at peak effort. Because the rate-recovery loop is based on ST segment changes surrounding peak effort, the direction of rotation is independent of the absolute magnitude of ST depression at end exercise. Therefore, in most cases, the recovery-phase pattern cannot be reliably predicted from exercise-phase data alone. Over half of our normal subjects with clockwise loops had measurable ST depression at the end of exercise that was often similar in magnitude to that found at the onset of the counterclockwise loop pattern in patients with coronary disease. However, all subjects with absolutely no ST depression in any lead at end exercise had clockwise recovery-phase loop patterns when examined in the context of changing amounts of ST segment elevation 60 msec after the J point. Whether or not complete absence of ST depression at end exercise Okin et al Recovery Phase ST Segment Depression Downloaded from http://circ.ahajournals.org/ by guest on June 11, 2017 alone might simply be interpreted as a normal test response remains to be established, but a normal pattern may occur even in cases with later recovery phase ST depression if early recovery-phase behavior in these subjects initiates a clockwise pattern of rotation. Also of note, counterclockwise rate-recovery loops in patients with coronary disease are not simply markers for an increase in ST segment depression during recovery as has been reported in some patients with negative end exercise tests by standard criteria.9,37 An increase in absolute magnitude of ST depression during recovery was seen in only nine of our 124 patients with coronary disease, including one patient who had ST segment depression that exceeded 0.1 mV only during recovery. In these cases, early recovery-phase augmentation of ST depression during heart rate slowing is an obvious indication of counterclockwise rotation. On the other hand, ST depression was less during recovery in the large majority of patients with coronary disease, which was similar to the recovery-phase behavior of ST depression in normal subjects, and distinct rotation only became apparent by construction of the rate-recovery loop. Recovery-Phase Behavior of ST Segment Depression in the Time Domain Unlike the patterns that result from reference to heart rate, distinct recovery-phase behavior of ST segment depression was not found in the time domain. Nearly two thirds of patients with coronary disease had clockwise time-recovery loops that were indistinguishable from the time-recovery loops of most normal subjects. The diagnostic value of recovery loops in the rate domain, but not in the time domain, highlights differences between heart rate and time as estimates of myocardial work in the period surrounding peak exercise. Heart rates at matched times before and after peak exercise are different. If the rate-recovery loop examines ST segment depression during recovery and exercise at approximately matched workloads, as reflected by similar heart rates, it follows that the time-recovery loop relates ST segment depression during exercise and recovery at varying levels of myocardial oxygen demand. Our findings therefore indicate that the time course of ST depression may be an indirect and potentially inaccurate method for evaluating myocardial ischemia. Although the time-dependent pattern of ST segment depression during recovery was not a sensitive criterion for coronary disease in the present study, other methods that incorporate the pattern of ST segment changes as a function of time during the postexercise period have been shown to improve the ability of the exercise electrocardiogram to identify coronary artery disease.2,7'13,14 Whether or not accuracy of these methods might be further enhanced by correction for rate, rather than time, throughout exercise remains to be examined. 539 Improved Identification of Coronary Disease The sensitivity of the rate-recovery loop for coronary disease is similar in magnitude to the improved accuracy of other methods based on heart rate correction of ST segment depression during exercise only.15-23 However, these new methods are different in principle and may provide different types of information. The nonlinear and complex behavior of ST segment depression with respect to heart rate during recovery28 indicates that this relation may be more difficult to quantify than the linear rate-related changes in ST segment depression that occur during exercise in patients with coronary disease.15-23 Thus, although the ST segment/heart rate slope is a continuous variable that can be related to the anatomic and functional severity of coronary obstruction,15-19,21-23 translation of recovery-phase data to a complementary continuous variable may prove difficult. Or the findings support the idea that the raterecovery loop provides diagnostic information distinct from ST segment criteria based on exercisephase findings. Sensitivity of the rate-recovery loop appears to be relatively independent of the extent of coronary artery disease (Table 3), unlike the performance of standard ST segment criteria2,9,10 and heart rate-adjusted ST segment criteria that are derived from exercise-phase data alone.15,23 The strong dependence of the test sensitivity of other electrocardiographic methods on the anatomic extent of coronary disease results from threshold criteria that are directly related to the severity of ischemia induced by exercise.2,9,10,23 In contrast, the direction of the rate-recovery loop is not dependent on any threshold magnitude of ST segment depression at peak exercise; it may thus be less affected by the anatomic and functional severity of underlying coronary artery obstruction than are standard test criteria. Similar reasoning may explain the absence of an effect of cardiac medications or previous myocardial infarction on sensitivity of the rate-recovery loop. /3-Blockers, by blunting the heart rate response to exercise, have been found to reduce the magnitude of ST segment depression at peak exercise38,39 but do not markedly affect the rate-dependent pattern of ST segment depression during recovery. Previous myocardial infarction may also result in a diminished magnitude of ST segment depression with exercise, leading to reduced sensitivity of partition-based standard electrocardiographic criteria.40,41 Remote myocardial infarction does not adversely affect sensitivity of the rate-recovery loop in the present population, but test performance may vary in patients with recent infarction who were excluded from this study.42 Limitations and Clinical Implications Although the present data show that the raterecovery loop is highly sensitive for detecting cor- 540 Circulation Vol 80, No 3, September 1989 Downloaded from http://circ.ahajournals.org/ by guest on June 11, 2017 onary artery disease in patients with stable angina, these findings should not be extrapolated to other populations without caution. Test sensitivity may be lower in asymptomatic subjects with coronary disease, and overall test performance may vary in patients with other chest pain syndromes, such as atypical angina. Test specificity may be lower in patients with other causes of nonischemic ST segment depression than in our clinically normal subjects.23,43X44 These important possibilities require careful evaluation. Further, it must be appreciated that predictive value of a positive rate-recovery loop, like all imperfect diagnostic tests, will vary with the population prevalence of disease.44,45 However, even with potential limitations, the raterecovery loop appears to represent a useful and easily performed method for improving the diagnostic value of the exercise electrocardiogram. Although our data show that the counterclockwise rate-recovery loop is a sensitive marker for coronary artery disease, the relation of these findings to prognostically important myocardial ischemia remains to be clarified. Because we did not measure myocardial ischemia per se, the mechanisms governing the direction of rate-recovery loops in our patients with angina32-36 can only be speculated. Further evaluation is required to examine whether or not the rate-recovery loop can separate myocardial ischemia in patients with coronary disease from abnormal repolarization during exercise in patients with noncoronary heart disease. Expansion of the loop method from a simple vector analysis to a more complex continuous variable that incorporates a magnitude term would be required for comparison with independent measures of the extent of exercise-induced myocardial ischemia. Thus, at present, the rate-recovery loop may best serve as a simple screen for the presence or absence of underlying coronary obstruction. Additional quantitative exercise-phase findings, such as the ST segment/heart rate slope, may be useful in confirming the diagnosis23 and may be required to estimate the extent and severity of disease19,21,46 in these patients. Acknowledgments We are indebted to Drs. Harvey L. Goldberg and Jeffrey S. Borer for providing the angiographic data. References 1. Bruce RA, Hossack KF, Rouen TA, Hofer V: Enhanced risk assessment for primary coronary heart disease events by maximal exercise testing: 10 years' experience of Seattle Heart Watch. JAm Coil Cardiol 1983;2:565-573 2. Hollenberg M, Budge WR, Wisneski JA, Gertz EW: Treadmill score quantifies electrocardiographic response to exercise and improves test accuracy and reproducibility. Circu- lation 1980;61:276-285 3. Sheffield LT: The exercise test in perspective. Circulation 1977;55:681-685 4. Chaitman BR: The changing role of the exercise electrocardiogram as a diagnostic and prognostic test for chronic ischemic heart disease. JAm Coll Cardiol 1986;8:1195-1210 5. Borer JS, Brensike JF, Redwood DR, Itscoitz SB, Passamani ER, Stone NJ, Richardson JM, Levy RI, Epstein SE: Limitations of the electrocardiographic response to exercise in predicting coronary artery disease. N Engl J Med 1975; 293:367-371 6. Epstein SE: Value and limitations of the electrocardiographic response to exercise in the assessment of patients with coronary disease. Am J Cardiol 1978;42:667-674 7. Hollenberg M, Zoltick JM, Go M, Yaney SF, Daniels W, Davis RC, Bedynek JL: Comparison of a quantitative treadmill exercise score with standard electrocardiographic criteria in screening asymptomatic young men for coronary artery disease. N Engl J Med 1985;313:600- 606 8. Lozner EC, Morganroth J: New criteria to enhance the predictability of coronary artery disease by exercise testing in asymptomatic subjects. Circulation 1977;56:799-802 9. Goldschlager N, Selzer A, Cohn K: Treadmill stress tests as indicators of presence and severity of coronary artery disease. Ann Intern Med 1976;85:277-286 10. Chaitman BR, Bourassa MG, Wagniart P, Corbara F, Ferguson RJ: Improved efficiency of treadmill exercise testing using a multiple lead ECG system and basic hemrodynamic response. Circulation 1978;57:71-79 11. McHenry PL, Richmond HW, Weisenberger BL, Rodway JS, Perry GF, Jordan JW: Evaluation of abnormal exercise electrocardiogram in apparently healthy subjects: Labile repolarization (ST-T) abnormalities as a cause of false positive responses. Am J Cardiol 1981;47:1152-1160 12. Simoons ML, Hugenholtz PG: Gradual changes of the ECG waveform during and after exercise in normal subjects. Circulation 1975;52:570-577 13. Barlow JB: The "false positive" exercise electrocardiogram: Value of time course patterns in assessment of depressed ST segments and inverted T waves. Am Heart J 1985;110:1328-1336 14. Neutel JM, Barlow JB, King J, Myburgh DP: The importance of time-course behaviour of ST segment and T wave changes following exercise: A reliable aid towards eliminating "false positives". JAm Coll Cardiol 1988;11:122A 15. Elamin MS, Mary DASG, Smith DR, Linden RJ: Prediction of severity of coronary artery disease using slope of submaximal ST segment/heart rate relationship. Cardiovasc Res 1980;14:681- 691 16. Berenyi I, Hajduczki S, Baszormenyi E: Quantitative evaluation of exercise-induced ST segment depression for estimation of degree of coronary artery disease. Eur Heart J 1984;5:289-294 17. Okin PM, Kligfield P, Ameisen 0, Goldberg HL, Borer JS: Improved accuracy of the exercise electrocardiogram: Identification of three-vessel coronary disease in stable angina pectoris by analysis of peak rate related changes in ST segments. Am J Cardiol 1985;55:271-276 18. Kligfield P, Okin PM, Ameisen 0, Borer JS: Evaluation of coronary artery disease by an improved method of exercise electrocardiography: The ST segment/heart rate slope. Am Heart J 1986;112:589-598 19. Finkelhor RS, Newhouse KE, Vrobel TR, Miron SD, Bahler RC: The ST segment/heart rate slope as a predictor of coronary artery disease: Comparison with quantitative thallium imaging and conventional ST segment criteria. Am Heart J 1986;112:296 -304 20. Detrano R, Salcedo E, Passalaqua M, Friis R: Exercise electrocardiographic variables: A critical appraisal. J Am Coll Cardiol 1986;8:836-847 21. Okin PM, Kligfield P, Ameisen 0, Goldberg HL, Borer JS: Identification of anatomically extensive coronary disease by the exercise ECG ST segment/heart rate slope. Am Heart J 1988;115:1002-1012 22. Okin PM, Kligfield P, Milner MR, Goldstein SA, Lindsay J: Heart rate adjustment of ST segment depression for reduction of false positive electrocardiographic responses to exer- Okin et al Recovery Phase ST Segment Depression 23. 24. 25. 26. 27. 28. 29. 30. Downloaded from http://circ.ahajournals.org/ by guest on June 11, 2017 31. 32. cise in asymptomatic men screened for coronary artery disease. Am J Cardiol 1988;62:1043-1047 Kligfield P, Ameisen 0, Okin PM: Heart rate adjustment of ST segment depression for improved detection of coronary artery disease. Circulation 1989;79:245-255 Detry JMR, Bruce RA: Effects of nitroglycerin on "maximal" oxygen intake and exercise electrocardiogram in coronary heart disease. Circulation 1971;43:155-163 Detry JM, Bruce RA: Effects of physical training on exertional ST segment depression in coronary heart disease. Circulation 1971;44:390-396 Bruce RA: Exercise testing of patients with coronary heart disease: Principles and normal standards for evaluation. Ann Clin Res 1971;3:323-332 Bruce RA, McDonough JR: Stress testing in screening for cardiovascular disease. Bull NYAcad Med 1969;45:1288-1305 Detry JMR, Piette F, Brasseur LA: Hemodynamic determinants of exercise ST segment depression in coronary patients. Circulation 1970;42:593-599 Bruce RA: Evolving improvements in exercise electrocardiography (editorial). Circulation 1989;79:458-459 Okin PM, Ameisen 0, Kligfield P: A modified treadmill exercise protocol for computer-assisted analysis of the ST segment/heart rate slope: Methods and reproducibility. J Electrocardiol 1986;19:311-318 Vecchio TJ: Predictive value of a single diagnostic test in unselected populations. N Engl J Med 1966;274:547-551 Parker JO, Chiong MA, West RO, Case RB: Sequential alterations in myocardial lactate metabolism, ST segments, and left ventricular function during angina induced by atrial pacing. Circulation 1969;40:113-131 33. Ihlen H, Simonsen S, Thaulow E: Myocardial lactate metabolism during pacing induced angina pectoris. Scand J Clin Lab Invest 1983;43:1-7 34. Tomoike H, Franklin D, McKown D, Kemper WS, Guberek M, Ross J Jr: Regional myocardial dysfunction and hemodynamic abnormalities during strenuous exercise in dogs with limited coronary flow. Circ Res 1978;42:487-496 35. Remme WJ, Van den Berg R, Mantel M, Cox PH, Van Hoogenhuyze DCA, Krauss XH, Storm CJ, Kruyssen DACM: Temporal relation of changes in regional coronary flow and myocardial lactate and nucleoside metabolism during pacing-induced ischemia. Am J Cardiol 1986; 58:1188-1194 541 36. Homans DC, Sublett E, Dai XZ, Bache RJ: Persistence of regional left ventricular dysfunction after exercise-induced myocardial ischemia. J Clin Invest 1986;77:66-73 37. Savage MP, Squires LS, Hopkins JT, Raichlen JS, Park CH, Chung EK: Usefulness of ST segment depression as a sign of coronary artery disease when confined to the postexercise recovery period. Am J Cardiol 1987;60:1405-1406 38. Gianelly RE, Treister BL, Harrison DC: The effect of propranolol on exercise-induced ischemic ST segment depression. Am J Cardiol 1969;161-165 39. Baily IK, Anderson SD, Rozea PJ, Bernstein L, Nyberg G, Korner PI: Effect of beta-adrenergic blockade with alprenolol on ST segment depression and circulatory dynamics during exercise in patients with effort angina. Am Heart J 1976;92:416-426 40. Castellanet MJ, Greenberg PS, Ellestad MH: Comparison of ST segment changes on exercise testing with angiographic findings in patients with prior myocardial infarction. Am J Cardiol 1978;42:29-35 41. Paine TD, Dye LE, Roitman DI, Sheffield LT, Rackley CE, Russell RO, Rogers WJ: Relation of graded exercise test findings after myocardial infarction to extent of coronary artery disease and left ventricular dysfunction. Am J Cardiol 1978;42:716-723 42. Ameisen 0, Kligfield P, Okin PM, Miller DH, Borer JS: Effects of recent and remote infarction on the predictive accuracy of ST segment/heart rate slope. JAm Coll Cardiol 1986;8:267-273 43. Sketch MH, Mooss AN, Butler ML, Nair CK, Mohiuddin SM: Digoxin-induced positive exercise tests: Their clinical and prognostic significance. Am J Cardiol 1981;48:655-659. 44. Diamond GA, Forrester JS: Analysis of probability as an aid in the clinical diagnosis of coronary artery disease. N Engl J Med 1979;300:1350-1358 45. Rifkin RD, Hood WB Jr: Bayesian analysis of electrocardio- graphic exercise stress testing. N Engl J Med 1977; 297:681-686 46. Kligfield P, Okin PM, Ameisen 0, Wallis J, Borer JS: Correlation of the exercise ST/HR slope with anatomic and radionuclide cineangiographic findings in stable angina pectoris. Am J Cardiol 1985;55:271-276 KEY WORDS * exercise tests * electrocardiography * oxygen consumption * ischemia Recovery-phase patterns of ST segment depression in the heart rate domain. Identification of coronary artery disease by the rate-recovery loop. P M Okin, O Ameisen and P Kligfield Downloaded from http://circ.ahajournals.org/ by guest on June 11, 2017 Circulation. 1989;80:533-541 doi: 10.1161/01.CIR.80.3.533 Circulation is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Copyright © 1989 American Heart Association, Inc. All rights reserved. Print ISSN: 0009-7322. Online ISSN: 1524-4539 The online version of this article, along with updated information and services, is located on the World Wide Web at: http://circ.ahajournals.org/content/80/3/533 Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in Circulation can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office. Once the online version of the published article for which permission is being requested is located, click Request Permissions in the middle column of the Web page under Services. Further information about this process is available in the Permissions and Rights Question and Answer document. Reprints: Information about reprints can be found online at: http://www.lww.com/reprints Subscriptions: Information about subscribing to Circulation is online at: http://circ.ahajournals.org//subscriptions/