Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
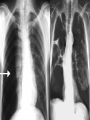
PNEUMOTHORAX TUCOM Internal Medicine 4th year Dr. Hasan.I.Sultan Pneumothorax Define as; Air accumulates in the pleural space Classification of pneumothorax A-Spontaneous 1-Primary; Without evidence of overt lung disease. Air escapes from the lung into the pleural space through rupture of a small subpleural emphysematous bulla or pleural bleb, or the pulmonary end of a pleural adhesion. 2-Secondary; Underlying lung disease, most commonly COPD and TB; also seen in asthma, lung abscess, pulmonary infarcts, bronchogenic carcinoma, all forms of fibrotic and cystic lung disease. B-Traumatic; • Iatrogenic (e.g. following thoracic surgery or biopsy) • Non-iatrogenic Clinical features; Commonest symptoms are sudden-onset unilateral pleuritic chest pain or breathlessness Small pneumothorax (<2 cm visible rim of air on chest x ray between lung margin and chest wall and occupying <50% of the volume of hemithorax) o The physical examination may be normal. A larger pneumothorax (>2 cm visible rim of air on chest x ray between lung margin and chest wall and occupying >50% of the volume of hemithorax) results in; o Decreased or absent breath sounds o Resonant percussion Types of spontaneous pneumothorax 1-Tension pneumothorax; It can act as a one-way valve allowing air to enter the pleural space during inspiration but not to escape on expiration. Intrapleural pressure may rise to well above atmospheric levels causes mediastinal displacement towards the opposite side and cardiovascular system compromise. Clinically, rapidly progressive breathlessness, marked tachycardia, hypotension, cyanosis and tracheal displacement away from the side of the lesion 2-Closed pneumothorax; Communication between the lung and pleural space seals off as the lung deflates and does not reopen the mean pleural pressure remains negative spontaneous reabsorption of air and re-expansion of the lung occur over a few days or weeks, and infection is uncommon. 3-Open pneumothorax; Communication fails to seal and air continues to transfer freely between the lung and pleural space- a bronchopleural fistula-transmission of infection – empyema. rupture of an emphysematous bulla, tuberculous cavity or lung abscess into the pleural space. Investigations Chest X-ray; Shows the sharply defined edge of the deflated lung with complete translucency (no lung markings) between this and the chest wall. Chest X-rays also show the extent of any mediastinal displacement and give information regarding the presence or absence of pleural fluid and underlying pulmonary disease. CT of chest; Is useful in distinguishing bullae from pleural air. Management Primary pneumothorax where the lung edge is less than 2 cm from the chest wall and the patient is not breathless normally resolves without intervention. Percutaneous needle aspiration (PNA) of air is a simple and well-tolerated alternative to intercostal tube drainage, with a 60-80% chance of avoiding the need for a chest drain in young patients presenting with a moderate or large spontaneous primary pneumothorax. Intercostal tube drainage; indicate in above patient who does not improved by PNA and in patients with underlying chronic lung disease, however, even a small secondary pneumothorax may cause respiratory failure. Need inpatient observation. Inserted in the 4th, 5th or 6th intercostal space in the mid-axillary line Supplemental oxygen as this accelerates the rate at which air is reabsorbed by the pleura. Surgical pleurodesis; • Second pneumothorax (even if ipsilateral). • First episode of secondary pneumothorax if low respiratory reserve makes recurrence hazardous • Occupational risk (e.g. flying or diving) should also undergo definitive treatment after the first episode of a primary spontaneous pneumothorax. • Persistent air leak and the lung fails to re-expand after appropriate pleural drainage.