Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
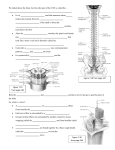
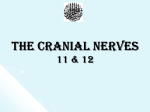
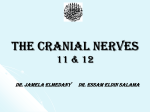
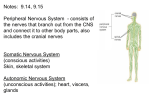
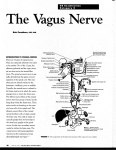
MINISTRY OF HEALTH OF UKRAINE VINNYTSIA NATIONAL MEDICAL UNIVERSITY NAMED AFTER M.I.PIROGOV NEUROLOGY DEPARTMENT Stomatology Faculty Lesson #6 Brainstem. Medulla Oblongata. Anatomy of Cranial Nerves IX-XII. 1. Goals: 1.1. To study the anatomical fundamentals of the Brainstem, the main Brainstem syndromes and their anatomical localization. 1.2. To acquire the technique of the examination of the Cranial Nerves IX-XII in normal condition and in different pathological conditions. 2. Basic questions: 2.1. Brainstem. Anatomical Fundamentals. 2.2. Cranial Nerves IX-XII. Examination of the Cranial Nerves IX-XII. 3. Literature: Mathias Baehr, M.D., Michael Frotscher, M.D. Duus’ Topical Diagnosis in Neurology. – P. 194-215 Mark Mumenthaler, M.D., Heinrich Mattle, M.D. Fundamentals of Neurology. – P. 26-27 Surface Anatomy of the Brainstem The three brainstem segments, i.e., the midbrain, pons, and medulla, have clearly defined borders on the ventral surface of the brainstem (Fig. 4.1a). Medulla The medulla extends from the site of exit of the roots of the first cervical nerve (C1), at the level of the foramen magnum, to its junction with the pons 2.53 cm more rostrally. Dorsal view. The gracile tubercles are seen on either side of the midline, flanked by the cuneate tubercles (Fig. 4.1b). These small protrusions are produced by the underlying nucleus gracilis and nucleus cuneatus of both sides. These are the relay nuclei in which the posterior column fibers of the spinal cord form synapses onto the second neurons of the afferent pathway, which, in turn, project by way of the medial lemniscus to the thalamus. The rostral border of the medulla is defined by a line drawn through the caudal portion of the middle cerebellar peduncles. The floor of the fourth ventricle, or rhomboid fossa, is bounded laterally by the inferior and superior cerebellar peduncles and divided into rostral and caudal portions by the striae medullares, which contain fibers running from the arcuate nuclei to the cerebellum. The caudal part of the floor contains a number of protrusions (tubercles) produced by the underlying cranial nerve nuclei, including the vagal triangle (or “trigone”; dorsal nucleus of the vagus nerve), the hypoglossal triangle (nucleus of the hypoglossal nerve), and the vestibular area (vestibular and cochlear nuclei), while the rostral part contains the facial tubercle, which is produced by the fibers of the facial nerve as they course around the abducens nucleus. The roof of the fourth ventricle is made up of the superior medullary velum, the cerebellar peduncles, and the cerebellum itself. Ventral and lateral views. A ventral view of the medulla (Fig. 4.1a) reveals the pyramids, which lend their names to the pyramidal tracts, whose fibers course through them. The pyramidal decussation can also be seen here. Lateral to the pyramid on either side is another protrusion called the olive, which contains the inferior olivary nucleus. The hypoglossal nerve (XII) emerges from the brainstem in the ventrolateral sulcus between the pyramid and the olive. The nuclei of the hypoglossal nerve, like those of the nerves to the extraocular muscles, are located near the midline in the brainstem, in the so-called basal lamina. Dorsal to the olive, the roots of the accessory (XI), vagus (X), and glossopharyngeal (IX) nerves emerge from the brainstem in a vertically oriented row (Fig. 4.1a and c). Further dorsally, between the exit of these nerves and the dorsolateral sulcus, lies the tuberculum cinereum, formed by the nucleus of the spinal tract of the trigeminal nerve. This is also the site of the posterior spinocerebellar tract, which ascends to the cerebellum by way of the inferior cerebellar peduncle (restiform body). Cranial Nerves The cranial nerves are examined individually. Figure 3.3 provide an overview of the anatomy and function of the 12 cranial nerves. The first two cranial nerves (the olfactory and optic nn.) are, in reality, portions of the brain that have been displaced into the periphery. The remaining 10 cranial nerves structurally and functionally resemble the other peripheral nerves of the body. They have motor, somatosensory special sensory, and autonomic functions. CN IX and X: Glossopharyngeal and Vagus Nn. The efferent fibers from the nucleus ambiguus to the muscles of the palate, larynx, and pharynx reach these structures through the glossopharyngeal and vagus nn. The larynx is innervated by two vagal branches, the superior laryngeal n, and the recurrent laryngeal n. The glossopharyngeal n. carries somatosensory fibers from the soft palate, the posterior pharyngeal wall, the tonsillar fossa, and the middle ear, as well as gustatory fibers from the posterior third of the tongue. The vagus n. carries somatosensory fibers from the external auditory canal, part of the external ear, and the meninges of the posterior fossa. It also carries efferent parasympathetic fibers to the thoracic and abdominal viscera. Examination of the pharynx and larynx. The motor function of the ninth and tenth cranial nerves is assessed by inspection of the palate and throat and, more importantly, by observation of the movements of these structures during phonation (“a−aa−ah . . .”) and after induction of the gag reflex by touching the posterior pharyngeal wall with, e. g., a cotton swab. Unilateral weakness of the palatal veil and the pharyngeal muscles makes these structures deviate laterally away from the side of the lesion, as shown in Fig. 3.13. Hoarseness due to a unilateral recurrent laryngeal nerve palsy can sometimes be heard only when the patient sings. CN XI: Accessory N. Examination of the sternocleidomastoid and trapezius mm. The external (final) branch of the purely motor accessory n. supplies the sternocleidomastoid m. and the upper portion of the trapezius m. To test the sternocleidomastoid m. on one side, the examiner asks the patient to turn the head to the opposite side against resistance, then observes and palpates the muscular contraction at the anterior edge of the lateral triangle of the neck (Fig. 3.14). The upper portion of the trapezius m. is examined as follows: the examiner stands in front of the patient, puts both hands on the patient’s shoulders, grasps the upper edge of the trapezius m. on either side between the thumb and index finger, and asks the patient to shrug the shoulders against resistance. In unilateral accessory nerve palsy, the shrug is less powerful on the affected side and the trapezius m. is palpably thinner andweaker (Fig. 3.15). CN XII: Hypoglossal N. The twelfth cranial nerve is a purely motor nerve to the muscles of the tongue. Lesions of this nerve produce atrophy and weakness of the tongue. A unilateral lesion usually produces a longitudinal furrow; when protruded, the tongue deviates to the weaker side because of the predominant force of the intact contralateral genioglossus m., which “pushes” the tongue across the midline (Fig. 3.16). Phonation, Articulation, and Speech Assessment of the patient’s voice and speech is a compulsory part of the neurological examination. The examiner should pay attention to possible hoarseness, to the volume of speech (e. g., hypophonia in Parkinson disease, p. 128), and to possible disturbances of articulation (dysarthria), of the tempo of speech, and of its linguistic form and content (aphasia, p. 41).