Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
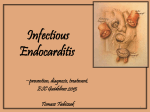
Cardiovascular disease Atherosclerosis • Slowly progressive disease of arteries, marked by elevated fibrofatty intimal plaques, formed by lipid deposition, smooth muscle cell proliferation and synthesis of extracellular matrix in intima. • Large to medium size muscular and large elastic arteries are involved, principally in abdominal aorta, coronary arteries, popliteal arteries, and descending thoracic aorta. • Lesion initially tend to be focal, only partially involving vessel circumference, and are patchy along the length. • Disease typically manifest in middle age or later life either as the vessel lumen is compromised, predisposing to thrombosis, or as underlying media thinned, predisposing to aneurysm formation. Risk factors for atherosclerosis A. Major: 1. Nonmodifiable: increasing age and family history. 2. Potentially controllable: hyperlipidemia, hypertension, smoking, diabetes. B. Uncertain significance: obesity, physical inactivity, stress, alcohol, estrogen deficiency in post menopausal. Morphology • Raised white intimal lesion, protruding into vessel lumen. • Histologically, atheroma composed of a superficial fibrous cup, containing smooth muscle cells, leukocytes and dense connective tissue extracellular matrix, overlying a necrotic core containing dead cells, lipid, cholesterol clefts, lipid laden foam cells and plasma protein, in the periphery are proliferating small vessels. Vasculitis • Vascular inflammatory injury, often with necrosis. • May be localized as a result of direct injury (infection, trauma, toxins), or systemic, characterized by multifocal necrosis (necrotizing vasculitis) and thrombosis. • Most systemic vasculitis are thought to have immune origin, secondary to deposition of Ag-Ab complex (e.g: systemic lupus erythematous), or antibody to fixed tissue Ag (e.g: Kawasaki disease) or delay type hypersensitivity reactions, especially in lesions with granulomas (e.g: temporal arteritis) Vascular tumors • Benign tumors: as Hemangioma, Glomus tumor, simple and cavernous Lymphangioma. • Intermediate: as Kaposi sarcoma, Hemangioendothelioma. • Malignant: as Angiosarcoma, Hemangiopericytoma Hemangioma • Common on children, has several histological and clinical variants. 1. Capillary hemangioma: usually in skin and mucous membrane, 1-2 mm to several centimeter in diameter, well defined Unencapsulated lesion composed of closely packed aggregates of capillary size thin-wall vessels. 2. Cavernous hemangioma: large vascular channels forming un encapsulated but discrete lesions, usually 1-2 cm in diameter, they have same distribution as capillary hemangioma but common particular in liver but can involve CNS and viscera. 3. Pyogenic granuloma: ulcerated polypoid variant of capillary hemangioma on skin or oral mucosa, often secondary to trauma, consist of proliferating capillaries with significant interspersed edema and inflammatory infiltrate. Capillary hemangioma Cavernous hemangioma Kaposi sarcoma • Four form are recognized. 1. Chronic classic: elderly men of eastern European, consist of multiple red to purple cutaneous plaques and nodules on lower extremities. 2. Lymphadenopathic/ African: clinically similar to classic but in younger men, largely restricted to lymph nodes. 3. Transplant associated: patient undergoing immunosuppressive therapy, there is both cutaneous and systemic visceral involvement. 4. AIDS-associated: occur anywhere in skin and mucous membrane, lymph nodes, GIT or viscera. Morphology • Lesion consist of sheets of plump, spindle shape cells creating slit like vascular space filled with red blood cells, intermingled with vascular channels lined by recognizable endothelium. • There is also scattered microhemorrhage and hemosedrin deposits. • Origin of tumor cells remain uncertain, but current evidence favors viral associated neoplasm (HIV or HPV 8) of endothelial cells. Kaposi sarcoma Angiosarcoma • Neoplasm arise in skin, soft tissue, breast, liver and spleen. • Begin as small, well demarcated red nodule, evolving into large, fleshy gray-white, soft tissue masses. • Degree of differentiation vary from highly vascular variety with plump anaplastic endothelial cells to quite undifferentiated lesion without vascular lumen and with marked cellular atypia, including giant cells. Myocardial infarction • Two types 1. Transmural infarct: full thickness of ventricular wall, usually caused by sever coronary arteries atherosclerosis. 2. Subendocardial infarct: limited to inner one third or half of ventricular wall Morphology Grossly : • Before 6-12 hrs, lesion usually unapparent; however, in early as 3-6 hrs lesion may accentuated by use of histochemical techniques. • By 12-24 hrs, infarct tissue readily apparent-pale to cyanotic. • In 1st week, lesion become progressively more sharply defined, yellow and softened. • circumferential rim of hyperemic granulation tissue appears by 7-10 days and progressively expands. • White fibrous scar usually well established by 6 weeks. Microscopically • Within 1 hr of ischemic injury, there is intracellular edema, myocytes at edge of infarct become wavy and buckled, attributed to stretching of noncontractile dead fibers by adjacent viable contracting myocytes. • 12-72 hrs; neutrophils infiltration into necrotic tissue, with progressive evolution of characteristic myocytes coagulation necrosis, dead myocytes become hypereosinophilic with loss of nuclei. • 3-7 days; dead myocytes begin to disintegrate and are resorbed by macrophages and enzyme proteolysis. • After 7-10 days; granulation tissue replace necrotic tissue, ultimately generating dense fibrous tissue. Rheumatic heart disease. • Acute recurrent inflammatory disease that typically occur 1-5 weeks after a group A of streptococcal infection. • Occur mainly in children but adults may suffer the first attack. • Diagnosis rests on clinical history and the presence of two of five major (Jones) criteria, as follow: 1. Erythema marginatum: macular skin lesion. 2. Sydenham chorea; neurological disorder( purposeless movement). 3. Carditis. 4. Subcutaneous nodules. 5. Migratory large joint polyarteritis. Minor criteria: fever, arthralgia, leukocytosis Morphology • Aschoff bodies are pathognomic foci of fibrinoid necrosis found in many sites. • Transient fibrinous pericarditis in acute phase. • Inflammatory valvulitis. • Chronic or healed valve shows fibrous thickening of leaflets, bridging fibrosis across the commissures, in addition to calcification. Infective Endocarditis • Colonization of cardiac valves with microbial organism lead to the formation of friable , infected vegetation's and frequently valve injury, termed infective myocarditis, traditionally, acute and subacute forms has been distinguished. Acute infective endocarditis • Caused by high virulence organisms (e.g; staph. aureus) often seeding a previously normal valve producing a necrotizing ulcerative and invasive infection. • It is rapidly developing fever with rigors, malaise and weakness. • The large vegetation in acute infective endocarditis often cause embolic complications. • Even with treatment death occur in days to weeks in 50-60 % of patients. Subacute infective endocarditis • Caused by organism of low to moderate virulence (most commonly streptococcus viridans) seeding abnormal or previously injured valve. • Cause less valvular destruction than acute form. • Has insidious onset with non-specific malaise, low grade fever, weight loss and flue like syndrome. • Vegetations tend to be smaller than acute form, and so embolic complication are less frequent than acute endocarditis. • Less fatal than acute. Morphology • Friable 0.5-2 cm microbe laden vegetation are apparent on one or more valve. • Acute infective endocarditis commonly associated with bulky vegetations that cause erosion or perforation of leaflets, invading adjacent myocardium or aortic wall to produce abscess cavity. • Subacute has smaller vegetations and rarely erode or penetrate the leaflets. • With prosthetic valve ring abscess is almost always present. • With intravenous drug abuse , vegetations are often acute and on right sided valve, but left sided valve are also frequently involved , most often staph. aureus