Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
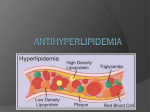
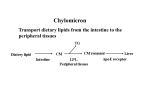
Antihyperlipoproteinemic Drugs Antihyperlipoproteinemic Drugs Niacin (Nicotinic Acid) Fibrates: Gemfibrozil & Clofibrate Mechanism of Action Indications AE - Water soluble vitamin that inhibits lipolysis in adipose tissue and so lowers free FA in circulations, which is necessary for VLDL and so LDL synthesis. So, both TAG (in VLDL) and cholesterol (in VLDL and LDL goes down. - Increases tissue plasminogens and lowers plasma fibrinoges - Tx. of type IIb and type IV hyperlipidemia - Raise plasma HDL levels (most effective) - Decrease plasma TAG by increasing lipoprotein lipase activity and so hydrolyzing TAG in VLDL and Chylomicrons - Moderate increase in HDL - Inhibits cholesterol synthesis in liver and increases biliary excretion of cholesterol so decreased plasma cholesterol - Lowers plasma fibrinogen levels - Tx. Of type III, type IV and type V hyperlipidemia - Decreased MI incidence had been seen w/ this drug - Intense cutaneous flush which can be decreased by taking aspirin prior to taking niacine - Pruritus - Nausea - Abdominal pain - Hyperuricemia & gout - Hepatotoxicity - Impaired glucose tolerance - Activation of peptic ulcer - Mild GI disturbance - Gall stone formation b/c of increased biliary cholesterol excretion - Myositis, muscle weakness and tenderness, myalgia - Claudications - Thrombosis (??) - Decreased libido CI Other Should be avoided in pregnancy b/c of teratogenic effects Shows decreased mortality Should not be used in pt. w/ hepatic and kidney dysfunction and should be avoided in pt. w/ pre-existing gall bladder disease Lowers coumarin clearance and so increases its anticoagulant effects, so should lower the coumarin dose when taking this drug Bile acid binding resins: Cholestyramine Colestipol - Binds to (-)vely charged bile acids and bile salts and increases their excretion in feces and so decreases bile acid return to liver, so liver uses cholesterol to make more bile acid and bile salt so the intracellular cholesterol goes down and so LDL receptors go up, which increases uptake of circulating LDL and so plasma cholesterol goes down. HMG CoA Reductase Inhibitors: Lovastatin Simvastatin Pravastatin Fluvastatin - Inhibits HMG CoA Reductase, which is necessary for cholesterol synthesis. So, intracellular cholesterol goes down. As a result, LDL receptors goes up and uptake of circulating LDL by cell goes up lowering plasma cholesterol - HDL may go up in some pt. - Small decrease in TAG - Macrophages ingest oxidized LDL and become foam cells, which then accumulates in vessels and forms atherosclerotic plaque, so probucol inhibits oxidation of LDL and so slows development of atherosclerosis Probucol - DOC in tx. of type IIa and type IIb hyperlipidemia. (it has little effects in pt. who are homozygous of type IIa hyperlipidemia that is they have no functional LDL receptors) - Cholestyramine relieves pruritus caused by bile acid accumulation in pt. w/ biliary obstruction - Tx. of all kinds of hyperlipidemias - Less effects in pt. homozygous type IIa hyperlipidemia - Constipation, bloating Flatulence Nausea Abdominal pain Impaired absorption of fat soluble vitamins (vit. A, D, E and K) - Reduced absorption of folic acid and ascorbic acid - Interfere w/ intestinal absorption of other drugs - limited use in type IIa and type IIb hyperlipidiemia b/c it also decreases HDL which is a risk factor for atherosclerosis - claimed to reduce fq of new angioplasty - Mild GI Disturbance - Prolongation of QT interval - Fewer AEs Increased liver enzymes Myopathy Rhabdomyolysis GI disturbance Headache Increases coumarin levels Should be taken w/ meals CI in pregnancy and nursing mothers, and shouldn’t be used in children and teenagers CI in pt who have abnormally long QT interval -Accumulates in adipose tissue for months - Should be taken w/ food Combination Drug Therapy: - Type II hyperlipidemias can be treated with combination of Niacin and Bile acid binding agent such as cholestyramine. The combination of HMG CoA Reductase inhibitors and bile acid binding agents can be used to lower LDL cholesterol. Triple drug combination is possible but increases risk of kidney failure Types of Hyperlipidemias Type of Hyperlipidemia Type I: Familial Hyperchylomicronemia Type IIA: Familial Hypercholesterolemia Problem Increased chylomicrons and so increased TAG Blocked degradation of LDL so, elevated LDL w/ normal VLDL (increased plasma cholesterol) Type IIB: Familial Combined (Mixed) Hyperlipidemia Increased VLDL and LDL, so increased plasma TAG and cholesterol Type III: Familial Dysbetalipoproteinemia Increased IDL so increased TAG and cholesterol Type IV: Familial Hypertriglyceridemia Increased VLDL and so increased TAG Type V: Familial Mixed Hypertriglyceridemia Increased VLDL and Chylomicrons, so elevated cholesterol but greatly increased TAG Treatment No drug therapy Low fat diet Bile acid binding resins HMG CoA Reductase inhibitors Niacin (in homozygous) Low saturated fat and low cholesterol diet Niacin Bile acid binding resins HMG CoA Reductase inhibitors Low saturated fat and low cholesterol diet Fibric Acid HMG CoA Reductase inhibitors Diet modification Fibric Acid Niacin Diet modification Fibric Acid Niacin HMG CoA Reductase inhibitors Diet modification