Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
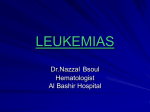
Published OnlineFirst August 25, 2009; DOI: 10.1158/1078-0432.CCR-08-2941 Molecular Pathways Complexity of CEBPA Dysregulation in Human Acute Myeloid Leukemia Thomas Pabst1,3 and Beatrice U. Mueller2,3 Abstract The transcription factor CCAAT enhancer binding protein alpha (CEBPA) is crucial for normal development of granulocytes. Various mechanisms have been identified how CEBPA function is dysregulated in patients with acute myeloid leukemia (AML). In particular, dominant-negative mutations located either at the N- or the C terminus of the CEBPA gene are observed in roughly 10% of AML patients, either in the combination on separate alleles or as sole mutation. Clinically significant complexity exists among AML with CEBPA mutations, and patients with double CEBPA mutations seem to have a more favorable course of the disease than patients with a single mutation. In addition, myeloid precursor cells of healthy carriers with a single germ-line CEBPA mutation evolve to overt AML by acquiring a second sporadic CEBPA mutation. This review summarizes recent reports on dysregulation of CEBPA function at various levels in human AML and therapeutic concepts targeting correction of CEBPA activity. The currently available data are persuasive evidence that impaired CEBPA function contributes directly to the development of AML, whereas restoring CEBPA function represents a promising target for novel therapeutic strategies in AML. (Clin Cancer Res 2009;15 (17):5303–7) Background The hallmark of acute myeloid leukemia (AML) is the accumulation of myeloid precursor cells in the bone marrow. Characteristically, the malignant cells display a block in their normal differentiation process at a particular stage. Remarkably, however, research on the pathogenesis of AML has traditionally focused on the analysis of oncogenes or tumor suppressor genes to clarify the deregulated proliferation and cell death features of AML cells. Although the ultimate relationship between altered proliferation and differentiation in AML remains to be elucidated, a current concept indicates that deregulation of some transcription factors critically affects both differentiation and cell cycle as being involved in AML. This review intends to highlight recent reports on dysregulation of the differentiation factor CEBPA at various levels in human AML. The CCAAT enhancer binding protein alpha (CEBPA) is a member of the basic region leucine zipper family of transcription factors (1–3). It is composed of two transactivation domains in the N-terminal part, and a leucine zipper region mediating dimerization with other CEBP family members and a DNA- Authors' Affiliations: Departments of 1Oncology and 2Internal Medicine, University Hospital, and 3University of Bern, Bern, Switzerland Received 4/28/09; revised 5/6/09; accepted 5/7/09; published OnlineFirst 8/25/09. Grant support: Swiss National Science Foundation (SF) SF 310000-109388 and Swiss Cancer League (T. Pabst); and SF31000-113761 (B.U. Muellar). Requests for reprints: Thomas Pabst, University Hospital, 3010 Bern, Switzerland. Phone: 41-31-632-8430; Fax: 41-31-632-3410; E-mail: thomas. [email protected]. F 2009 American Association for Cancer Research. doi:10.1158/1078-0432.CCR-08-2941 www.aacrjournals.org binding domain in the C-terminal part. As a condition for DNA binding, dimerization depends on the basic amino acid residues, and genomic alterations in the exact distance between basic region and leucine zipper impair DNA binding. Two inframe start codons give rise to two CEBPA isoforms: The p30 protein is initiated at an AUG codon further downstream and thus lacks the amino terminal sequences, whereas the C terminus is identical to the full-length p42 protein (4–6). As a consequence, the p30 isoform lacks domains mediating the contact with the transcriptional apparatus, whereas other functions such as dimerization or regions involved in protein-protein interactions are preserved in both p30 and p42 proteins. CEBPA is an intronless gene located at chromosome 19q13.1 (2, 3). It was originally isolated as a rat liver transcription factor regulating hepatic and adipocyte genes (7–9). Studies in adipocyte lines have founded the role of CEBPA as an inhibitor of cell proliferation and as a tumor suppressor. In hematopoiesis, the interest in CEBPA is based on its crucial role during the development of granulocytes and on its deregulation associated with myeloid transformation (10–14). Nonconditional targeted disruption of cebpa results in a selective block in early granulocyte maturation, and these mice die at birth because of severe hypoglycemia (15). Conditional cebpa deficiency in adult mice blocks the transition from common myeloid progenitors (CMP) to granulocyte monocyte progenitors (GMP) resulting in the accumulation of myeloid blasts (16). Moreover, knock-in mice with a targeted mutation in the cebpa basic region, which specifically inhibits the CEBPAE2F interaction, predisposed mice to a myeloproliferative disorder (17). Finally, mice carrying engineered cebpa alleles that specifically disrupt the 42-kDa wild-type protein while allowing expression of the dominant-negative 30-kDa form developed 5303 Clin Cancer Res 2009;15(17) September 1, 2009 Downloaded from clincancerres.aacrjournals.org on July 26, 2015. © 2009 American Association for Cancer Research. Published OnlineFirst August 25, 2009; DOI: 10.1158/1078-0432.CCR-08-2941 Molecular Pathways AML with complete penetrance (18). These studies suggest that the tumor suppressor activity of CEBPA resides within the 42-kDa translational isoform, and that efficient transformation of the granulocyte lineage observed in the absence of p42 is due to p30-mediated bypassing of the CEBPA-dependent transition from the CMP stage to the GMP stage. In AML, specific loss of p42, therefore, bypasses the CEBPA-regulated coupling of lineage commitment and proliferation control during myeloid differentiation, leading to the formation of progenitors prone to undergo transformation and exerting deregulated proliferative capacity. Clinical-Translational Advances CEBPA mutations and expression levels. With regard to its key role for myeloid development, it was hypothesized that CEBPA function may be decreased or absent in leukemic cells of AML patients. In fact, a rapidly increasing literature suggests that CEBPA function is critically altered in subsets of AML patients at various levels. First of all, a number of groups have reported genomic mutations in the CEBPA gene in between 5% and 14% of AML patients (6, 19–23). Two types of mutations are predominantly observed (Fig. 1): N-terminal frame-shift mutations prematurely truncate the full-length p42 form while preserving the p30 form, with the latter inhibiting the remaining wild-type CEBPA p42 protein in a dominant-negative manner (6). Second, C-terminal in-frame insertions or deletions disrupt the basic zipper region, thus critically affecting DNA binding (6); this is further illustrated by reports on the X-ray structure of the CEBPA protein-DNA interaction identifying the critical basic region residues (24). The characteristics of patients with CEBPA mutations involve myeloblastic subtypes (M1 or M2 according to the FrenchAmerican-British classification), and a normal karyotype. CEBPA mutations are not consistently associated with specific cytogenetic abnormalities or molecularly defined entities (20, 23). The immunophenotype of AML blasts with CEBPA mutations comprises expression of HLA-DR + CD7 + CD13 + CD15 + CD33 + CD34+, with expression of CD7 being particularly noteworthy because this T-cell marker is usually negative in AML blasts (22). Using microarray analyses, AML patients with nonsilent CEBPA mutations express a distinctive gene expression signature (25–28). Surprisingly, genes involved in erythroid differentiation, including GATA1, FOG1, EPOR, KLF1, GFI1B, and genes encoding erythrocyte membrane proteins and hemoglobin chains, were upregulated in AML patients with CEBPA mutations (28). In contrast, genes involved in myeloid differentiation, such as RUNX1, PU.1, and ID1, were suppressed in such patients, as were members of the homeobox family (HOXA1-10, HOXB2-6, and MEIS1). Remarkably, genes involved in proliferation signaling pathways, such as FLT3, LYN, and members of the RAS family or their regulators (VAV2, VAV3), were also downregulated in these patients (28). The miRNA signature associated with CEBPA mutations comprised 15 miRNA probes that were upregulated, Fig. 1. CEBPA functional domains and mechanisms resulting in CEBPA dysregulation in human AML. Two transactivation domains (TAD1, TAD2) are depicted as well as a basic region (basic) mediating DNA binding and a leucine zipper region (Zip) for dimerization. The mRNA translated from the ATG at amino acid (AA) 1 encodes the wild-type 42-kDa CEBPA protein, whereas the 30-kDa form is translated from the ATG at AA120. The peptide initiated at AA1 is truncated by N-terminal frame-shift mutations, whereas the C-terminal in-frame mutations affect full-length and 30-kDa peptides. S-21-P: phosphorylation at serin 21 mediates functional inactivation of the CEBPA protein. K-161-sumoylation: Sumoylation at lysine 161 by activated Ubc9 as well as activation of TRIB2 ultimately lead to proteasomal degradation of the CEBPA protein. Activated calreticulin blocks CEBPA translation. Physical interaction of CEBPA protein with c-Jun or AML1-ETO suppress CEBPA function. Clin Cancer Res 2009;15(17) September 1, 2009 5304 www.aacrjournals.org Downloaded from clincancerres.aacrjournals.org on July 26, 2015. © 2009 American Association for Cancer Research. Published OnlineFirst August 25, 2009; DOI: 10.1158/1078-0432.CCR-08-2941 CEBPA in Human AML among them eight miRNA probes corresponding to members of the miR-181 family, which is involved in erythroid and lymphoid differentiation. In contrast, no hematopoietic function is known so far for the two miRNAs (miR-194 and miR-34a), which were suppressed in patients with CEBPA mutations. There is a predominant CEBPA mutation pattern in AML patients, with the majority of AML patients having more than one CEBPA mutation (20, 23). The most frequent scenario is the combination of an N-terminal frame-shift mutation and a C-terminal in-frame mutation, with the two mutations typically being located on different alleles. This may have implications for our understanding why additional genetic abnormalities are rarely observed in AML patients with CEBPA mutations, because the most frequent “second” genomic abnormality in such patients is an additional CEBPA mutation. Because both main types of mutation can occur as sole abnormality at diagnosis, these observations indicate that CEBPA mutations might predispose to the occurrence of an additional CEBPA mutation, ultimately inducing AML. All studies so far indicated that AML patients with CEBPA mutations enjoy a favorable clinical outcome (20–23). Why CEBPA mutations confer good prognosis remains unclear. Interestingly, it was recently suggested that only patients with double CEBPA mutations have favorable clinical outcome, whereas single CEBPA mutations did not differ from CEBPA wild-type patients (29). However, the groups were small (28 CEBPAdouble-mut versus 13 CEBPAsingle-mut patients); forthcoming data from other cohorts are necessary to appreciate the significance of this finding. The putative discrepancy in outcome between CEBPAdouble-mut and CEBPAsingle-mut patients may be explained by the concept that the decrease in CEBPA function mediated by mutation in a single allele may not be sufficient to initiate AML, thus requiring additional mutational events. Whereas it was suggested that CEBPA single-mut patients have some tendency toward more FLT3-ITD and NPM1 mutations, this clearly needs to be investigated in larger cohorts (29). Because the ratio of p30/p42 CEBPA peptides is different in leukemic cells with single versus double CEBPA mutations, it is less surprising that distinctive gene expression profiles have been reported for CEBPAdouble-mut and CEBPAsingle-mut AML patients (29). Inherited AML is a rare event. Several families have been reported in whom members affected by AML carried germline heterozygous CEBPA mutations (30–34). The type of the germline CEBPA mutation was an N-terminal out-of-frame mutation leading to the preferential production of the 30-kDa dominantnegative isoform. These observations suggest that a substantial decrease in CEBPA function renders a predisposition to AML in these patients. Intriguingly, most of the affected members in the families had an additional C-terminal in-frame CEBPA mutation on separate alleles at diagnosis of AML. The C-terminal mutation disappeared upon remission (32, 33). This suggests that the germline N-terminal CEBPA mutation predisposed to the occurrence of a somatic C-terminal CEBPA mutation, ultimately inducing AML after a long latency period. However, not all carriers of a germline N-terminal CEBPA mutation developed a second CEBPA mutation at diagnosis. Despite extensive molecular analysis, no additional mutations were detected so far in most of these normal karyotype AML patients with a single germline CEBPA mutation. This finding would argue in favor of a straightforward mechanism underlying the accumulation of immature myeloid precursors in the www.aacrjournals.org presence of a disabling N-terminal mutation of the CEBPA gene in those patients. Thus, the ultimate relationship between germline CEBPA mutation and the development of overt leukemia remains to be clarified. Besides genomic mutations, dysregulated expression can disrupt the function of transcription factors crucial for normal hematopoiesis. Indeed, the presence of the AML1-ETO fusion protein, encoded by the t(8;21) translocation commonly found in AML patients of the M1 or M2 subtype, suppresses CEBPA mRNA expression through inhibition of autoregulation (35). Interestingly, other leukemic fusion proteins involving core binding factor (CBF) family members, such as the AML1MDS1-EVI1 fusion in t(3;21) AML or the CBFB-MYH11 fusion in inv(16) AML, have not been shown to suppress CEBPA mRNA indicating an AML1-ETO specific effect on CEBPA transcriptional control (35–37). In patients with severe congenital neutropenia (SCN), the lymphoid enhancer-binding factor (LEF-1) is suppressed in myeloid cells exhibiting a differentiation block of myelopoiesis at the promyelocytic stage (38). LEF-1 is a member of the Wnt signaling pathway, performing its function in complexes with βcatenin. One of the unique features of LEF-1 is to regulate target gene expression by DNA bending and helical phasing of transcription-binding sites, acting as an architectural transcription factor. Accordingly, LEF-1 was found to activate the CEBPA promoter, and reconstitution of LEF-1 in early hematopoietic progenitors of SCN patients restored CEBPA expression and corrected the defective myelopoiesis, identifying LEF-1 as a key regulator of myelopoiesis (38). Whether this mechanism is involved in subsets of AML has not been reported yet. Finally, hypermethylation of the CEBPA promoter was first reported preferentially in AML-M2 patients (39). Recently, a small subgroup of patients was defined exhibiting a gene expression profile resembling that of AML patients with CEBPA mutations, while lacking such mutations (28, 40, 41). The CEBPA gene was found to be silenced by promoter hypermethylation, and these leukemias exhibited a mixed myeloid/ T-lymphoid immunophenotype and frequent NOTCH1 mutations. The Tribbles homolog (TRIB2), a downstream effector of the NOTCH1 pathway, was induced in some of these leukemias. Remarkably, forced expression of TRIB2 altered the p30/p42 CEBPA ratio in favor of the oncogenic 30-kDa form. Moreover, activated TRIB2 blocked the CEBPA 42-kDa wildtype protein by physical interaction, resulting in the proteasomal-dependent degradation of CEBPA. Besides, a systematic analysis of leukemic cells of AML patients investigating changes of the CEBPA isoform ratio has not been reported so far, most likely because of the usual limitation of clinical material needed for such an analysis. Members of the CEBP transcription factor family can be targeted by IGH-translocations in B-cell precursor acute lymphoblastic leukemia (B-ALL) (refs. 42, 43). Importantly, such translocations resulted in overexpression of affected CEBPs, including translocation t(14;19)(q32;q13) involving CEBPA. This result indicates that not only loss, but also gain of function of CEBPA has leukemogenic potential. Regulating the rate of translation of specific mRNAs is an efficient mechanism of oncogenic proteins to modulate the levels of target proteins. Such a mechanism was shown for CEBPA in AML with t(3;21) and inv(16): The RNA-binding protein calreticulin was found to be activated in cells of such AML patients, 5305 Clin Cancer Res 2009;15(17) September 1, 2009 Downloaded from clincancerres.aacrjournals.org on July 26, 2015. © 2009 American Association for Cancer Research. Published OnlineFirst August 25, 2009; DOI: 10.1158/1078-0432.CCR-08-2941 Molecular Pathways and calreticulin protein interacts with GCN repeats within CEBPA (and CEBPB) mRNAs, thereby efficiently blocking translation of CEBP proteins (36, 37, 44). The activity of the CEBPA protein in human AML is further affected by a rapidly growing list of various mechanisms. Phosphorylation of CEBPA at serine 21 is mediated by extracellular signal-regulated kinases 1 and/or 2 (ERK1/2), which recognize serine 21 of CEBPA as a substrate through an FXFP-docking motif (45). This phosphorylation induces a conformational change in CEBPA, such that the transactivation domains of two CEBPA molecules within a dimer move farther apart. Activation of the fms-like tyrosine kinase 3 (FLT3) in human AML seems to block the phosphorylation of CEBPA at serine 21, which may explain the differentiation block of blasts in leukemias with activated FLT3 (46). Finally, sumoylation of wild-type CEBPA protein by Ubc9 activation has been shown to impair CEBPA function (47). Additional post-translational mechanisms of CEBPA modulation remain to be investigated in human AML, such as whether the composition of heterodimers with other CEBP family members is altered in AML (48). Also, the impact of repressors of CEBPA activity, such as CA150, has to be tested in AML as well as the role of CEBPA acetylation or changes in subcellular localization during malignant transformation (49–51). Finally, there is evidence that suppressed CEBP activity is involved in the differentiation block of patients with acute promyelocytic leukemia (APL/AML-M3) characterized by the presence of the PML-RARA fusion protein. Conditional induction of PML-RARA in myeloid U937 cells decreases CEBPA activity (52). In vivo, enhanced expression of CEBPA in PMLRARA transgenic mice prolongs survival of such animals (53). All-trans retinoic acid (ATRA) treatment of patients with APL induces CEBPB, CEBPE, and, to a lesser extent, CEBPA mRNA expression (54). ATRA-induced activation of CEBPB then leads to induction of PU.1, and thereby downstream effectors (54). Dysregulated transcription factor activity and leukemia therapy. At the molecular level, AML is increasingly recognized as a very heterogeneous cancer. The observation of recurring mutations in genes encoding differentiation-inducing transcription factors in AML patients has allowed the identification of new subgroups in AML, thereby contributing to a more risk-adapted therapeutic approach. Historically, the potential for differentiating therapy to improve cure rates in AML is exemplified by the use of ATRA for the treatment of APL (55). ATRA treatment is leading to a degradation of the PML-RARA fusion product, to the release of corepressors, restoration of normal regulation of RARA-responsive gens, and hence terminal differentiation of APL cells. The degradation of PML-RARA also indicates a common pathway, in which the mechanisms of action of ATRA converge on those with arsenic trioxide (ATO). At low concentrations, ATO induced partial morphologic differentiation, whereas at high concentrations, apoptosis induction prevailed in APL cells (56). In addition, much interest was historically focusing on vitamin D compounds. Although 1,25(OH)2D3 induced partial differentiation of hematopoietic blasts in some AML patients, clinical responses were modest, with hypercalcemia being a prominent limiting factor. In the past 30 years, the interrogational power of molecular methods to study AML has greatly expanded. For clinicians, this increasingly contrasts to current concepts of conventional chemotherapy still being applied as standard treatment for the vast majority of AML patients. The difficulties of developing drugs that precisely modulate specific transcription factors and of bringing them to the targeted cells remain the challenges for the development of novel therapeutic concepts targeting correction of transcription factor activities. The capacity of CEBPA to overcome the block of differentiation in AML blasts makes it an obvious target of interest for any differentiation-inducing therapy. Fusion peptides (such as TAT or VP22) facilitating the entry into the cells, as well as lentiviral vectors, may be valuable tools for such an approach (57, 58). Unfortunately, exogenous restoration of a nuclear transcription factor remains a significant technical challenge. A more promising approach seems to be the activation of the CEBPA-differentiation pathway through small molecules modulating the expression of CEBPA mRNA or protein. In fact, MAP/ERK kinase (MEK) inhibitors block serine-21 phosphorylation of CEBPA, which increases the granulocytic differentiation potential of the CEBPA protein (46). Interestingly, FLT3 tyrosine kinase inhibitors also dephosphorylate serine-21 CEBPA (46). In addition, CEBPA translation can be efficiently induced by 2-cyano-3,12-dioxoolean-1,9-dien-28-oic acid (CDDO), which alters the p42/p30 ratio of the CEBPA isoforms in favor of the full-length form thereby inducing granulocytic differentiation (59). Finally, the results of high-throughput studies are long awaited, thereby screening large collections of small molecules in order to identify compounds with the potential to restore CEBPA function. However, differentiation therapy targeting restoration of CEBPA function requires further study before clinical application. Disclosure of Potential Conflicts of Interest No potential conflicts of interest were disclosed. Acknowledgments The authors apologize to all investigators whose work could not be cited due to limitations in space and references. References 1. Landschulz WH, Johnson PF, Adashi EY, et al. Isolation of a recombinant copy of the gene encoding C/EBP. Genes Dev 1988; 2:786–800. 2. Birkenmeier EH, Gwynn B, Howard S, et al. Tissue-specific expression, developmental regulation, and genetic mapping of the gene encoding CCAAT/enhancer binding protein. Genes Dev 1989;3:1146–56. 3. Antonson P, Xanthopoulos KG. Molecular clon- ing, sequence, and expression patterns of the human gene encoding CCAAT/enhancer binding protein α (C/EBP α). Biochem Biophys Res Commun 1995;215:106–13. 4. Lin FT, MacDougald OA, Diehl AM, et al. A 30kDa alternative translation product of the CCAAT/enhancer binding protein α message: Transcriptional activator lacking antimitotic activity. Proc Natl Acad Sci U S A 1993;90:9606–10. 5. Nerlov C, Ziff EB. CCAAT/enhancer binding Clin Cancer Res 2009;15(17) September 1, 2009 5306 protein-α amino acid motifs with dual TBP and TFIIB binding ability cooperate to activate transcription in both yeast and mammalian cells. EMBO J 1995;14:4318–28. 6. Pabst T, Mueller BU, Zhang P, et al. Dominantnegative mutations of CEBPA, encoding CCAAT/ enhancer binding protein-α (CEBPA), in acute myeloid leukemia. Nat Genet 2001;27:263–70. 7. Cao Z, Umek RM, McKnight SL. Regulated expression of three C/EBP isoforms during www.aacrjournals.org Downloaded from clincancerres.aacrjournals.org on July 26, 2015. © 2009 American Association for Cancer Research. Published OnlineFirst August 25, 2009; DOI: 10.1158/1078-0432.CCR-08-2941 CEBPA in Human AML adipose conversion of 3T3–1 cells. Genes Dev 1991;5:1538–52. 8. Watkins PJ, Condreay JP, Huber BE, et al. Impaired proliferation and tumorigenicity induced by CCAAT/enhancer binding protein. Cancer Res 1996;56:1063–7. 9. Timchenko NA, Wilde M, Nakanishi M, et al. CCAAT/enhancer binding protein α (C/EBPα) inhibits cell proliferation through the p21 (WAF-1/ CIP-1/SDI-1) protein. Genes Dev 1996;10:804–15. 10. Tenen DG. Disruption of differentiation in human cancer: AML shows the way. Nat Rev Cancer 2003;3:89–101. 11. Koschmieder S, Halmos B, Levantini E, Tenen DG. Dysregulation of the C/EBPα differentiation pathway in human cancer. J Clin Oncol 2009; 27:619–28. 12. Mueller BU, Pabst T. CEBPA and the pathophysiology of acute myeloid leukemia (AML). Curr Opin Hematol 2006;13:7–14. 13. Rosenbauer F, Tenen DG. Transcription factors in myeloid development: balancing differentiation with transformation. Nat Rev Immunol 2007;7:105–17. 14. Rosmarin AG, Yang Z, Resendes KK. Transcriptional regulation in myelopoiesis: Hematopoietic fate choice, myeloid differentiation, and leukemogenesis. Exp Hematol 2005;33:131–43. 15. Zhang DE, Zhang P, Wang ND, et al. Absence of granulocyte colony-stimulating factor signaling and neutrophil development in CCAAT enhancer binding protein α-deficient mice. Proc Natl Acad Sci U S A 1997;94:569–74. 16. Zhang P, Iwasaki-Arai J, Iwasaki H, et al. Enhancement of hematopoietic stem cell repopulating capacity and self-renewal in the absence of the transcription factor C/EBPα. Immunity 2004;21:853–63. 17. Porse BT, Bryder D, Theilgaard-Mönch K, et al. Loss of C/EBPα cell cycle control increases myeloid progenitor proliferation and transforms the neutrophil granulocytic lineage. J Exp Med 2005;202:85–96. 18. Kirstetter P, Schuster MB, Bereshchenko O, et al. Modeling of C/EBPα mutant acute myeloid leukemia reveals a common expression signature of committed myeloid leukemia-initiating cells. Cancer Cell 2008;13:299–310. 19. Gombart AF, Hofmann WK, Kawano S, et al. Mutations in the gene encoding the transcription factor CCAAT/enhancer binding protein α in myelodysplastic syndromes and acute myeloid leukemias. Blood 2002;99:1332–40. 20. Preudhomme C, Sagot C, Boissel N, et al. Favorable prognostic significance of CEBPA mutations in patients with de novo acute myeloid leukemia: a study from the Acute Leukemia French Association (ALFA). Blood 2002;100: 2717–23. 21. Frohling S, Schlenk RF, Stolze I, et al. CEBPA mutations in younger adults with acute myeloid leukemia and normal cytogenetics: prognostic relevance and analysis of cooperating mutations. J Clin Oncol 2004;22:624–33. 22. Bienz M, Ludwig M, Oppliger-Leibundgut E, et al. Risk assessment in patients with acute myeloid leukemia and a normal karyotype. Clin Cancer Res 2005;11:1416–25. 23. Pabst T, Mueller BU. Transcriptional dysregulation during myeloid transformation in AML. Oncogene 2007;26:6829–37. 24. Miller M, Shuman JD, Sebastian T, et al. Structural basis for DNA recognition by the basic region leucine zipper transcription factor CCAAT/enhancer-binding protein α. J Biol Chem 2003;278:15178–84. 25. Bullinger L, Dohner K, Bair E, et al. Use of gene-expression profiling to identify prognostic www.aacrjournals.org subclasses in adult acute myeloid leukemia. N Engl J Med 2004;350:1605–16. 26. Marcucci G, Maharry K, Radmacher MD, et al. Prognostic significance of, and gene and microRNA expression signatures associated with, CEBPA mutations in cytogenetically normal acute myeloid leukemia with high-risk molecular features: a Cancer and Leukemia Group B Study. J Clin Oncol 2008;26:5078–87. 27. Hackanson B, Bennett KL, Brena RM, et al. Epigenetic modification of CCAAT/enhancer binding protein α expression in acute myeloid leukemia. Cancer Res 2008;68:3142–51. 28. Keeshan K, He Y, Wouters BJ, et al. Tribbles homolog 2 inactivates C/EBPα and causes acute myelogenous leukemia. Cancer Cell 2006; 10:401–11. 29 . Wouters BJ, Löwenberg B, ErpelinckVerschueren CA, et al. Double CEBPA mutations, but not single CEBPA mutations, define a subgroup of acute myeloid leukemia with a distinctive gene expression profile that is uniquely associated with a favorable outcome. Blood 2009;113:3088–91. 30. Smith ML, Cavenagh JD, Lister TA, Fitzgibbon J. Mutation of CEBPA in familial acute myeloid leukemia. N Engl J Med 2004;351:2403–7. 31. Sellick GS, Spendlove HE, Catovsky D, et al. Further evidence that germline CEBPA mutations cause dominant inheritance of acute myeloid leukemia. Leukemia 2005;19:1276–8. 32. Nanri T, Uike N, Kawakita T, et al. A pedigree harbouring a germ-line N-terminal C/EBPα mutation and development of acute myeloblastic leukemia with a somatic C-terminal C/EBPα mutation. Blood 2006;108:543a [abstr]. 33. Pabst T, Eyholzer M, Haefliger S, et al. Somatic CEBPA mutations are a frequent second event in families with germline CEBPA mutations and familial acute myeloid leukemia. J Clin Oncol 2008;26:5088–93. 34. Renneville A, Mialou V, Philippe N, et al. Another pedigree with familial acute myeloid leukemia and germline CEBPA mutation. Leukemia 2009;23:804–6. 35. Pabst T, Mueller BU, Harakawa N, et al. AML1ETO downregulates the granulocytic differentiation factor CEBPA in t(8;21) myeloid leukemia. Nat Med 2001;7:444–51. 36. Helbling D, Mueller BU, Timchenko NA, et al. The leukemic fusion gene AML1–1-EVI1 suppresses CEBPA in acute myeloid leukemia by activation of calreticulin. Proc Natl Acad Sci U S A 2004;101:13312–7. 37. Helbling D, Mueller BU, Timchenko NA, et al. CBFB-SMMHC is correlated with increased calreticulin expression and suppresses the granulocytic differentiation factor CEBPA in AML with inv(16). Blood 2005;106:1369–75. 38. Skokowa J, Cario G, Uenalan M, et al. LEF-1 is crucial for neutrophil granulocytopoiesis and its expression is severely reduced in congenital neutropenia. Nat Med 2006;12:1191–7. 39. Chim CS, Wong ASY, Kwong YL. Infrequent hypermethylation of CEBPA promoter in acute myeloid leukaemia. Br J Haematol 2002;119: 988–90. 40. Figueroa ME, Wouters BJ, Skrabanek L, et al. Genome-wide epigenetic analysis delineates a biologically distinct immature acute leukemia with myeloid/T-lymphoid features. Blood 2009; 113:2795–804. 41. Wouters BJ, Jordà MA, Keeshan K, et al. Distinct gene expression profiles of acute myeloid/ T-lymphoid leukemia with silenced CEBPA and mutations in NOTCH1. Blood 2007;110:3706–14. 42. Akasaka T, Balasas T, Russell LJ, et al. Five members of the CEBP transcription factor 5307 family are targeted by recurrent IGH translocations in B-cell precursor acute lymphoblastic leukemia (BCP-ALL). Blood 2007;109:3451–61. 43. Chapiro E, Russell L, Radford-Weiss I, et al. Overexpression of CEBPA resulting from the translocation t(14;19)(q32;q13) of human precursor B acute lymphoblastic leukemia. Blood 2006; 108:3560–3. 44. Timchenko LT, Iakova P, Welm AL, et al. Calreticulin interacts with C/EBPα and C/EBPβ mRNAs and represses translation of C/EBP proteins. Mol Cell Biol 2002;22:7242–57. 45. Ross SE, Radomska HS, Wu B, et al. Phosphorylation of C/EBPα inhibits granulopoiesis. Mol Cell Biol 2004;24:675–86. 46. Radomska HS, Basseres DS, Zheng R, et al. Block of CEBPA function by phosphorylation in acute myeloid leukemia with FLT3 activating mutations. J Exp Med 2006;203:371–81. 47. Geletu M, Balkhi MY, Peer Zada AA, et al. Target proteins of C/EBPαp30 in AML: C/EBPαp30 enhances sumoylation of C/EBPαp42 via up-regulation of Ubc9. Blood 2007;110:3301–9. 48. Parkin SE, Baer M, Copeland TD, et al. Regulation of CCAAT/enhancer binding protein (C/EBP) activator proteins by heterodimerization with C/ EBPγ (Ig/EBP). J Biol Chem 2002;277:23563–72. 49. McFie PJ, Wang GL, Timchenko NA, et al. Identification of a co-repressor that inhibits the transcriptional and growth-arrest activities of CCAAT/enhancer-binding protein α. J Biol Chem 2006;281:18069–80. 50. Ceseña TI, Cui TX, Subramanian L, et al. Acetylation and deacetylation regulate CCAAT/enhancer binding protein β at K39 in mediating gene transcription. Mol Cell Endocrinol 2008;289:94–101. 51. Zhang J, Wilkinson JE, Gonit M, et al. Expression and sub-cellular localization of the CCAAT/ enhancer binding protein α in relation to postnatal development and malignancy of the prostate. Prostate 2008;68:1206–14. 52. Truong BTH, Lee YJ, Lodie TA, et al. CCAAT/ enhancer binding proteins repress the leukemic phenotype of acute myeloid leukemia. Blood 2003;101:1141–8. 53. Lee YJ, Jones LC, Timchenko NA, et al. CCAAT/enhancer binding proteins α and ε cooperate with all-trans retinoic acid in therapy but differ in their antileukemic activities. Blood 2006;108:2416–9. 54. Mueller BU, Pabst T, Fos J, et al. ATRA resolves the differentiation block in t(15;17) acute myeloid leukemia by restoring PU.1 expression. Blood 2006;107:3330–8. 55. Rowley JD, Golomb HM, Dougherty C. 15/17 translocation, a consistent chromosomal change in acute promyelocytic leukaemia. Lancet 1977; 1:549–50. 56. Chen GQ, Shi XG, Tang W, et al. Use of arsenic trioxide (As2O3) in the treatment of acute promyelocytic leukemia (APL): 1,As2O3 exerts dose-dependent dual effects on APL cells. Blood 1997;89:3345–53. 57. Zhou Y, Du W, Koretsky T, et al. TAT-mediated intracellular delivery of NPM-derived peptide induces apoptosis in leukemic cells and suppresses leukemogenesis in mice. Blood 2008; 112:2474–83. 58. Miyoshi H, Smith KA, Mosier DE, et al. Transduction of human CD34+ cells that mediate long-term engraftment of NOD/SCID mice by HIV vectors. Science 1999;283:682–6. 59. Koschmieder S, D'Alo F, Radomska H, et al. CDDO induces granulocytic differentiation of myeloid leukemic blasts through translational up-regulation of p42 CCAAT enhancer binding protein α. Blood 2007;110:3695–705. Clin Cancer Res 2009;15(17) September 1, 2009 Downloaded from clincancerres.aacrjournals.org on July 26, 2015. © 2009 American Association for Cancer Research. Published OnlineFirst August 25, 2009; DOI: 10.1158/1078-0432.CCR-08-2941 Complexity of CEBPA Dysregulation in Human Acute Myeloid Leukemia Thomas Pabst and Beatrice U. Mueller Clin Cancer Res 2009;15:5303-5307. Published OnlineFirst August 25, 2009. Updated version Cited articles Citing articles E-mail alerts Reprints and Subscriptions Permissions Access the most recent version of this article at: doi:10.1158/1078-0432.CCR-08-2941 This article cites 59 articles, 37 of which you can access for free at: http://clincancerres.aacrjournals.org/content/15/17/5303.full.html#ref-list-1 This article has been cited by 5 HighWire-hosted articles. Access the articles at: http://clincancerres.aacrjournals.org/content/15/17/5303.full.html#related-urls Sign up to receive free email-alerts related to this article or journal. To order reprints of this article or to subscribe to the journal, contact the AACR Publications Department at [email protected]. To request permission to re-use all or part of this article, contact the AACR Publications Department at [email protected]. Downloaded from clincancerres.aacrjournals.org on July 26, 2015. © 2009 American Association for Cancer Research.