Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
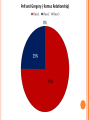
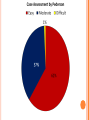
INCIDENCE OF MANDIBULAR NERVES DAMAGE FOLLOWING OF THE LOWER WISDOM TOOTH REMOVAL IN USIM CLINIC Supervisor: Dr John Chong Keat Hon Group members: Nurfarhana Mohd Yusop 1080042 Siti Nur Farhanah Mohd Desa 1080055 RESEARCH BACKGROUND Third molar or wisdom tooth is the most common tooth to be impacted1. Impacted wisdom tooth has been associated with pathological changes to the tooth and its supporting structure2. The problematic impacted wisdom tooth can be managed either conservatively or alternatively removed by surgical extraction3. The complications following surgical removal of lower wisdom teeth may vary from alveolar osteitis, infections, haemorrhage, nerve injury and mandibular fracture4. In this study, we aim to obtain data on the incidence of nerve injury following surgical removal of lower wisdom tooth and the related contributing factors namely anatomical and operative variables5, 6. OBJECTIVES General objective: To determine the incidence of nerve injury following surgical removal of impacted mandibular third molars in USIM dental clinic. Specific objectives: To assess the incidence of nerve injury of the lingual and inferior alveolar nerves (temporary/permanent) following surgical removal of lower wisdom teeth. To assess the operators’ experience in relation to nerve injury during surgical removal of wisdom teeth. To assess the relationship between wisdom teeth’s anatomical position and the nerve injury during surgical removal. METHODOLOGY Study design: retrospective study involving patients that had undergone surgical removal of lower wisdom teeth in USIM dental clinic from June 2011 until December 2012, n=37 Research tools and data collection procedure: Patient’s folders Orthopantomogram radiographs (OPG) Patient’s folder: to determine the patient’s gender, the operator whom conducted the surgery and the presence of nerve injury following surgical removal of lower wisdom tooth OPG: to determine the classification of impacted wisdom tooth and its relationship to inferior alveolar nerve (IAN) Winter’s classification Pell and Gregory classification Risks of IAN injury Pederson scale Statistical analysis: Data were analyzed by using Statistical Package for Social Sciences (SPSS) version 20.0. RESULTS DISCUSSION From the collected data, it was shown that there is no nerve injury recorded following surgical removal of the lower wisdom teeth during the retrospective study from June 2011 to December 2012. One of the limitations in this study is that the sample that we obtained from June 2011 until December 2012 in USIM dental clinic was small which is merely 37 samples. Even though the number of patients who are indicated for surgical removal of wisdom tooth are increasing, some of the patients’ appointments cannot be arranged as they had already undergone the treatment elsewhere. Poor record keeping by the operator is also one of the limitations as there is incomplete information recorded in the patients’ folders. There were also some patients that are unable to be recalled for review following surgery thus there is no information gained regarding the nerve injury. Our recommendation is to have a bigger sample size for the future research. Poor recording should be rectified and folder checking should be more vigilant. Operators should record the presence or absence of the signs and symptoms of nerve injuries. The importance of keeping a good record for future references and medico-legal purposes should be emphasized. Regarding to the insufficient data keeping of the operators, we suggested a questionnaire is to be attached with consent form for assessment of lingual and inferior alveolar nerve. The questionnaire that we suggested is the modification of neurosensory questionnaire11. It will be used to interview the patient one week after the surgical procedure either during recall visit or by phone call. If altered sensation presence in any parts of the mouth, the questionnaire will be repeated after a month. QUESTIONNAIRE11 Do you feel a tingling sensation/numbness on the tongue? - YES Can you differentiate the temperature of food and beverages on each side? - YES - NO Do you feel a tingling/numbness on the chin (on the side of the surgery? - YES - NO Do you feel a tingling sensation/numbness on the lower lips (on the side of surgery)? - YES - NO Have you experienced any altered taste sensation? - YES - NO - NO Do you feel a tingling/numbness on the gum (on the side of the surgery)? - YES - NO CONCLUSION Based on the collected data, there is no incidence of nerve injury following surgical removal of wisdom tooth in USIM dental clinic from June 2011 to December 2012. The small sample in this survey made the assessment of the three operators’ experiences on surgical removal of lower wisdom teeth become unnoticeable. In this retrospective study, there is no differences between the anatomical position of the lower wisdom teeth to the incidence of nerve injury. REFERENCES 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. Impacted tooth [Internet]. [updated 2012 May 4; cited 2012 June 8]. Available from: http://www.nlm.nih.gov/medlineplus/ency/article/001057.htm Interventions for treating asymptomatic impacted wisdom teeth in adolescents and adults [Internet]. 2008 Oct 8. [updated 2005 Feb 6; cited 2012 June 8]. Available from: http://onlinelibrary.wiley.com/doi/10.1002/14651858.CD003879.pub2/abstract Ministry of Health. Management of Unerupted and Impacted Third Molar Teeth. Malaysia; Dec 2005. 23 p. Report No.: MOH/P/PAK/107.05 (GU) Cankaya AB, Erdem MA, Cakarer S, Cifter M, Oral CK. Iatrogenic Mandibular Fracture Associated with Third Molar Removal. International Journal of Medical Sciences. 2011; 8(7): 547-553. Bui CH, Seldin EB, Dodson TB. Types, Frequencies, and Risk Factors for Complications after Third Molar Extraction. Journal of Oral and Maxillofacial Surgery. 2003; 61: 1379-1389. Carmichael FA, McGowan DA. Incidence of Nerve Damage Following Third Molar Removal: A West of Scotland Oral Surgery Research Group Study. British Journal of Oral and Maxillofacial Surgery. 1992; 30: 78-82. Jaffar RO, Tin-Oo MM. Impacted Mandibular Third Molars among Patients Attending Hospital Universiti Sains Malaysia. Archives of Orofacial Sciences. 2009; 4(1): 7-12. Garcia AG, Sampedro FG, Rey JG, Vila PG, Martin MS. Pell–Gregory classification is unreliable as a predictor of difficulty in extracting impacted lower third molars. British Journal of Oral and Maxillofacial Surgery. 2000; 38: 585-587. Rood JP, Shehab BAAN. The Radiological Prediction of Inferior Alveolar Nerve Injury during Third Molar Surgery. British Journal of Oral and Maxillofacial Surgery. 1990; 28: 20-25. Diniz-Freitas M, Lago-Mendez L, Gude-Sampedro F, Somoza-Martin JM, Gandara-Rey JM, GarciaGarcia A. Pederson scale fails to predict how difficult it will be to extract lower third molars. British Journal of Oral and Maxillofacial Surgery. 2007; 45: 23-26. Ridaura-Ruiz L, Figueiredo R, Valmaseda-Castellon E, Berini-Aytes L, Gay-Escoda C. Sensibility and Taste Alteration After Impacted Lower Third Molar Extractions. A Prospective Cohort Study. Med Oral Patol Oral Cir Bucal. 2011. doi: 10.4317/medoral.17890.