Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
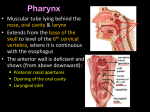
Gross: 8:00 - 9:00 Scribe: Taylor Nelson Thursday, February 26, 2009 Proof: Chaz Capra Dr. Salter Pharynx, Craniovertebral Joints and Prevertebral Region Page 1 of 4 I. Pharynx: Median Section [S2] a. The pharynx exists from the base of the skull down to the inferior level of the cricoids cartilage b. 15 cm long tube connecting inferiorly to the oesophagus c. 5 cm wide superiorly, narrows down to 1.5 cm as it junctions with the esophagus (most narrow point of the entire alimentary canal) d. [S4] Subdivisions of the pharynx: i. Nasopharanyx – vertical boundaries are the base of the skull and posterior aspect of the soft palate ii. Oropharynx – vertical boundaries are the uvula and the epiglottis iii. Laryngopharynx, sometimes called the hypopharynx because it is the inferior part of the pharynx – vertical boundaries are the epiglottis and the cricoids cartilage 1. [S5] Subdivisions are related to cavities anteriorly and this is where they get their names – nasopharynx is related to the nasal cavity anteriorly, oropharynx is related to the oral cavity anteriorly, and the laryngopharynx is related to the larynx anteriorly II. Walls of Pharynx – in the form of four layers [S6] a. Wall of the pharynx consists of four layers, form internal to external: i. Mucosa – including the palatine tonsil ii. Submucosa – synonymous with the pharyngobasilar fascia iii. Muscle iv. Fascial layer – external to the pharynx, called the buccopharyngeal fascia b. [S7] Cross section of the oral cavity displaying the four layers of the pharynx i. Mucosa includes the palatine tonsil ii. Submucosa includes the pharyngobasilar fascia which allows you to remove the tonsil by simply scooping it out of the bed of fascia iii. Muscular layer is external to the submucosa iv. Pharyngobasilar fascia forms the anterior boundary of the retropharyngeal space c. [S8] Muscular coat of the pharynx in the posterior view, buccolaryngeal layer has been removed i. submucosa extends superiorly as the pharyngobailar fascia to fill the space void of muscle at the base of the skull ii. in lab we’ll use scissors to cut this muscle layer and expose the posterior aspect of the pharyhnx iii. [S9] when we cut open the posterior wall of the pharynx we’ll be looking at the anterior relationships 1. the nasal cavity, the oral cavity, and the laryngeal cavity iv. [S10] Pharynx: Opened Posterior View 1. Posterior nares, or posterior opening of the nose is called the choanae, just the connection between the nose and the pharanyx 2. Soft palate and uvula are also depicted, uvula can be bifid because it is the last part of the palate to close embryologically 3. The opening to the larynx is called the aditus III. Characteristics of each of the three part of the pharynx [S11] a. [S12] Nasopharynx (mucosa intact) i. Pharyngeal isthmus is a connection between the nasopharynx and the oropharynx ii. In the roof of the nasopharynx at the midline there is a pharyngeal tonsil (called adenoid when enlarged), may extend laterally and cover the orifice of the Eustachian tube leading to potential for otitis media (infection of the middle ear) iii. Can see the orifice for the auditory tube (also called the Eustachian tube, pharyngeal tympanic tube) iv. Torus tubarius is an elevation produced by the medial end of the Eustachian tube v. Fold of tissue coming down from the torus tubarius and extending into the pharynx itself is known as the salpingopharyngeal fold (salpingo refers to tube) vi. Pharyngeal recess – deep recess extends laterally, located just posterior to the torus tubarius and Eustachian tube, important because cancer can develop in this area, if there is infection in this area it is very close to the lateral pharyngeal space which is confluent with the retropharyngeal space and the infection can potentially travel to the media stinum b. [S13] Nasopharynx – with mucosa removed i. Can see the cartilaginous portion of the medial end of the Eustachian tube called the torus tubarius ii. Two muscles associated with the Eustachian tube, both of which have been implicated in closing and opening the Eustachian tube: 1. Tensor (veli) palatine – tensor of the palate, located anterior and lateral to the levator palatine, cannot close the tube if there is a split/cleft palate 2. Levator (veli) palatine – forms an elevation in the floor of the Eustachian tube – VERY IMPORTANT Gross: 8:00 - 9:00 Scribe: Taylor Nelson Thursday, February 26, 2009 Proof: Chaz Capra Dr. Salter Pharynx, Craniovertebral Joints and Prevertebral Region Page 2 of 4 iii. Salpingopharyngeus muscle lies deep to the salpingopharyngeal fold, part of the longitudinal coat of the third layer of the pharynx c. [S14] Eustachian tube connects the nasopharynx to the middle ear i. Remains open in a cleft palate because the tensor palatine cannot act on a cleft palate ii. In the neonate, the Eustachian tube is wider, shorter, and more horizontal so infection can easily spread to the middle ear iii. Torus tubarius is the medial end of the cartilaginous portion of the Eustachian tube d. [S15] The soft and hard palate act as a partition to separate the nasal cavity and nasopharynx from the oral cavity and oral pharynx i. The hard palate is located anteriorly to the soft palate ii. The soft palate consists of minor salivary glands (these glands are prone to cancer) e. [S16] Oropharynx (mucosa intact) i. Fold of tissue extending from the soft tissue down to the tongue called the palatoglossal fold, muscle deep to this fold called the paltoglossus muscle ii. Fold extending from the soft palate into the pharynx called the palatopharyngeal fold, muscle deep to this fold called the palatopharyngeus muscle iii. Palatine tonsil bed/fossa lies between the palatopharyngeal fold and palatoglossal fold f. [S17] Tonsillar Bed I – with mucosa removed i. Depiction of the pharyngobasilar fascia (sub mucosa) which provides a nice plane that the tonsil can bee scooped out of ii. Palatoglossus lies deep to the palatoglossal fold iii. Palatopharyngeus lies deep to the palatopharyngeal fold iv. Area between the two muscles is the throat or fauces v. [S18] If you remove the pharyngobasilar fascia you can see the true tonsillar bed 1. Superior constrictor muscle forms the tonsillar bed vi. [S19] Tonsillary bed with the inferior part of the superior constrictor removed 1. Muscle called the styloglossus is only seen by virtue of the fact that part of the tonsillar bed has been removed 2. Tonsilar branch of the facial artery – main arterial supply to the tonsillar bed 3. Bbleeding from a tonsilextomy is usually due to lasceration of veins, usually the external palatine (paratonsilar) vein 4. The nerve is the glossopharyngeal nerve which is extending toward the toungue a. Swelling after tonsilextomy can impinge fibers of IX and you may experience temporary loss of taste and general sensations to the posterior 1/3 of the toungue b. Only nerve in the palatine tonsil bed – WILL SEE ON LAB EXAM 5. Muscle with question mark is the styloglossus which is only seen with removal of the tonsillar bed a. [S20] lies lateral to the superior constrictor m., and joins with the hyoglossus m. b. artery that lies deep to the hyoglossus muscle is the lingual artery vii. [S21] palatoglossal fold and palatopharyngeal fold surround the palatine tonsil 1. Lymphoid tissue on the posterior 1/3 of the tongue is called lingual tonsil g. [S22] Laryngopharynx (with mucosa intact) i. Defined from the epiglottis superiorly and the tip end of the cricoids cartilage inferiorly ii. Opening or aditus indicated by green star iii. Aryepiglottic fold forms part of the aditus iv. Piriform recess – important because many cancers can form here, nerve found in this region is the internal laryngeal nerve v. Bulge indicates the location of the cricoids cartilage IV. Muscles of the Pharynx [S23] a. [S24] Three external circular constrictor muscles that constrict in sequence form superior to inferior to propel the bolus of food form the pharynx to the esophagus b. Three internal longitudinal muscles c. [S25] 3 inner longitudinal muscles: i. Salpingopharyngeus m. joins with palatopharyngeus m. ii. Paltopharyngeus m. iii. Stylopharyngeus m. – upper fibers lie external to the constrictor so will only see inferior fibers d. Three external circular muscles i. Superior constrictor, external to the longitudinal muscles ii. Middle constrictor iii. Inferior constrictor Gross: 8:00 - 9:00 Scribe: Taylor Nelson Thursday, February 26, 2009 Proof: Chaz Capra Dr. Salter Pharynx, Craniovertebral Joints and Prevertebral Region Page 3 of 4 1. [S28] The three constrictor muscles are like flower pots stacked on top of one another 2. Insertions of the constrictor muscles occur posteriorly a. Common insertion for all three is termed the midline raphe b. The superior constrictor has an attachment at the base of the skull called the pharyngeal tubercle 3. All of the constrictors have their origins anteriorly a. Superior constrictor – pterygomandibular raphe (extends between the medial plate of the pterygoid process and the mandible) and the bone at either end b. Middle constrictor – stylohyoid ligament and superior surface of the greater horn of the hyoid c. Inferior constrictor – thyroid (origin of the thyropharyngeus portion of the inferior constrictor) and crocoid (cricopharyngeus portion of the inferior constrictor) cartilages 4. Gaps above, below, and between the constrictors a. Gap superior to superior constrictor – pharyngobasilar fascia, which is pierced by the levator palate m. and the auditory tube, is related to this gap b. Gap between the sup. and middle. constrictor – stylopharyngeus m., stylohyoid ligament and IX n. are seen in this gap c. Gap between middle an inferior constrictor – thyrohyoid membrane (pierced by internal laryngeal nerve) lies here d. Gap inferior to inferior constrictor – Most common site for a pharyngeal hernia to occur is a thin wall known as the region of Killian’s dehiscence (lies between the thyropharyngeus portion and the cricopharyngeus portion of the inferior constrictor m. ), recurrent laryngeal nerve is located in this gap as well V. Nerves of Pharynx [S35] a. [S36] Afferent Fibers From Pharynx i. Red represents fibers of the pharyngeal branch of V2 that innervates this area of the pharynx just superior to the Eustachian tube orifice ii. Blue represents the pharyngeal branches of the IX n. which supplies sensory fibers to most of the pharynx iii. Auburn represents the innervation overlap between the internal laryngeal nerve IX n. iv. So you have a sensory overlap of innervations from V2, IX n., and X n. b. [S37] Motor innervations of the pharynx i. Pharyngeal branches of X supply all the muscles of the pharynx but the stylopharyngeus m. 1. If these fibers are disrupted it leads to difficulty with swallowing ii. IX n. is motor to the stylopharyngeus m. iii. Sympathetic fibers supply smooth muscles to the blood vessels iv. Pharyngeal plexus consists of the sensory fibers from IX n. and all of the motor fibers 1. Found on the posterior aspect of the middle constrictor m. VI. Blood Supply and Lymphatics [S38] a. [S39] Remember SALFOPSM i. Ascending pharyngeal a. will be found from a medial view 1. Ascends vertically with the internal carotid a. ii. Ascending palatine branch of the facial artery can also be seen iii. [S40] Pharyngeal veins drain into the internal jugular vein iv. [S41] Pharynx drains into the retropharyngeal lymph nodes which in turn drain into the deep cervical lymph nodes v. [S42] Palatine tonsil drains lymphatically mostly to the jugulodigastric lymph node or tonsillar node VII. Atlanto – Occipital and Atlanto – Axial Jts. [S44] a. [S45] This is C1 through C4 vertebrae stacked together, you see the articulation of the dens with the anterior arch of C1 b. Will discuss the transverse ligament of the atlas which prevents the dens form passing posteriorly and impinging on the spinal cord c. Atlanto – occipital joints – together they act as an ellipsoid joint and permit flexion and extension of the head as well as lateral flexion d. The median atlanto – axial joint is an important pivot joint e. [S46] Muscles producing movement of the atlanto – occipital joints i. Rectus capitis anterior and longus capitis – flexion ii. Sternocleidomastoid – flexion iii. Supra and infrahyoid muscles – flexion iv. [S47] rectus capitis posterior major, rectus capitis posterior minor, superior oblique of head – Extension Gross: 8:00 - 9:00 Thursday, February 26, 2009 Dr. Salter Pharynx, Craniovertebral Joints and Prevertebral Region Scribe: Taylor Nelson Proof: Chaz Capra Page 4 of 4 VIII. Internal Craniocervical Ligaments [S48] a. After the spinal cord has been removed you can see a continuation of the posterior longitudinal ligament which continues superiorly as the tectorial membrane b. If the tectorial membrane is removed you will see the cruciate ligament which consists of 3 parts: a superior and inferior band (neither of which we need to worry about) and a transverse ligament of atlas (important to know this portion of the cruciate) c. Alar ligaments run from the dens to the margin of the foramen magnum d. [S49] If one is hung one may fracture the axis at the pars inter-articularis (know where this is in reference to the axis) IX. [S50] a. Originally there were 8 cervical sympathetic ganglia, one associated with each cervical spinal nerve, but theses gaglia coalesced into 3 (4) ganglia; therefore, these remaining cervical sympathetic ganglia were left to send postsynaptic fibers (via GRC) to several spinal nerves each b. [S51] Location of the sympathetic trunk i. Located posterior to the carotid sheath on the prevertebral fascia ii. Inferior cervical ganglion is joined with the superior thoracic ganglion 82% of the time and this combined ganglion known as the stellate ganglion iii. Refer to GRC that associate the ganglia with the ventral rami X. Overview of Sympathetics to Head [S52] a. Sympathetic fibers get into the head via the internal and external carotid nerve b. Lateral horns of cord levels T1-L2, preganglionic fibers enter the sympathetic trunk, preganglionic axons ascend, pos ganglionic fibers pass into the external and internal carotid nerve, and then they extend to the target tissue where they are involved in vasoconstriction, dilate the pupils, and stimulate sweat glands c. [S53,54] consider sympathetic fibers to the cervical viscera i. Sympathetic fibers to the neck viscera, eg. the pharynx, would ascend as presynaptic fibers to reach the cervical sympathetic ganglia, synapse would then occur, and postsynaptic fibers would pass to the viscera via direct branches or via the blood vessels. [End @ 54:13] Note: The lecture continued for approximately three more minuets with lab instructions, this portion of the lecture was not transcribed.