Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
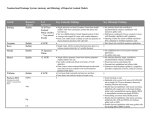
Epiphora Definition overflow of tears Causes 1. oversecretion a. reflex tearing i. infections ii. corneal irritation – trichiasis, foreign bodies b. supranuclear – emotions c. infranuclear – aberrant nerve regeneration (crocodile tears) 2. reduction in drainage a. functional – poor lacrimal pump function (displaced punctum, eyelid laxity, weak orbicularis, CN VII palsy) b. anatomical i. congenital ii. acquired 1. primary (PANDO)– NL duct obstruction caused by inflammation or fibrosis of unknown cause 2. secondary (SALDO) – infection, neoplastic, traumatic and mechanical Anatomy Lacrimal draining system consists of: 1) upper drainage system – puncta and canaliculi 2) lower drainage system – nasolacrimal sac and duct Puncta both directed posteriorly upper lies more medial Canaliculi 1) 2mm vertical component 2) 8mm horizontal 3) Lower slightly longer 4) In most cases, horizontal component merges to form common canaliculus 5) Small mucosal flap (valve of Rosenmuller) separates common canalicular opening from nasolacrimal sac to prevent tear reflux Nasolacrimal sac 6) Common duct enters the sac at the fundus 3.5mm below the apex 7) The sac is separated from the middle meatus of the nasal cavity via the lacrimal bone and frontal process of the maxilla. Nasolacrimal duct 8) opening of the duct in the inferior meatus is protected by a mucosal fold, known as the valve of Hasner, whose function is to prevent air and other nasal contents from entering, especially when the nose is blown. Physiology Jones model with blinking, the superior and deep heads (Horner’s muscle) of the orbicularis contract forcing the puncta to move medially, the canaliculi to shorten and compression of the lumen of the canaliculi. contraction of the deep heads of the pre-septal portion causes the nasolacrimal sac to expand. The resultant negative pressure allows the tears to flow from the common canaliculus into the sac. On eyelid opening, the canaliculi expand and lengthen and the sac collapses following relaxation of the orbicularis muscles. Positive pressure is now induced, forcing the tears to flow down the nasolacrimal duct into the nose Management Epiphora due to lacrimal hypersecretion is never an indication for surgery on the lacrimal excretory system. Resection of the lacrimal gland or severance of its ducts or efferent nerve supply to decrease secretion is condemned because of the risk of keratitis sicca. Acute trauma Many authors contend that the superior canaliculus is of little or no importance in tear drainage, and repair of an injury to the upper canaliculus is unnecessary With 1 canaliculus not repaired, >75% will have no symptoms Others argue that there is no way to predict who will, so repair them all Repair best undertaken within first 2-5 days Established Obstruction Nonsurgical Generally not successful for obstructive systems Digital massage Antibiotics Surgical 1. Punctal repositioning (if has medial ectropion) 2. Canaliculaplasty - strictures of the punctum i. Externalizing the residual lower canaliculus in an -ostomy-type procedure possible even when the residual canaliculus is only one-fourth of the normal canalicular length ii. Conjunctivodacryocystostomy o moving the fundus of the tear sac anteriorly and approximating it to the conjunctiva disrupts the lacrimal pump mechanism and often ends in failure. iii. Conjunctivodacryocystorhinostomy o Indicated in cases of flaccid canaliculi, paralysis of lacrimal pump, absence or obliteration of canaliculi, proximal obstruction o Pyrex tubes exert capillary traction on tears and keep the ducts patent (conduit between medial conjuctival cul-de-sac and nasal cavity, bypassing canaliculus and NLD) o Although Jones tubes work by capillary action, they should be placed vertically to facilitate tear drainage through gravity. iv. conjunctivorhinostomy. o indicated when the tear sac is absent or has been obliterated. 3. Dacryocystorhinostomy procedure of choice for nasolacrimal duct obstruction approach may be external or endoscopic (usually with laser) Endoscopic laser method Dilatation of the lower punctum was performed and a 20G vitreoretinal probe was inserted in the lower canaliculus and advanced into the nasolacrimal sac. The light was directly visualised endonasally with a 0° rigid nasal endoscope, and the laser energy was delivered The nasal mucosa and lacrimal bone were ablated and the ostium was enlarged anteriory as necessary with a microronguer.